Article Text

Abstract
Police face an increased risk of developing mental health problems, yet reliable estimates of their psychological difficulties remain unknown. This systematic review and meta-analysis estimate the pooled prevalence and risk factors for mental health problems among police personnel worldwide. Three independent reviewers searched 16 databases and screened 11 506 articles published between January 1980 and October 2019. Eligible studies involved at least 100 active police professionals and used validated instruments to ascertain specific mental health problems. Estimates were pooled using random-effects meta-analyses. In total, 60 cross-sectional and seven longitudinal studies, involving 272 463 police personnel from 24 countries met criteria for inclusion. The overall pooled point prevalence was 14.6% for depression (95% CI 10.9% to 18.6%), 14.2% for post-traumatic stress disorder (PTSD; 95% CI 10.3% to 18.7%), 9.6% for a generalised anxiety disorder (95% CI 6.7% to 12.9%), 8.5% for suicidal ideation (95% CI 6.1% to 11.2%), 5.0% for alcohol dependence (95% CI 3.5% to 6.7%) and 25.7% for hazardous drinking (95% CI 19.6% to 32.4%). The strongest risk factor for depression and suicidal ideation was higher occupational stress, and the strongest risk factors for PTSD were higher occupational stress and avoidant coping strategies. Higher levels of peer-support were associated with significantly lower PTSD symptoms. Our findings suggest that the prevalence of mental health problems among police exceeds twice that previously reported in mixed samples of first responders, and is associated with poor social support, occupational stress and maladaptive coping strategies. Without effective intervention, psychological difficulties will remain a substantial health concern among police.
- epidemiology
- psychology
- psychiatry
- post traumatic stress disorder
- public health
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Studies suggest that the prevalence of mental health problems among first responders is higher than the general population.
Most studies on police personnel report elevated levels of post-traumatic stress disorder (PTSD), yet comprehensive estimates for wider mental health problems among police are lacking.
What are the new findings?
Results suggest that around one in four police officers screened positive for hazardous drinking, one in seven met criteria for PTSD and depression, and one in 10 met criteria for an anxiety disorder or suicidal ideation.
Findings indicate that poor social support, higher occupational stress and individuals’ maladaptive coping strategies are strong risk factors for potential mental health problems among police.
How might this impact on policy or clinical practice in the foreseeable future?
Police officers show a substantial burden of mental health problems, emphasising the need for effective interventions and monitoring programmes.
The results support increased funding initiatives for police well-being to match preventative efforts currently offered in other high-risk populations.
Introduction
Police personnel in the UK and USA respond to an estimated 10 to 35 million calls annually,1 2 ranging from mental health crises and violent assaults to the deaths of fellow officers.3 Repeated traumatic exposure in police is associated with an increased risk of developing mental health problems, and represents a substantial public health concern.4–6 The prevalence of post-traumatic stress disorder (PTSD) and depression in police are reported to exceed twice that of the general population (20% vs 7%–9%),7 8 and are linked to poorer quality of life,9 elevated risk of errors,10 aggression,10 cardiac deaths,11 substance misuse,12 absenteeism13 14 and suicide.15
Despite these health risks, reliable estimates on the prevalence and risk factors for psychological difficulties among police remain unknown. Epidemiological estimates range from 0.8% to 41.1% for PTSD,16 17 and from 5% to 43% for alcohol misuse.18 19 Studies on commonly reported risk factors for mental disorders, including prior childhood trauma, being female, younger age and emotional responses, often fail to produce consistent results.20 Instead, most cited estimates rely on indirect data derived from mixed samples of multidisciplinary disaster workers, with little relevance to police. Approximately 600 studies relevant to psychiatric problems among rescue workers have been identified in recent meta-analyses,21–27 with only six independent police samples on PTSD.28–33 Compared with other first responders, police are uniquely exposed to graver interpersonal violence (eg, homicide),28 and negative perceptions by the public and their peers.29 Police-specific studies are, however, limited by small, cross-sectional and non-representative convenience samples of 43 to 300 participants.21 The few existing epidemiological police studies are based on the same sample or department,30 leading to selection bias and limited generalisability across police organisations.
Reliable epidemiological insights into the mental health of police are urgently needed to inform policy and intervention for at-risk personnel. This meta-analysis provides the first comprehensive summary of studies published on the prevalence and risk factors for mental health problems among police worldwide.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses and the Meta-analysis of Observational Studies in Epidemiology guidelines.34 35 The review protocol was published in the PROSPERO registry before full commencement (CRD42018111847).31
Search strategy and study eligibility
We searched MEDLINE, PsycINFO, EMBASE, Web of Science, AMED, CINAHL, PILOTS, SciVerse Scopus, the Cochrane Library, PubMed, ERIC, Global Health Archives, ProQuest Central, OpenGrey and Google Scholar for English, Swedish or German language articles published between 1 January 1980 and 8 October 2019. We used a comprehensive list of search terms developed in consultation with a librarian. Due to their high publication rate of police-related studies, the Journal of Psychiatric Research, Journal of Policing, Journal of Traumatic Stress and Journal of Nervous Mental Diseases were hand-searched along with reference lists of relevant full-text articles and reviews.21–27 Finally, 16 frequently cited police health authors were contacted for additional article recommendations. The last retrieval of studies occurred on 20 October 2019. The complete search strategy is described in online supplementary table S1.
Supplemental material
Three independent researchers (SS, RA and MS) reviewed abstracts, full-text articles and corresponding reference lists using Covidence’s systematic review software.32 Any disagreement over study inclusions between reviewers was resolved by a fourth independent reviewer (JB).
We included studies if they: reported on police-specific data to calculate the point prevalence of a specific mental health problem or its associated risk; used a validated instrument or qualified clinician interview to ascertain psychiatric symptoms; involved a sample size ≥100 participants; were rated as low risk of bias as per the Newcastle–Ottawa Scale (NOS; score: ≥3); reported on the same outcome/risk factor as three other eligible studies; were published in English, Swedish or German; and comprised a peer-reviewed publication. We classified alcohol misuse into two categories of severity: high-risk or hazardous drinking (moderate), and harmful drinking or alcohol dependence (severe), aligning with national guidelines and instrument cut-off scores.33 36 Given the volume of available studies, we excluded studies rated as low in methodological quality to condense between-study heterogeneity and to increase the validity of pooled estimates.
When studies were based on the same sample, we extracted data from all studies and prioritised the highest NOS quality-rated study and then the study with the largest sample size per outcome, minimising bias from non-independent samples.33 Finally, to isolate studies to exposures related to police work and to provide comparable estimates of the overall police population, we excluded case studies, retired personnel, trainees, clinical populations and studies based on electronic health registries.
Data extraction and quality assessments
Using a standardised data extraction form, the three reviewers independently extracted: sample characteristics (eg, sample size, age (mean/range, years), percentage of males); response rate; follow-up time; psychiatric measure and cut-off score; effect sizes (eg, prevalence, odd ratios, Pearson’s r etc); and main type of trauma exposure (event endorsed by >70% of the sample). We requested additional data from 30 authors, 17 of whom replied within the 2-month deadline (57% response rate). The remaining 13 studies were excluded, as no relevant estimates could be ascertained.
The methodological quality and risk of bias of each study were assessed by the three reviewers using a modified version of the NOS.37 38 The NOS assesses three methodological domains: selection (maximum two points, including representativeness of the sample and sample size); comparability (maximum one point, including comparing non-responders with responders); and outcome (maximum two points, including outcome assessment and quality of reported statistics) with a maximum score of five (see online supplementary table S2). Consistent with previous meta-analyses,36 studies were classified as high risk of bias/low quality (score: <3) or low risk/moderate to high quality (score: ≥3).
Data analyses
We pooled prevalence estimates of each outcome using random-effects meta-analyses as per the pre-specified protocol,31 accounting for the observed between-study heterogeneity.39 We also applied the Freeman–Tukey double arcsine transformation to stabilise the variance of each estimate,34 as several estimates were close to zero. The point prevalence was defined as the number of identified cases (per instrument cut-off score) divided by the total number of participants assessed at that same time. If longitudinal studies reported estimates for multiple periods, we used the overall period prevalence.
We pooled correlation estimates on risk factors using random or fixed effects meta-analyses (I2 <50%), based on the inverse‐variance method. The inverse-variance method allowed larger studies with smaller standard errors to carry more weight.35 We also applied the Hartung and Knapp method to ensure greater precision when pooling risk factors with a smaller number of studies (k<4) and high between-study heterogeneity (I2 >50%).40 Extracted correlation effect estimates were converted to the log ORs,41 providing an approximate estimate of the ORs. Any multiple effect estimate presented for the same overall risk factor was averaged and weighted for df. Log ORs were back-transformed into ORs for the convenience of interpretation.
Between-study heterogeneity of estimates was assessed using the I2 statistic (>75%=illustrates substantial heterogeneity), standard χ2 tests and prediction intervals.42 43 To further investigate between-study heterogeneity, estimates were stratified by pre-specified subgroups,31 defined as potential sources of variation when at least four studies were available for each comparator group. The influence of age, sex and year of publication were examined using random-effects meta-regressions. The impact of individual study estimates on the between-study heterogeneity was explored by serially omitting individual studies from the overall estimate. Finally, publication bias was examined using Egger’s test, Begg and Mazumdar's rank test and visually through funnel plots when at least 10 studies were present.42 43 R version 3.6.1 (R Foundation for Statistical Computing) and “meta” package were used to perform all analyses.37 44
Results
Study characteristics
Individual key study characteristics are summarised in online supplementary table S3. In total, 60 cross-sectional and seven longitudinal studies (75 sources),4 5 8 12 18 19 38 45–113 involving 272 463 police personnel from 24 countries met criteria for inclusion (figure 1). Of these, 44 different studies provided estimates on PTSD, 27 studies on depression, 12 studies on alcohol misuse, 11 studies on an anxiety disorder, 10 studies on suicidal ideation and three studies on drug misuse. Most studies were from North America (31 studies, 46%), followed by Europe (19 studies, 28%) and Australia (seven studies, 10%), with a median sample size of 631 (range: 100–1 00 518). The population were primarily male (median percentage: 76%), working within general police duty areas (82%, 55 studies), with a median age of 39.1 years (range: 19–77 years). The majority of studies used self-report questionnaires (61 studies, 91%), whereas six studies used a structured clinical interview (9%) to ascertain psychiatric symptoms.114–116

Flow diagram of the 67 selected studies for this systematic review.
Quality assessment
The overall quality of 30 studies was high (46%; NOS score >3) and 37 studies were of moderate quality (54%; NOS score=3). Four studies were large nationally representative surveys comprising between 3272 and 8581 police personnel from Poland,48 Norway,50 Australia79 and Canada,18 respectively. Individual study methodological quality NOS scores are depicted in online supplementary table S4.
Prevalence of mental health problems
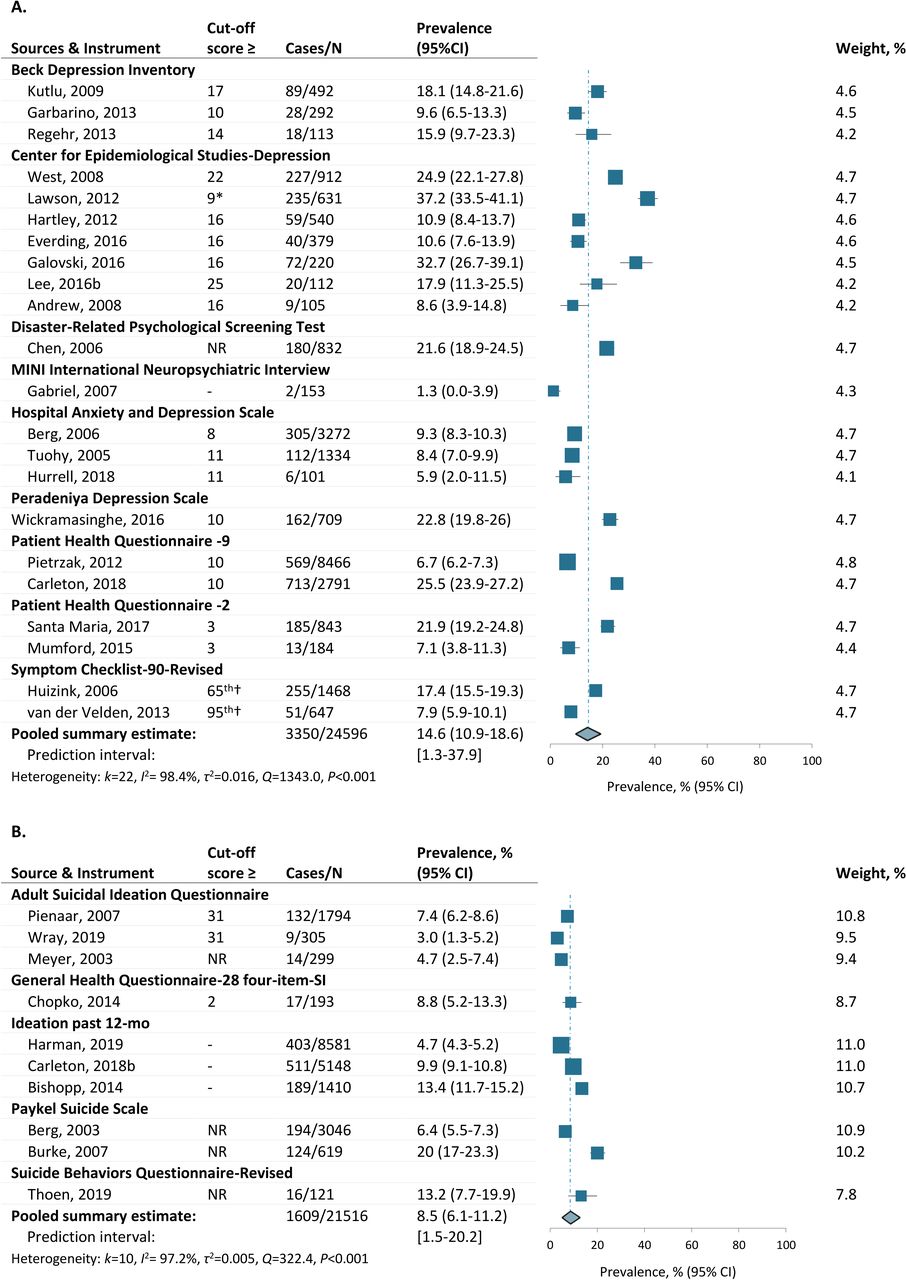
The pooled prevalence estimates were 14.6% for depression or depressive symptoms (95% CI 10.9% to 18.6%, k=22), 14.2% for PTSD or PTSD symptoms (95% CI 10.3% to 18.7%, k=29), 25.7% for hazardous or high-risk drinking (95% CI 19.6% to 32.4%, k=9), 9.6% for a generalised anxiety disorder (95% CI 7.7% to 14.6%, k=10), 8.5% for suicidal ideation (95% CI, 6.1% to 11.2%, k=10) and 5.0% for harmful drinking or alcohol dependence (95% CI 3.5% to 6.7%, k=7). All estimates showed significant between-study heterogeneity (range Q=138.5–3397.2; range I²=95.7%–99.2%; range τ2=0.00–0.026; all P<0.001) but demonstrated moderate variation in terms of predictions intervals (figures 2–4). Three studies also reported on estimates for random drug tests in police (eg, cocaine, marijuana and anabolic steroids).45 88 98 However, the small number of studies and the substantial between-study heterogeneity (prediction interval: 0% to 100%) precluded any reliable meta-analytic pooling (pooled estimates shown in online supplementary figure S2).

Prevalence of PTSD or PTSD symptoms.For each outcome across figures 2-4, studies are stratified by screening instrument alphabetically and ordered by increasing sample size. The area of each square is proportional to the double arcsine estimate. Horizontal lines indicate 95% confidence intervals of the estimate. The dashed line marks the overall summary estimate for all studies. NR, Not reported.

Prevalence of depression or depressive symptoms, and suicidal ideations. *study used the short form of the Center for Epidemiologic Studies Depression. †cut-off score based on the upper percentile of the study sample. NR, Not reported.
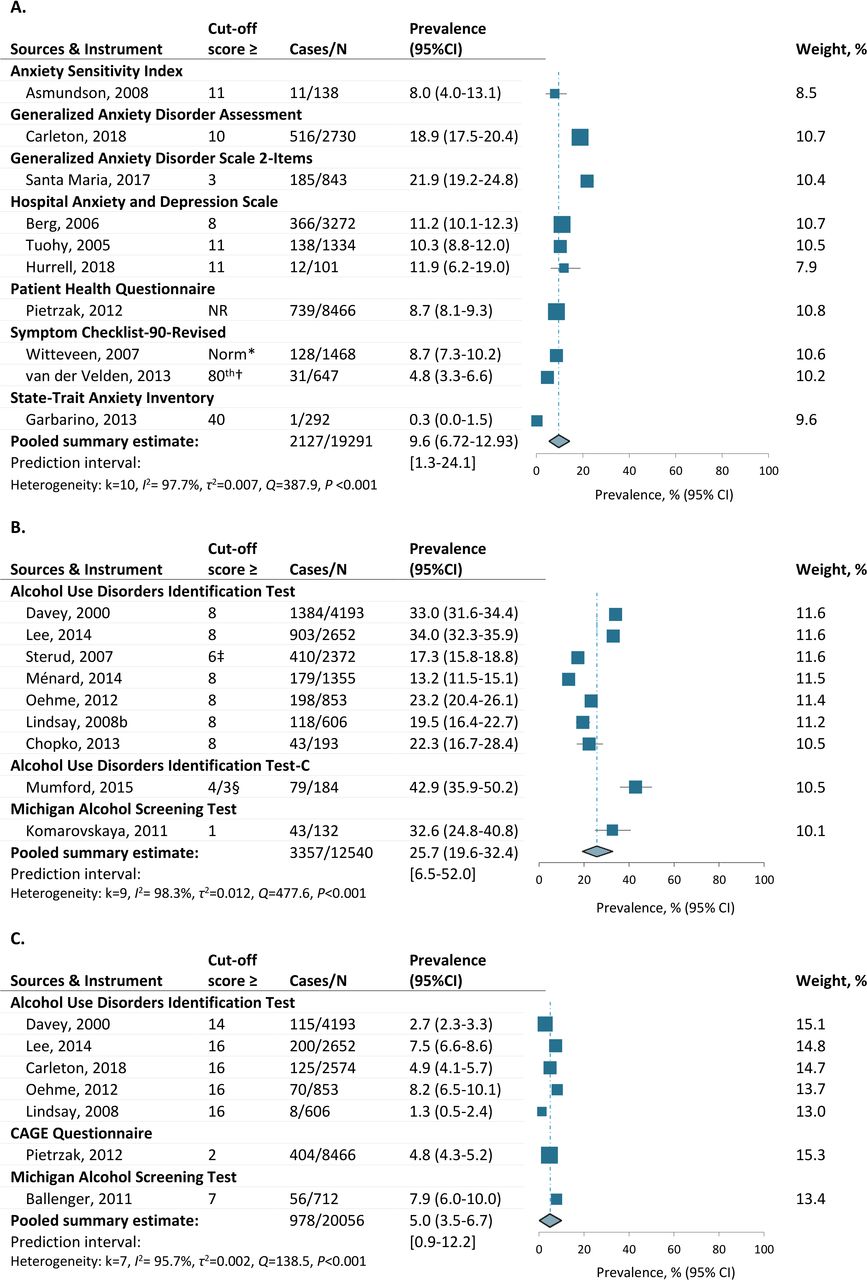
Prevalence of an anxiety disorder or anxiety symptoms, hazardous drinking and alcohol dependence. *cut-off score based on normative table of the general Dutch population. †cut-off score based on the upper percentile of the study sample. ‡Study omitted item "2" from the instrument and therefore used a lower cut-off score. §≥4 cut-off score for males and ≥3 cut-off score for females. NR, Not reported.
Sensitivity analysis of prevalence estimates
Serially omitting each study in separate sensitivity analyses highlighted that no study impacted on the overall prevalence of PTSD, depression, suicidal ideations and alcohol dependence by more than 0.5%. For hazardous drinking and anxiety disorders, exclusion of two studies,8 19 and one study,68 respectively, affected the overall prevalence by more than 1%. No study exclusion markedly affected the between-study heterogeneity (range I²=97.7%–99.2%; P<0.01).
Subgroup analyses of prevalence estimates
Details of each subgroup analysis are provided in online supplementary tables S5 to S6. Overall, we found significantly higher estimates of PTSD in studies from Asia, South America or Africa (21.2%) relative to other continents (range: 7.8%–16.5%), and in studies with police personnel indirectly exposed to dead bodies or severe injuries (24.2%), compared with directly life-threatening events or disasters (prevalence range: 6.9%–16.7%) (test for subgroup differences, all P<0.05).
For depression, we found significantly higher prevalence estimates in studies from Asia, Africa or Australia (24.9%) than studies from Europe (10.6%) or North America (15.0%); in studies with smaller sample sizes (<200 participants) (17.0%) than in larger studies (8.5%); and in studies with lower NOS quality score on the comparability between respondents and non-respondents (17.3%) than in studies with higher NOS score (9.5%). Together, the results suggest that differences in study continent and type of trauma exposure explained some of the between-study heterogeneity observed in PTSD and depression, whereas fewer factors helped explain the variation across other psychiatric conditions.
Meta-regressions of prevalence estimates
In separate meta-regressions, no prevalence estimate was significantly affected by publication year, mean age or studies proportion of males (P>0.05 for all between-group comparisons; online supplementary tables S5 and S6).
Publication bias of prevalence estimates
We found little or no evidence for asymmetry following visual inspections of funnel plots (see online supplementary figures S3–S8), and there was no evidence for small-study effects (Egger’s test range=−0.5 to 4.5, Rank's test range=-23.0 to 9.0, P-values range=0.51–0.79).
Risk factors for mental health problems
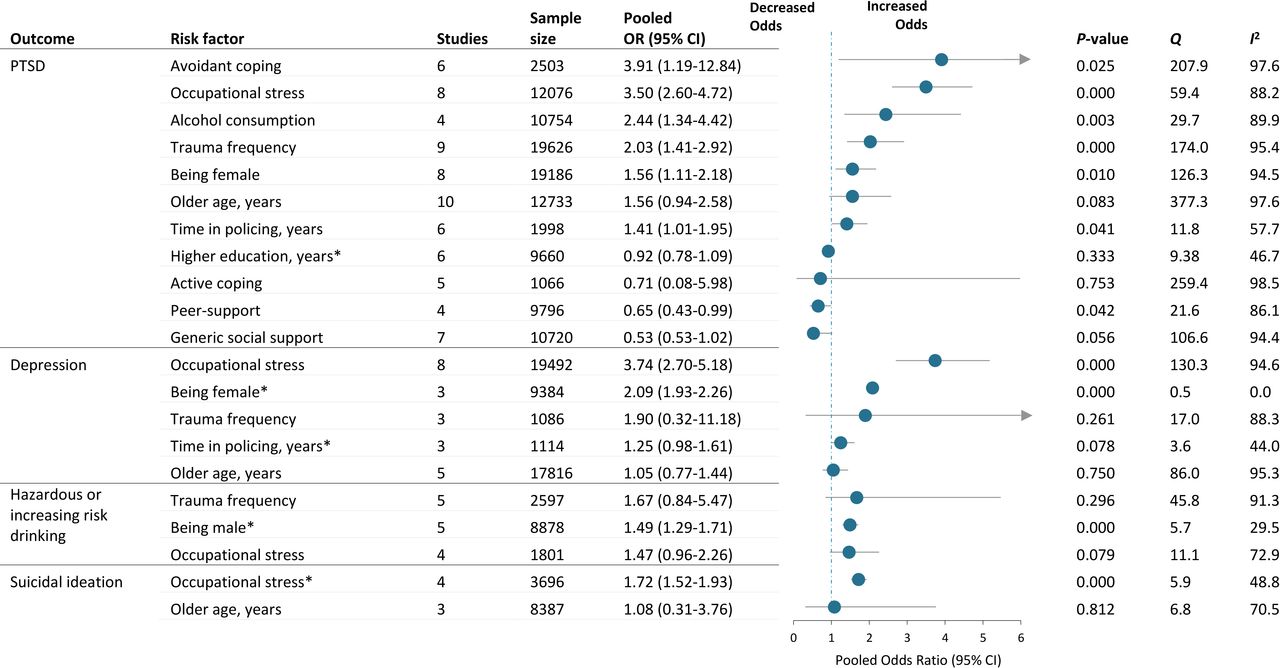
Figure 4 presents the ORs for each pooled risk factor by type of mental health problem, as reported at least three times by 49 different studies. Individual study estimates for each risk factor are presented in figures S7–S10.
Risk factors for PTSD
Pooled data from 30 studies revealed that police PTSD was significantly associated with being female (OR 1.56, 95% CI 1.11 to 2.18, k=8), greater trauma frequency (OR 2.03, 95% CI 1.41 to 2.92, k=9), longer time in policing (OR 1.41 95% CI 1.01 to 1.95, k=6), avoidant coping strategies (OR 3.91, 95% CI 1.19 to 12.84, k=6), higher levels of alcohol consumption (OR 2.44, 95% CI 1.34 to 4.42, k=4) and higher occupational stress (OR 3.50, 95% CI 2.60 to 4.72, k=8) (all P<0.05; figure 4). By contrast, higher levels of peer-support (OR 0.65, 95% CI, 0.43 to 0.99, k=4) was associated with significantly lower PTSD symptoms. There was moderate to substantial between-study heterogeneity across all pooled risk factors (range I 2=46.7%–98.5%; figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled estimates for risk factors of mental health problems among police personnel. Pooled estimates are based on random-effects meta-analyses of the log odds ratio unless otherwise stated. Horizontal lines indicate 95% confidence intervals of the estimate.When overlapped by a confidence interval, the dashed line marks the estimate for no association. *Estimates based on a fixed-effects meta-analysis due to lower between-study heterogeneity.
Risk factors for depression, suicidal ideation and hazardous drinking
Of the 15 studies reporting on depression (figure 5), being female was significantly associated with depressive symptoms (OR 2.09, 95% CI 1.93 to 2.26, k=3), and higher levels of generic occupational stress were significantly associated with both depression (OR 3.74, 95% CI 2.70 to 5.18, k=8) and suicidal ideation (OR 1.72, 95% CI 1.52 to 1.93, k=4). For alcohol misuse, being male was significantly associated with hazardous drinking (OR 1.49, 95% CI 1.29 to 1.71, k=5). The between-study heterogeneity ranged from low to high across all outcomes (range I 2=0.0%–97.6%).
Meta-regressions of risk factors
Meta-regressions revealed that studies with a higher percentage of males were associated with an increased effect of co-worker support on PTSD symptoms (estimate: −0.15, 95% CI −0.23 to −0.08, P=0.012; online supplementary table S7).
Sensitivity analysis of risk factors
Serially omitting individual studies from risk factors with at least five studies illustrated that the strength of the association and the between-study heterogeneity between PTSD, time in policing and avoidant coping varied substantially depending on the study included (P-value range: 0.00–0.12; I2 range=53.5%–98.9%). All other estimates remained generally constant.
Publication bias of risk factors
Publication bias was discerned in studies reporting on the association between age and PTSD (Egger’s test: bias=−6.35, P=0.752; Rank test=23.0, P=0.04). No evidence for publication bias was observed across all other conditions (Egger’s test and Rank’s test P>0.2; see online supplementary figure S13 for funnel plots).
Discussion
Based on data from 272 463 police personnel and 24 countries, we found that about one in four police officers screened positive for hazardous drinking, one in seven globally met criteria for PTSD and depression, and one in 10 met criteria for an anxiety disorder or suicidal ideation. Our findings suggest that the prevalence of mental health problems among police often exceed twice that reported for the general population. Compared with the recent UK Adult Psychiatric Morbidity Survey of the general population (adults aged 16–64 years, n=7546), we found higher estimates in police for PTSD (13.7% vs 4.4%), generalised anxiety disorder (10.9% vs 6.6%), depression (14.6% vs 3.8%), suicidal ideation (9.2% vs 3.3%) and hazardous drinking (25.7% vs 16.6%).117 Contrasted to previous meta-analyses on police, current prevalence estimates also exceeds twice those previously reported for PTSD (14.3% vs 4.7%),21–27 and depression (14.6% vs 7.0%).118 Overall, these findings indicate that previous studies on mixed first responders underestimate the prevalence of mental problems in the wider police population, and illuminate the critical healthcare needs of police worldwide.
Higher occupational stress and being female were the most consistent risk factors for poorer mental health among police, although their effect varied across outcomes. The impact of occupational stressors is broadly consistent with Agnew's general strain theory,119 where repeated negative experiences in the absence of occupational rewards are believed to intensify the strain of smaller police stressors (eg, administration, caseload). The effect of cumulative strain may also hamper the natural resolution of trauma-related psychological difficulties that otherwise would occur over time in less stressful environments.120 As police are unique in carrying firearms and responding to violence, additional stress is posed by negative perceptions from peers and the public,121 along with cultural barriers to help-seeking (ie, stigma).122 Similarly, the large proportion of males and power differences observed between genders in police may put females at a disadvantage of peer support, potentially inferring greater susceptibility to depression and PTSD.122 While based on a modest pool of findings, the consistency across outcomes highlight that organisational risk factors play a central role in the development of mental health problems in police, rather than the job itself.
Avoidant coping strategies and hazardous drinking were associated with a higher risk of PTSD, supporting previous findings in mixed populations.123–125 Maladaptive coping strategies have long been emphasised as unique characteristics of vulnerability to stress, potentially disrupting the memory encoding of traumatic events and increasing PTSD risk.126 However, the cross-sectional nature of the pooled data does not allow for insights into the causal factors of PTSD. Increased avoidance, for example, may be a way of coping with trauma rather than a cause of it. Further longitudinal research on the association between early onset of negative coping strategies and long-term psychiatric conditions are needed.
Limitations
This study has important limitations and estimates should be considered with caution. First, each risk factor was analysed individually, affecting the ability to make assumptions about their contribution to psychiatric conditions when taking into account other risk factors.127 For example, avoidance might contribute differently to the risk of PTSD when taking into account organisational stress. Nonetheless, our estimates still provide valuable insights to facilitate preventive strategies to reduce psychological risks. Further, given the high between-study heterogeneity and limited data available on covariance matrixes, there would have been minimal benefits of applying a multivariate approach.128
Second, the overall between-study heterogeneity across estimates remained substantial and could not be explained by most subgroup analyses. As in most large meta-analyses, several factors not examined in the subgroup and sensitivity analyses (eg, culture, mental health awareness, comorbid conditions) may have influenced the variation in our estimates. For instance, our subgroup analyses highlighted that the prevalence of mental health problems in the police was higher in Asia than other continents. Nonetheless, no large-scale study globally or in the USA provided nationally representative estimates on police for reliable cross-country comparisons. The limitations of this heterogeneity, therefore, reflects that the ‘best available data’ is limited. However, the consistency of our results across larger samples and sensitivity analyses also suggest that estimates are valid and merit further study.
Third, most studies were cross-sectional and outcomes may, therefore, have been caused by non-police-related factors, including prior trauma or military service, or been confounded by lower socioeconomic status.129 130 Still, in an attempt to isolate the link between police-related mental health problems,we only included studies looking at active police personnel. Additionally, with the exception of a handful of studies on police recruits or disaster workers, no large study provided longitudinal estimates on the risk factors for psychiatric disorders in police.
Finally, estimates were mainly obtained using self-report instruments (91%) rather than clinician interviews, with only one identified study using a gold-standard Clinician-Administered Scale (eg, CAPS for PTSD).131 Many studies also lacked details on self-report procedures and we were unable to establish whether PTSD symptoms related to specific events or repeated trauma. However, self-report measures may reflect more accurate estimates than interviews, given their ability to protect anonymity, and the potential stigma of face-to-face questioning among police.122
Implications
Despite these limitations, our findings of increased mental health problems among police illustrate that facilitation of early identification and help-seeking for psychiatric conditions is vital for improving officers’ quality of life. Continuous mental health screenings and psychoeducation throughout a police career could prove beneficial, as opposed to single screenings after large incidents.132 The association between social support, generic occupational stress and decreased psychological difficulties also allude to the benefits of integrating routine peer support and mindfulness training in police departments.133 For instance, positive peer and leader attitudes towards mental health have shown to buffer the negative effects of police trauma and job strain.134 Specific preventative efforts should, therefore, be aimed at minimising negative police cultures via stigma reduction strategies, confidential counselling without supervisory approval, increased employee-assistance programmes and routine psychoeducation.
The limited occupational support is further compounded by inadequate evidence for effective interventions, resulting in a lack of consensus as to what should be offered. To date, two comprehensive Cochrane reviews attest to the inconclusive evidence for police interventions. One review investigated specific police stress intervention studies,135 and the other examined interventions for stress, burnout and job satisfaction across professions.136 Both reviews reported that no intervention study was of adequate quality to include in their synthesis. Another review by the Campbell Collaboration found no evidence for an overall reduction in psychobiological symptoms for police-specific stress interventions.137 Only one high-quality pilot trial, using combined psychopharmacology, has shown potential effectiveness in reducing psychiatric symptoms among mixed first responders.138 Other interventions such as trauma risk management have been studied in pre-post designs and shown limited effectiveness.139 Further research into interventions that address stress and peer support in the police is needed, taking into account risk differences between genders and cultures.
Overall, our results support the increased funding initiative from the US National Institute for Occupational Safety and Health, and the UK government's common goals for increasing police well-being,140 141 to prioritise research on mental health in police and match preventative efforts in other high-risk populations.
Acknowledgments
We are grateful to Dr Brian Chopko (Kent State University), Professor Christine Stephens (Massey University), Professor John Violanti (University at Buffalo), Professor Charles Marmar (New York University), Dr Karoline Ellrich (Criminological Research Institute of Lower Saxony), Professor Karl Peltzer (Human Sciences Research Council Cape Town), Dr Kim Ménard (Penn State Altoona), Marie-Christine Plat (Unversity of Amsterdam), Dr Nicholas Carleton (University of Regina), Professor Paula Brough (Griffith University), Professor Steyn Renier (University of South Africa) and Vincent McNally for providing additional input and data to complete our analyses. We also express our deepest appreciation to the police personnel and their families worldwide for their collaboration with all the research and their service to the public.
References
Supplementary materials
Press release
Footnotes
Contributors Concept: SS, JB. Design: SS. Drafting of the manuscript: SS, RA. Acquisition, analysis or interpretation of data: SS, RA, JB, SR, MS, RJ. Statistical analysis: SS, RJ. Critical revision of the manuscript for important intellectual content: SS, JB, RA, SR, MS, RJ. Study supervision: JB (primary), SR (secondary), RJ (statistical).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.