Article Text

Abstract
We aim to quantitatively synthesise available epidemiological evidence on the prevalence rates of workplace violence (WPV) by patients and visitors against healthcare workers. We systematically searched PubMed, Embase and Web of Science from their inception to October 2018, as well as the reference lists of all included studies. Two authors independently assessed studies for inclusion. Data were double-extracted and discrepancies were resolved by discussion. The overall percentage of healthcare worker encounters resulting in the experience of WPV was estimated using random-effects meta-analysis. The heterogeneity was assessed using the I 2 statistic. Differences by study-level characteristics were estimated using subgroup analysis and meta-regression. We included 253 eligible studies (with a total of 331 544 participants). Of these participants, 61.9% (95% CI 56.1% to 67.6%) reported exposure to any form of WPV, 42.5% (95% CI 38.9% to 46.0%) reported exposure to non-physical violence, and 24.4% (95% CI 22.4% to 26.4%) reported experiencing physical violence in the past year. Verbal abuse (57.6%; 95% CI 51.8% to 63.4%) was the most common form of non-physical violence, followed by threats (33.2%; 95% CI 27.5% to 38.9%) and sexual harassment (12.4%; 95% CI 10.6% to 14.2%). The proportion of WPV exposure differed greatly across countries, study location, practice settings, work schedules and occupation. In this systematic review, the prevalence of WPV against healthcare workers is high, especially in Asian and North American countries, psychiatric and emergency department settings, and among nurses and physicians. There is a need for governments, policymakers and health institutions to take actions to address WPV towards healthcare professionals globally.
- violence
- epidemiology
- risk factors
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Workplace violence (WPV) has been shown to have negative effects on the organisation (eg, staff turnover, higher absenteeism, reduced job commitment and job dissatisfaction), the mental and physical health of healthcare practitioners, and the quality of healthcare delivery.
What are the new findings?
The global prevalence of WPV by patients and visitors against healthcare workers is high, especially in Asian and North American countries, psychiatric and emergency department settings, and among nurses and physicians.
Globally, more experienced healthcare workers, white populations, physicians, nurses, healthcare workers working in urban settings and those working longer hours were more likely to experience non-physical violence.
Men, more experienced healthcare workers, white populations, physicians, nurses, being single/unmarried healthcare workers and those working longer hours were more likely to encounter physical violence.
Key messages
How might this impact on policy or clinical practice in the foreseeable future?
Knowledge of the prevalence of WPV by patients and visitors against healthcare workers and understanding the differences across groups can inform strategies for developing targeted antiviolence campaigns and intervention programmes.
Enacting preventive strategies and providing safer workplace environments for healthcare workers should be urgently prioritised.
In particular, efforts should be targeted at emergency department, mental health and pre-hospital settings.
At the organisation level, measures might include expanding staffing levels to decrease the need for individual practitioners to work extended hours and developing education and training programmes on managing WPV.
Other measures could include increasing public awareness about the negative impacts of WPV on healthcare professionals and enforcing appropriate policies and legislation (eg, encouraging staff to promptly report violent acts and judicial punishment of perpetrators).
Introduction
Workplace violence (WPV) against healthcare workers is a global problem,1 2 as it is a key occupational hazard faced by healthcare professionals worldwide. It is defined as ‘incidents where staff are abused, threatened or assaulted in circumstances related to their work, including commuting to and from work, involving an explicit or implicit challenge to their safety, well-being or health’.3 It includes physical assault, aggression, sexual harassment, bullying, and verbal abuse or threats.4 WPV has been associated with reduced job satisfaction, commitment and efficiency, poor quality of life, as well as increased stress, sleep disruption, burn-out and even death.5–9 In addition, WPV has a negative impact on the retention of healthcare workers and the quality of medical care.10–12
Healthcare workers are the main providers of healthcare services and the foundation of any healthcare system. The efficiency, effectiveness and quality of a nation’s healthcare system are directly associated with the quality and size of its healthcare workforce. Thus, investigating WPV against healthcare staff is of considerable importance. Enhanced understanding of the issue can inform the development of targeted interventions and policies to reduce violence and improve the safety of healthcare staff and quality of care.
The significance of WPV against healthcare workers has been increasingly recognised by decision makers, health professionals and researchers globally. Previous reviews have tended to focus on one particular group of healthcare workers (eg, doctors, nurses or emergency medical service personnel only) and/or specific types of WPV (such as verbal, physical violence or sexual harassment only).13 14 In addition, the existing reviews15 16 have not used quantitative techniques to compute the pooled prevalence rate estimates, or have only partially included relevant studies.17–19 Many more studies have been published recently, which will allow a more precise quantitative analysis of the prevalence rates of WPV against healthcare workers. Importantly, the prevention and control of WPV is not an isolated event and needs to be considered in the context of the whole health system. Previous studies20–23 have shown that gender, occupation, practice settings and work schedules were associated with WPV. These factors may vary across different countries.24–28 At present, it is unknown whether WPV prevalence rates vary across gender, study location, the time of violence occurrence, occupations, practice settings and countries at the global level, and which types of WPV have the highest prevalence and what are the key risk factors associated with WPV. To investigate these questions, we conducted a systematic review of relevant studies on the prevalence of and risk factors for WPV in healthcare workers across the world and investigated the causes of heterogeneity in findings across individual studies.
Methods
This meta-analysis was conducted following the checklist of the Meta-Analysis of Observational Studies in Epidemiology guidelines for the design, analysis and interpretation.29
Search strategy
We conducted a comprehensive search of PubMed, Embase and Web of Science databases from their inception to October 2018 for pertinent studies that reported on WPV prevalence among healthcare workers. The search terms were ‘workplace violence’ or ‘violence’ or ‘assault’ or ‘abuse’ or ‘aggression’ or ‘bullying’ or ‘harassment’ and ‘health care worker’ or ‘health worker’ or ‘health professional’ or ‘health care professional’ or ‘health care provider’ or ‘healthcare worker’ or ‘healthcare professional’ or ‘healthcare provider’ or ‘physician’ or ‘doctor’ or ‘nurse’ or ‘nursing’ or ‘medical staff’. Only articles published in the English language were considered. Additionally, we manually scrutinised the reference lists of retrieved articles for additional pertinent publications.
Inclusion and exclusion criteria
Studies meeting the following criteria were included: (1) the study was of a cross-sectional or cohort study design; (2) the study population was healthcare workers aged ≥18 years; (3) WPV was from external sources (eg, patients, patients’ family or relatives, or visitors); and (4) the study reported prevalence rates of WPV against healthcare workers or provided sufficient information for their calculation. We excluded reviews, essays, conference abstracts, letters and commentaries. When multiple publications from the same study population were identified, we included the publication that presented the most complete information on results or the publication with the largest number of cases.
Data extraction
Relevant data from studies, including authors, year of publication, study/geographical location, sample size, participants’ age (range or mean age at entry) and gender, definitions and measurements of WPV, frequency and type of WPV, prevalence rates, and prevalence period of WPV were extracted on to a data abstraction form purposely designed for this study. WPV included physical violence (physical and sexual assaults) and non-physical violence (verbal abuse, threat and sexual harassment).
Quality appraisal
To assess the quality of included studies, an 11-point scoring system recommended by the Agency for Healthcare Research and Quality was applied for cross-sectional studies.30 This tool comprises three items assessing the quality of participant selection (eg, inclusion/exclusion criteria), five assessing the quality of measurement (eg, source of data, reliability/validity assessment) and three assessing the quality of analysis (eg, management of missing data, confounding). Each item has three choices: ‘yes’, ‘no’ and ‘unclear’. Article quality was evaluated according to the established scoring system: 1 point if the item was considered in the study and 0 point if the item was not considered or we were unable to determine if it had been considered. The score ranges from 0 to 11 points, with a higher score representing higher study quality; ratings are reported in online supplementary eTable 1. All studies were appraised by authors YG and JL. The interobserver agreement (κ) was 0.902.
Supplemental material
Data analysis
Prevalence rates of WPV against healthcare workers were calculated in meta-analysis using the random-effects model. If studies reported results separately by perpetrators of WPV (eg, patients, patients’ family or relatives, or visitors), we included the estimated prevalence rates with the largest cases in the main analysis. For studies that reported results separately by prevalence period of WPV (1-year prevalence and career period prevalence), we included the estimated 1-year prevalence of WPV in the primary analysis. For studies that reported results separately by types of non-physical violence (verbal abuse, threat and sexual harassment), these outcomes were considered as independent reports in the primary and subgroup analyses. To identify the factors associated with prevalence of violence against healthcare workers, pooled ORs for potential influencing factors were calculated with a random-effects model.
Statistical heterogeneity across studies was estimated with the I² statistic, where values of 25%, 50% and 75% represented cut-off points for low, moderate and high degrees of heterogeneity, respectively.31
Subgroup analyses stratified by gender, study location, study period, the World Bank’s income categories, practice setting, work schedules, WPV type and occupation of healthcare workers were conducted to investigate potential sources of heterogeneity between subgroups. Subgroup differences were tested by meta-regression analysis (using STATA V.12.0 ‘metareg’ command).
Potential publication bias was assessed with the Egger’s linear regression test,32 with the results indicating publication bias when p<0.10. All statistical analyses were performed with STATA V.12.0. Except where otherwise specified, p values were two-tailed with a significance level of 0.05.
Results
Study selection
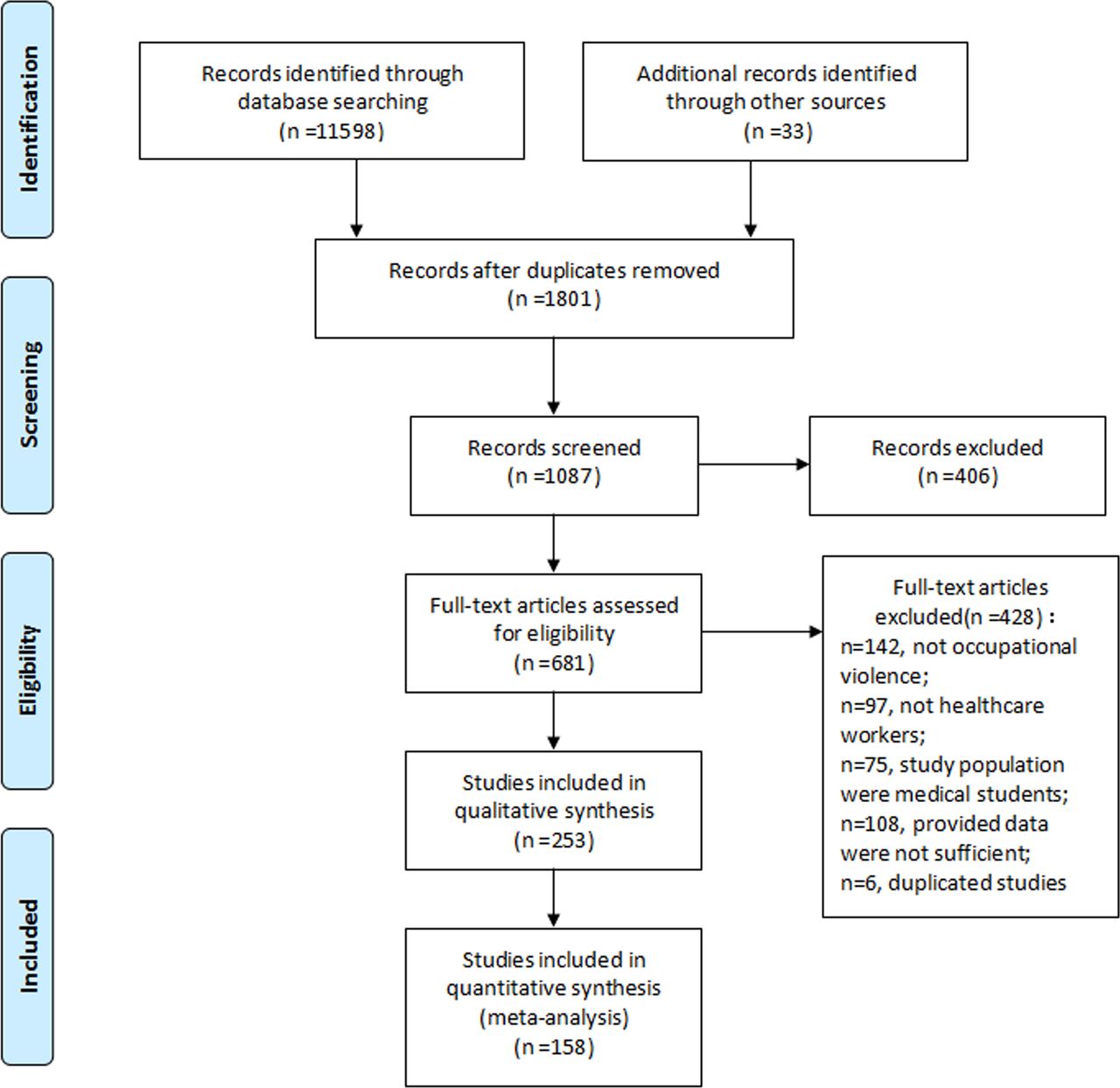
The process of study selection, identification and inclusion using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram is presented in figure 1. Initially, 11 598 articles were retrieved from PubMed, Embase and Web of Science databases. After the initial screening of titles and abstracts, 681 articles were selected for further full-text assessment. After retrieving the full text for detailed evaluation, 253 studies were included in the qualitative analysis and 158 studies were included in the quantitative meta-analysis (12-month prevalence of WPV).

Flow chart of identification of relevant observational studies in relation to workplace violence.
Study characteristics
The main characteristics of the included 253 studies published between 1987 and 2018 are shown in online supplementary eTable 2. Of these 253 studies, 106 were conducted in Asian countries, 54 in North America, 48 in Europe, 27 in Australasia (Australia and New Zealand), 11 in Africa, 3 in Latin America and 4 studies were international collaborations. In total, 217 studies reported results for both men and women combined; 68 studies reported results for men and women separately; 1 study reported results for men only; 18 studies reported results for women only; and 16 studies did not report the gender. The sample size of included studies ranged from 36 to 39 898 (median=380; IQR: 200–903), with a total of 331 544 participants. We included 114 studies that considered any type of WPV prevalence, 217 studies that investigated the prevalence of non-physical violence and 212 studies that assessed physical violence. Verbal abuse was the most common form of non-physical violence considered in the included studies (n=175), followed by threats (n=79) and sexual harassment (n=75); 20 studies reported more than one type of violence. The average quality assessment score of all included studies was 5.3 points. Definitions of WPV varied across studies. Some studies defined WPV according to a response to survey question, and a few studies used definitions provided by the WHO and/or the International Labour Office (online supplementary eTable 3).
More than four in five studies on any type of WPV (95 of 114) were published since 2006. Studies published before 2006 were predominantly conducted in Europe. Studies from Asia, North America and Australasia began to increase after 2006 (figure 2A). More than three-quarters of the reports on non-physical violence (279 of 349) were published since 2006. Studies on non-physical violence published before 2006 were predominantly conducted in North America. Studies on non-physical violence from Asia, Europe and Australasia began to increase after 2006 (figure 2B). More than half of these studies on physical violence (137 of 212) were published since 2010. Studies on physical violence published before 2010 were mainly conducted in Asia and North America. Studies on physical violence from Europe and Australasia began to increase after 2006 (figure 2C).

{kind=link}
{kind=link}
(A) Data for any type of workplace violence set by year and study location. (B) Data for non-physical violence set by year and study location. (C) Data for physical violence set by year and study location. The size of the circle is proportional to the sample size.
The 12-month prevalence of any type of WPV against healthcare workers
In total, 78 studies were included in the analysis to estimate the 12-month prevalence of any type of WPV. Table 1 shows the percentage of WPV reported in the included studies. From the random-effects meta-analysis, a prevalence of 61.9% (95% CI 56.1% to 67.6%) was estimated globally among healthcare workers, with significant heterogeneity across studies (I2 =99.9%, p<0.001).
Proportion of exposure to any type of WPV, non-physical and physical violence: overall estimate and subgroup analysis (12-month prevalence)
For study location, Australasia had the highest prevalence (70.9%; 95% CI 63.9% to 78.0%), followed by North America (67.3%; 95% CI 48.8% to 85.8%), Asia (64.9%; 95% CI 59.6% to 70.2%) and Africa (59.2%; 95% CI 39.8% to 78.6%). Europe had the lowest prevalence of WPV (48.1%; 95% CI 34.6% to 61.6%) (table 1).
Across practice settings, the prevalence was highest in prehospital settings (83.9%; 95% CI 74.4% to 93.4%). Across work schedules, group with mixed shifts had higher prevalence of any form of WPV than day or night shifts (72.8% vs 49.7% vs 39.4%). Across occupations, nurses had the highest exposure to any form of WPV, followed by physicians and other healthcare professionals (59.2% vs 56.8% vs 44.4%) (p=0.02). No significant between-group difference was found for gender and study period (all p>0.05).
In Asian countries, the pooled prevalence of any type of WPV was 77.3% (95% CI 59.6% to 95.1%) in 1990–1999 and decreased to 64.0% (95% CI 58.1% to 69.9%) in 2010–2018. By contrast, there was an increasing trend in Europe (27.2% in 2000–2009 vs 53.0% in 2011–2018) (table 2).
Trends of study period-specific WPV 12-month prevalence across study locations
The 12-month prevalence of non-physical violence against healthcare workers
One hundred and forty studies with 229 reports investigated the 12-month prevalence of non-physical violence. A prevalence of 42.5% (95% CI 38.9% to 46.0%) for non-physical violence was estimated globally among healthcare workers. Substantial heterogeneity was observed (p<0.001; I2 =99.9%). Verbal abuse (57.6%; 95% CI 51.8% to 63.4%) was the most common form of non-physical violence, followed by threats (33.2%; 95% CI 27.5% to 38.9%) and sexual harassment (12.4%; 95% CI 10.6% to 14.2%).
For study location, North America had the highest prevalence (58.7%; 95% CI 46.0% to 71.4%), followed by Asia (45.5%; 95% CI 40.4% to 50.7%), Australasia (38.7%; 95% CI 28.0% to 49.4%), Latin America (36.8%; 95% CI 25.4% to 48.3%), Africa (32.7%; 95% CI 21.5% to 44.0%) and Europe (31.6%; 95% CI 27.1% to 36.1%). Across practice settings, the prevalence of non-physical violence was highest in emergency departments (EDs) (62.3%; 95% CI 53.7% to 70.8%). No significant between-group difference was observed for gender, study period, income category, work schedules and occupation (all p>0.05).
In Australasia, the pooled prevalence of non-physical violence was 31.7% (95% CI 20.4% to 43.1%) in 2000–2009 and increased up to 50.2% (95% CI 30.9% to 69.5%) in 2010–2018. By contrast, there was a decreasing trend in Europe (35.6% vs 29.0%) and North America (90.9% vs 50.1%). The pooled prevalence of non-physical violence was stable in Asian countries (2000–2009: 50.9% vs 2010–2018: 44.5%) (table 2).
The 12-month prevalence of physical violence against healthcare workers
One hundred and thirty-eight studies investigated the 12-month prevalence rate of physical violence. A prevalence of 24.4% (95% CI 22.4% to 26.4%) for physical violence was estimated globally among healthcare workers, and there was a high heterogeneity (p<0.001; I2 =99.7%).
Across study locations, North America had the highest prevalence (37.3%; 95% CI 31.9% to 42.8%), followed by Australasia (28.2%; 95% CI 20.1% to 36.4%), Asia (24.1%; 95% CI 21.0% to 27.3%), Africa (20.9%; 95% CI 15.6% to 26.3%), Europe (20.1%; 95% CI 15.3% to 25.2%) and Latin America (4.4%; 95% CI 0.6% to 8.1%). Across practice settings, physical violence was the most prevalent in psychiatric/mental health settings (50.6%; 95% CI 34.8% to 66.4%). No significant between-group difference was observed for gender, income category and work schedules (all p>0.05).
In Asian countries, the pooled prevalence of physical violence was 19.6% (95% CI 14.1% to 25.1%) in 2000–2009 and increased up to 25.0% (95% CI 21.4% to 28.5%) in 2010–2018. By contrast, there was a decreasing trend in North America (48.9% vs 32.6%). The pooled prevalence of physical violence was stable in Europe (20.1% vs 20.3%) (table 2).
Factors associated with WPV
A total of 74 included studies investigated the predictors of WPV. Table 3 shows the results of the meta-analyses of factors associated with WPV. Healthcare workers exposed to shift work, who were younger and who worked longer hours (>40 hours per week) had a higher risk for any type of WPV. More experienced healthcare workers, healthcare workers from white ethnic backgrounds, physicians, nurses, healthcare workers working in urban settings and those who worked longer hours per week were more likely to experience non-physical violence. Male healthcare workers, more experienced healthcare workers, healthcare workers from white ethnic backgrounds, physicians, nurses, being single/unmarried healthcare workers and those who worked longer hours per week were more likely to encounter physical violence.
Meta-analysis of risk factors associated with WPV against healthcare workers
Exclusion of studies with quality scores less than 5 yielded pooled prevalence rates of 62.5% (95% CI 58.3% to 66.6%, p<0.001), 44.1% (95% CI 39.7% to 48.6%, p<0.001) and 25.7% (95% CI 23.1% to 28.3%, p<0.001) for any type of WPV, non-physical violence and physical violence, respectively. Analysis of studies that reported the prevalence of WPV against healthcare workers in any timeframe (12 months or lifetime) did not alter the results of the primary and subgroup analyses. These differences across subgroups were robust (eg, gender, study location, occupation, settings and so on) (online supplementary eTable 4).
The Egger’s test showed significant evidence of publication bias for studies that assessed the prevalence of any form of WPV, non-physical violence and physical violence (Egger’s p<0.05).
Discussion
This is the first comprehensive systematic review and meta-analysis to estimate the prevalence of any type of WPV, non-physical violence and physical violence against healthcare workers across the continents of the world.
This meta-analysis has added some newly important findings compared with previous seven reviews and meta-analyses13–19 in several important aspects. The number of included original studies, study perspective, and the scope and depth of study were different from the previous reviews. Our meta-analysis included 253 studies with larger sample sizes and many more events. The present study is the first to systematically summarise evidence on the prevalence and predictors of WPV towards all healthcare professionals (including physicians, nurses and other healthcare staff). Additionally, more detailed and comprehensive analyses were conducted in the current study. For example, the relationships between the prevalence of WPV and the gender of healthcare workers, practice settings, work schedules, professions mostly affected, geographical areas of affected healthcare workers and the types of WPV with the highest prevalence rates were investigated. Finally, we have identified the risk factors associated with WPV.
One valuable and important finding was that the pooled prevalence of WPV was higher among Asian countries than European countries. These observed differences may in part reflect differences in culture/context, differences in care or special workplace interventions (eg, human-centred workplace cultures, provision of adequate staffing levels, group training, open communication and so on) in various countries. Other possible reasons for the observed differences could be the difference in healthcare systems, lower numbers of healthcare workers per 1000 population and lower government health expenditure in Asian countries compared with European countries, resulting in heavier workloads for doctors and nurses and compromising communication skills with patients.33–35 Previous studies have highlighted that appointment or referral systems do not operate in some Asian countries (such as China, Thailand, India and so on).36 37 There are often lengthier waiting times in health settings in some Asian countries (such as China and India) and less time available to communicate with patients due to the heavier workloads, which may result in WPV.38 39 Alternatively, it could be that healthcare workers feel safer to report violent events in these settings leading to the higher prevalence. We also found that compared with European countries, North America and Australasia had a higher prevalence of WPV. This finding was in line with Nelson’s report40 that the highest rates of physical violence and sexual harassment against healthcare workers were found in Australia, England, Ireland, USA, Canada and New Zealand, while the lowest rates of bullying and sexual harassment were found in Europe. A possible explanation was that abuse cases were under-reported in European countries. A 2014 Medscape Ethics report indicated that European doctors were twice as likely to not report suspected domestic violence than their US counterparts,41 and this tendency to under-report may carry over to their own experiences of WPV. Nevertheless, more detailed analyses on this difference are needed. Finally, the regional differences observed in the prevalence of WPV may be attributed to broader social and individual factors. Social vulnerabilities are contextual factors (eg, cultural attitudes to healthcare workers, work setting, work environment and healthcare system). Individual vulnerabilities might include age, gender, education level, marital status, professional level and work tenure, as we identified these risk factors associated with WPV. These developmental and environmental factors can differentially and adversely affect different populations.42 43 This finding is important and provides new insights for future studies on vulnerability factors contributing to differences in exposure to WPV.
There were no significant differences in the prevalence of any form of WPV, non-physical and physical violence according to gender. This is inconsistent with previous findings, which have found that men are more likely to encounter WPV than are women.44–46 One possible explanation for our finding is the sample size differences between the two genders in this study, that is, there were fewer male than female participants. Some previous studies also did not report on gender; thus, gender differences may shift towards the null or become more pronounced. Interestingly, when we further analysed gender differences in the prevalence of WPV stratified settings within studies, we found that women than men were less likely to be exposed to physical violence, in primary care (OR=0.52; 95% CI 0.29 to 0.92) and in general hospitals (OR=0.65; 95% CI 0.47 to 0.89); however, women were more likely to encounter sexual harassment than were men (OR=3.92; 95% CI 2.70 to 5.70).
Healthcare professionals who worked in EDs and mental health settings reported higher levels of non-physical and physical violence exposure, respectively. This finding is in accordance with other studies,20 21 44 47which implicate these settings as risky for violence. For example, Cannavò et al 48 reported that women working in ED experienced a lower risk of aggression from patients. Al-Azzam et al 49 showed that marital status, work tenure, antiviolence policy and training about dealing with violence were important predictors of WPV for mental health department nurses. Jatic et al 50 found that gender and workplace setting (urban) were significantly associated with WPV in primary care institutions. In future studies, focusing on these settings may be of value in order to identify the key factors responsible for WPV in each setting, or in each ward or department.
This study has several notable strengths. First, previous studies have reviewed the prevalence of WPV against selected occupational groups (eg, doctors, nurses, ED staff only); however, the number of included studies, study population, research perspective and key points were different from our study. Thus, this is the first study investigating the prevalence and predictors of WPV against healthcare professionals around the world to date. Second, based on the subgroup analysis, we showed important findings that the prevalence of any type of WPV was much higher in Asian countries, North America and Australasia than in European countries, and higher across work groups with mixed shifts compared with fixed shifts groups (eg, day shifts and night shifts). Third, verbal abuse was the most common form of violence, followed by threats, physical assault and sexual harassment. Healthcare workers who practised in EDs were at higher risk for non-physical violence than other healthcare workers; however, those who worked in psychiatric settings had a higher risk for physical violence. Finally, we have further investigated the trends of study period-specific WPV prevalence across study locations. Overall, these analyses provide a broader view of WPV prevalence and its risk factors among healthcare professionals.
Some potential limitations of this study need to be mentioned. Although the definition of WPV was relatively objective and specific, its prevalence could have been underestimated. Various reasons for under-reporting WPV included absence due to injury or time lost, time-consuming incident reporting procedures, inadequate supervisory or coworker support, fear of reprisal or blame for reporting, or a belief that reporting violent cases will not lead to any positive changes.51 52 Under-reporting could result in underestimation of the true extent of the problem. Second, high heterogeneity was observed in this meta-analysis, as would be expected when pooling estimates across time and locations. The heterogeneity across studies may result from differences in healthcare systems, cultural background, samples, definitions and measurement of violence, occupation, and practice settings. However, sensitivity analyses and consistent results from various subgroup analyses indicated that our findings were relatively reliable and robust, and the heterogeneity can be overestimated when studies with large sample sizes are pooled.53
We suggest that, first, studies that investigate sociodemographic characteristics and the reasons and intentions of perpetrators are important, as these can help to better understand the reasons and risk factors for WPV. These can provide important information for the prevention of WPV. Second, additional studies investigating the long-term psychological and physical negative effects of WPV for healthcare workers would be of great value, as they could add to knowledge about the associations between WPV and adverse effects (eg, post-traumatic stress disorder, depression, anxiety, burn-out, turnover and so on). Third, standardising the definitions of WPV would further strengthen research evidence.
Our findings have important policy implications for the prevention and control of WPV. The findings from this study highlight the importance of enacting preventive strategies to reduce the risk of WPV over countries and practice settings. Prevention measures might include providing adequate staffing to reduce the weekly working hours of individual healthcare workers, or developing education and training programmes to assist healthcare workers to better manage WPV. It may also be of benefit to increase public awareness towards the negativity of the WPV phenomenon against healthcare professionals through mass media campaign, and to enforce appropriate policies and legislation (eg, encouraging staff to promptly report violent acts and judicial punishment on the perpetrators). The study findings suggest that prevention strategies are urgently needed, particularly in ED, mental health and prehospital settings,50 54–57 to reduce violence towards healthcare professionals at the workplace in order to maintain the healthcare system.10 58
Conclusions
In conclusion, the results of this meta-analysis suggest that the prevalence estimate of WPV committed by patients or visitors is high towards healthcare professionals globally, with disparities in regions and practice settings. Enacting preventive strategies and providing safer workplace environments for healthcare workers should be urgently prioritised.
References
Footnotes
JL and YG contributed equally.
FS and ZL contributed equally.
Contributors YG, FS and ZL conceived the study. JL and YG searched the databases and checked them according to eligibility and exclusion criteria. HJ and LL helped develop the search strategies. JL and YG performed the data extraction and quality assessment. JL, YG, HJ and FS analysed the data. HJ, LL, RD and FS gave advice on meta-analysis methodology. YG wrote the draft of the paper. JL, YG, HJ, RD, OS, YZ, YaC, FS and ZL contributed to reviewing or revising the paper. All authors read and approved the final manuscript. FS and ZL are the guarantors of this work, and as such had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was supported by the Fundamental Research Funds for the Central Universities, Huazhong University of Science and Technology, Wuhan, China (2016YXMS215), the National Natural Science Foundation of China (71804049), and the China Postdoctoral Science Foundation funded project (2018M630870).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.