Article Text

Abstract
This systematic review and meta-analysis aimed to examine whether working beyond the standard working hours was associated with a greater risk of depressive disorder among workers included in published prospective studies. This manuscript was prepared according to the PRISMA guideline checklist. A database search was conducted using MEDLINE (PubMed), PsycINFO, and PsycARTICLES using a relevant set of keywords. The eligibility criteria were as follows: (1) participants were adult workers; (2) exposure was defined as overtime work; (3) outcome were depressive disorders clinically diagnosed or assessed by a structured interview and (4) the study design was prospective or cohort. 7 studies were identified in the systematic review and meta-analysis. Overtime work was associated with a small, non-significant, elevated risk of depressive disorder (pooled relative risk=1.075; 95% CI 0.834 to 1.387; p=0.575) in a random effects model. The association tended to be greater for women. The risk of working 50 or more hours per week was slightly but not significantly increased (pooled relative risk=1.241; 95% CI 0.880 to 1.750; p=0.218). The effect of overtime work on depressive disorder remains inconclusive and may be small if not negligible. Sex differences and the effect of longer working hours on depressive disorder should be addressed in the future.
Trial registration number Prospero CRD42015020003; Results.
Statistics from Altmetric.com
What this paper adds
Many studies have indicated that long working hours deteriorated mental health.
However, the association between working hours and depressive disorder is not obvious.
From the results, the effect of overtime work on depressive disorder remains inconclusive and may be small if not negligible.
It would also be useful to measure possible moderators.
In practice, reducing working hours may not be effective in preventing depressive disorder in the workplace.
Introduction
Depressive disorder is a common mental health problem in the workplace.1 ,2 It is associated with poor quality of life and poor work performance of workers, and this has a significant impact on organisations and companies, as well as on society at large.3 ,4 Depression represents a continuous spectrum, ranging from mild, non-clinical symptoms to severe depressive disorder.5 At the extreme end of the spectrum, severe depressive disorder with greater levels of disability and an increased risk of relapse are observed.6 Therefore, depressive disorder is an important target of mental health interventions in the workplace.7
Although working hours have been considered associated with symptoms of psychological distress such as depression and anxiety,8–10 the association between working hours and depressive disorder is not obvious. For instance, long hours of overtime work are the basis for judicial decisions regarding worker compensation for work-related mental disorders and suicide in Japan and Korea.11 However, systematic and meta-analytic reviews have found an inconsistent association between working hours and depression.12–15 Sparks et al12 reviewed 19 studies and established that working hours had a small, but significant, positive correlation with mental health, including depression. Fujino et al13 reviewed 17 studies and concluded that the association between working hours and the mental health, including depression, were inconsistent. A systematic review by van der Hulst14 examined three studies on working hours and psychological ill health and six studies on working hours and general ill health, including psychological distress, and also found inconclusive results. However, a recent systematic review15 of nine studies on mental state (5 on depressive state and 2 on anxiety) found a positive association between working hours and depressive state.
Of note, these systematic reviews evaluated different types of depression, ranging from non-clinical depressive symptoms to depressive disorder, as the outcome.8 Few studies have examined depressive disorders classified according to internationally standardised criteria.16–18 A systematic review and meta-analysis specifically addressing the association between working hours and depressive disorder would be useful to plan strategies focusing on the reduction of working hours, for the primary prevention of depressive disorder in the workplace.
This systematic review and meta-analysis aims to examine whether working hours beyond standard working hours are associated with a greater risk of depressive disorder. To the best of our knowledge, this is the first systematic review and meta-analysis specifically analysing this association. Since it is ethically problematic to conduct trials using working hours as exposure, we evaluated published prospective studies in order to investigate this association. We hypothesised that longer working hours would increase the risk of depressive disorder.
Methods
Protocol and registration
This review followed the PRISMA statement and the study protocol was registered at the PROSPERO (ID=CRD42015020003), http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015020003.
Study selection
Data sources and search terms
A systematic search of studies was conducted on 15 July 2016, using MEDLINE (PubMed), PsycINFO, and PsycARTICLES databases. There were no limitations on publication dates and the search focused on all publications containing target key words. Two investigators (NK and KI) conducted preliminary search using different key words. Key words were also extracted from the recent systematic review.15 The investigators independently proposed a set of keywords for the search and these were combined. The following combinations were used: ((work* AND hour*) OR workhour* OR (long AND hour*) OR (extended AND hour*) OR overtime OR overwork OR (extended AND work*) OR workload OR (job AND stress)) AND (‘depressive disorder’[MeSH Terms] OR (‘depressive’[All Fields] AND ‘disorder’[All Fields]) OR ‘depressive disorder’[All Fields] OR ‘depression’[All Fields] OR ‘depression’[MeSH Terms]) AND ((longitudinal AND study) OR (cohort AND study) OR (prospective AND cohort AND study) OR (prospective AND studies) OR (follow-up AND studies) OR (observational AND stud*)). Search strategies were adapted for PsycINFO and PsycARTICLES, as required.
Eligibility criteria
The eligibility criteria for the selection of studies to be included in this systematic review and meta-analysis were as follows:
(1) participants were adult workers employed by a company/organisation; (2) exposure was overtime work (defined as overtime per day, per week, or per month) beyond normal or regular working hours (operationally defined as 35–40 hours/week, which is consistent with the definition adopted by many countries, according to a recent International Labour Office survey19); (3) outcomes were depressive disorders diagnosed by a clinician or assessed by a structured interview; and studies using only a self-reported measure of symptoms of depression were excluded and (4) only prospective or cohort studies, including a case–control study nested in a cohort study, were considered.
Study selection process
First, two investigators (KI and KW) independently reviewed the abstracts of the records identified by the search (first screening). Second, a full-text review was conducted (second screening). We obtained the full-texts of the articles that met the eligibility criteria and those where we could not determine on the basis of the abstract alone. The instances when the two investigators did not agree on eligibility, three investigators (NK, KI and KW) carefully discussed the articles to determine whether these should be included or excluded.
Data collection
Information regarding study characteristics, overtime work, depressive disorder, and measure of the association between overtime work and depressive disorder, was collated from each eligible study. If the studies did not list this information and/or contained unclear information, we contacted the corresponding authors to seek clarification.
Characteristics of studies
The following data were collated: year of publication of the study, country where the study was conducted, study design (prospective, cohort, or nested case–control), sample sizes, sampling framework (population based or worksite based), participant characteristics, the number of outcome events (ie, the number of participants who have experienced depressive disorder during follow-up), length of follow-up and follow-up rate, if applicable.
Overtime work
The information on criteria for overtime work was collected as the exposure variable. In order to conduct a comparison with standard working hours (35–40 hours/week19), information on working hours and overtime was converted into working hours per week. The calculations were as follows: working hours per day were multiplied by 5; working hours per month were divided by 4; and overtime per month was divided by 4 and then 40 was added to this result.
Depressive disorder
Outcomes were as follows: new-onset depressive disorder or new treatment or sick leave due to depressive disorder diagnosed by a clinician or assessed by a structured interview during follow-up.
Association measures between overtime work and depressive disorder
We analysed relative risks (RRs), HRs or ORs (hereafter called RRs), and the 95% CIs of the association between overtime work and depressive disorder. Three investigators (NK, KI and KW) collaborated on extracting RRs and the CIs from each study for the meta-analysis while adjusting for demographic covariates, where possible. We did not use RRs adjusted for psychosocial factors at work (eg, job demands). When a study reported multiple RRs for different criteria of overtime work, we extracted the RR from each study for the nearest criteria to the standard working hours (35–40 hours/week).19 We selected RRs for men and women when the study provided only sex-specific RRs. Some studies reported sex-specific RRs in addition to sex-adjusted RRs. In these cases, we used the sex-adjusted RRs and then used the sex-specific RRs for a sex-stratified subanalysis. When a study reported RRs for population subsamples (eg, by occupation), as well as for the total population, the RR for the total population was used for the meta-analysis.
Statistical analysis
All RRs were transformed to a natural logarithm. We estimated the SE for a log-transformed RR based on the 95% CI for the RR. A log-transformed RR and its SE were used for the meta-analysis. For the main analysis, main RRs and the SEs from selected studies were subjected to a random-effects model meta-analysis (‘metan’ procedure using Stata V.12) to estimate a pooled RR and its 95% CI. Considering a possible heterogeneity in RRs among studies due to study characteristics, such as sample sizes and countries, we used a random effects model.20 However, we also conducted the analysis using a fixed-effect model. Heterogeneity among the studies was tested using I2. Publication bias was examined by drawing a funnel plot and conducting the Egger's test.
Subgroup meta-analyses were performed separately for men and women as well as Western and non-Western countries. A sensitivity analysis was also conducted for studies using longer hours as a criteria of overtime work (as working 50 and 60 hours per week or more). Additionally, using the ‘metareg’ procedure of Stata V.12, meta-regressions were conducted to determine the association between the RRs and the follow-up duration and publication year, respectively.
Changes to the protocol
After the registration of the study protocol at the PROSPERO, we changed its protocol in following points to improve the research quality. First, search terms were changed from (‘work hours’ OR ‘work hour’ OR workhours OR ‘working hours’ OR (‘work’ AND ‘hours’) OR ‘long hours’ OR ‘extended hours’ OR overtime OR overwork OR ‘extended work’ OR workload) AND depression AND (‘Longitudinal Studies’[MeSH Terms] OR ‘prospective studies’[mesh] OR ‘cohort studies’[mesh]) to ((work* AND hour*) OR workhour* OR (long AND hour*) OR (extended AND hour*) OR overtime OR overwork OR (extended AND work*) OR workload OR (job AND stress)) AND (‘depressive disorder’[MeSH Terms] OR (‘depressive’[All Fields] AND ‘disorder’[All Fields]) OR ‘depressive disorder’[All Fields] OR ‘depression’[All Fields] OR ‘depression’[MeSH Terms]) AND ((longitudinal AND study) OR (cohort AND study) OR (prospective AND cohort AND study) OR (prospective AND studies) OR (follow-up AND studies) OR (observational AND stud*)) for a more detailed search. Second, the inclusion criteria for the outcomes were changed. The original plan included studies of antidepressant use. We limited eligible outcomes to diagnosed depressive disorder. Third, the original plan was to collect multiple RRs for the different criteria of overtime work reported in studies in an effort to conduct a sensitivity analysis for overtime work as work exceeding 40 hours/week; and a meta-regression was planned to determine the association between the criteria of overtime work and RRs. However, in the new protocol, we collected one ‘representative’ RR from each study, which was calculated for an overtime category more than and closest to the standard working hours, that is, 35–40 hours/week not conducting a meta-regression for different overtime criteria.
Results
Selected studies
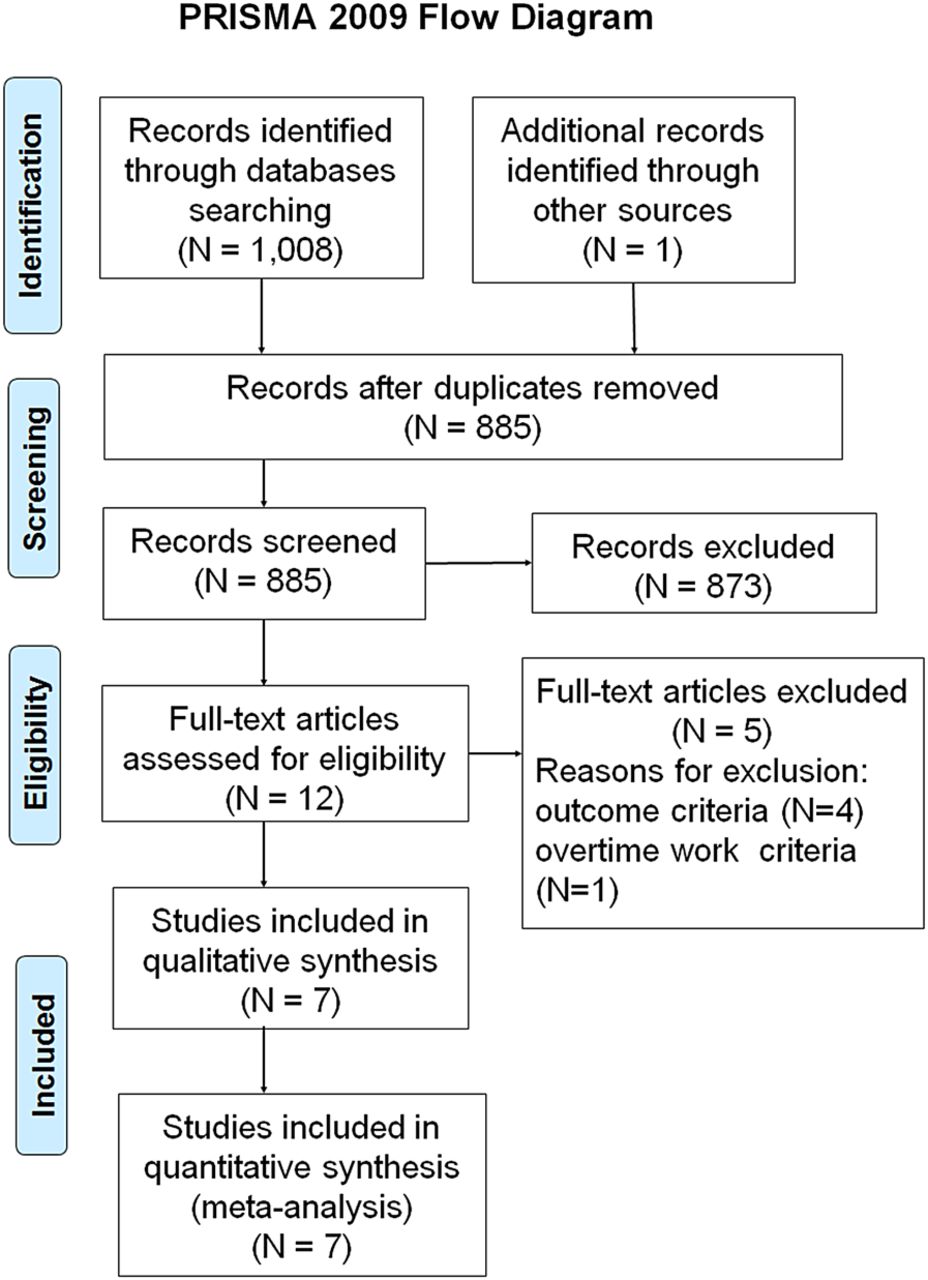
A PRISMA flow diagram of the study selection process is shown in figure 1. The initial search of the databases identified 1008 records. In addition, one record21 was identified through other sources, a secondary analysis of pre-existing data used for an already published study.22 From the 1009 records, 124 duplicates were removed. Following the first screening of the abstracts of the remaining 885, two authors (KI and KW) identified 12 records. Following the second screening of the 12 records by the two authors, 5 records were excluded because they did not meet the following criteria: outcome (N=4), or overtime work (N=5). Finally, seven studies were included in the systematic review and the meta-analysis.

PRISMA flow diagram.
Study characteristics
The seven studies that met our inclusion criteria are shown in table 1.17 ,18 ,21 ,23–26 Two of these were nested case–control studies. Kawakami et al23 conducted a 3-year nested case–control study with 15 cases of major depressive disorder and 75 controls among workers in a large company. Ogasawara et al24 also conducted a 1-month nested case–control study with 124 cases of major depressive disorder and 124 controls among workers in four companies. The remaining five studies were prospective (cohort) studies.17 ,18 ,21 ,25 ,26 In addition, Ogasawara et al24 also conducted a cohort study among 2740 employees. The follow-up duration for these five studies was 1–5.8 years, while the follow-up rate was 77.0–93.6. Three of the five studies adopted major depressive disorder as the outcome measure,21 ,25 ,26 while the other two adopted major depressive episode.17 ,18 The number of participants who have been newly diagnosed as depressive disorder were 8–175 among the studies. Two studies21 ,23 reported RRs for men only, four studies18 ,24–26 reported sex-combined RRs, and one17 reported RRs stratified by sex. Three studies21 ,23 ,24 were conducted in a non-Western country, that is, Japan, while the other four17 ,18 ,25 ,26 were conducted in Western countries, including Canada, the UK, and France.
Studies included in the systematic review and meta-analysis (N=7)
Results of individual studies
The measures of the association between overtime work and depressive disorder used in the seven studies examined in this review are shown in table 2. Of them, six studies reported a non-significant association between overtime work and the onset of depressive disorder;18 ,21 ,23–26 one study reported a significant positive association17 in women.
The measures of association between working hours and depressive disorder among seven studies
Several mistakes were found in the results published by Ogasawara et al;24 therefore, we received an erratum from the corresponding author. Furthermore, Wang et al25 compared three groups stratified according to weekly working hours (35–40, >41, and <35 hours/week); however, the RR for only the group working for 35–40 hours (compared with the group working <35 hours) was described in each study. We therefore, contacted the authors and obtained additional information on the RRs for the other groups.
Some studies conducted subanalyses or additional analyses. Kawakami et al21 conducted a subgroup analysis, stratifying respondents according to high and low depressive symptoms at baseline, as measured by the Center for Epidemiologic Studies Depression Scale (CES-D). The authors found only a small difference in the risk of sick leave due to depressive disorder (RR=1.25) between respondents working normal and those working long hours in the total sample. However, working 60 or more hours of overtime per week was associated with an ∼10-fold increased risk among respondents with a high CES-D score (≥16). An interaction term between work hours and CES-D score was marginally significant (p<0.10). In two of seven studies, the analyses were conducted using longer work hours as the criterion of overtime work. For instance, Kawakami et al21 investigated the risk of sick leave due to depressive disorder among workers who worked 60 or more hours per week, compared with those who worked less (RR=0.92; 95% CI 0.32 to 2.70). Virtanen et al18 reported a significantly elevated risk for the onset of major depressive episode among workers who worked 55–60 hours/week, compared with those who worked standard working hours (RR=2.30; 95% CI 1.05 to 5.06).
Meta-analysis
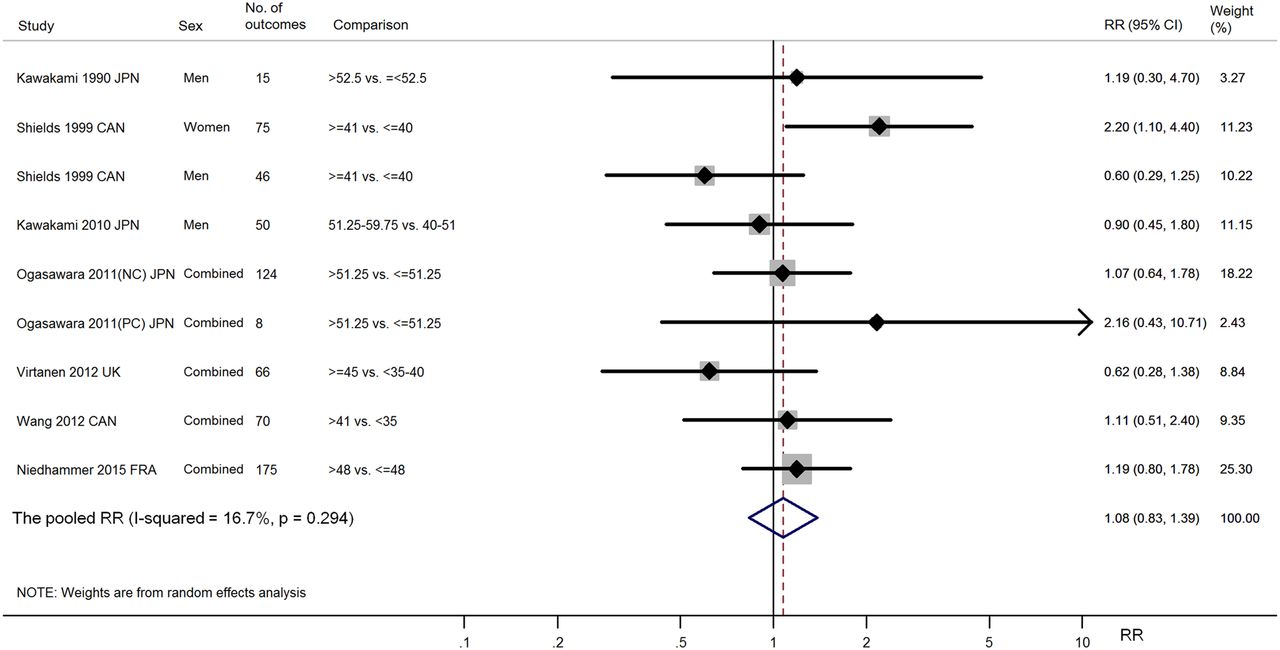
A meta-analysis using the random effects model showed some variation in the association between overtime work and depressive disorder (9 RRs derived from 7 studies) (figure 2). The pooled RR was slightly positive (RR=1.075; 95% CI 0.834 to 1.387) but not statistically significant (z=0.56, p=0.575). The heterogeneity was moderate (I2=16.7%) but not statistically significant (χ2 (8)=9.61, p=0.294). A fixed model meta-analysis also showed a slightly significant and slightly positive association between overtime work and depressive disorder (RR=1.084; 95% CI 0.868 to 1.354, z=0.71, p=0.476; data available on request).

Overtime work and relative risks (RRs) of depressive disorder for seven studies: a random-effect model.
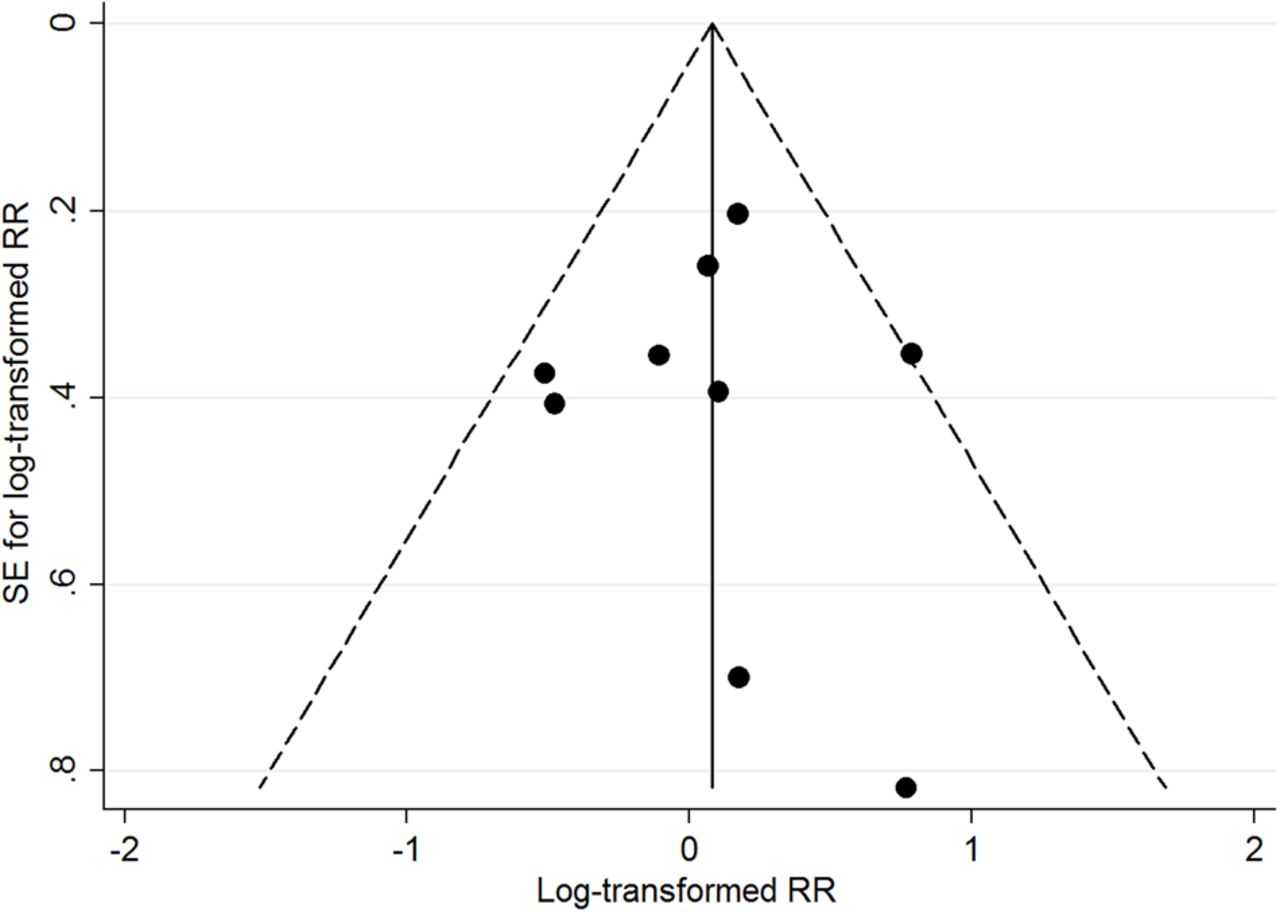
A funnel plot for the log-transformed RRs of depressive disorder associated with working hours and the SEs among the nine RRs from the seven studies indicated a relatively smaller number of studies with greater SE (ie, with a smaller sample size) reporting greater RRs (figure 3). The Egger's test was not significant (p=0.979).

{kind=link}
{kind=link}
{kind=link}
Funnel plot for log-transformed relative risks (RRs) of depressive disorder associated with overtime work and SEs for seven studies.
A meta-analysis of RRs was conducted using a random-effects model for sex-specific subgroups. For men (3 RRs derived from 3 studies), the pooled RR was 0.786 (95% CI 0.489 to 1.262), which was not significant (z=1.00, p=0.318). The heterogeneity was not significant (I2=0.0%, χ2 (2)=1.02, p=0.600). We could not calculate the pooled RR for women because only one study17 reported a RR for women, which was significantly high (RR=2.20, 95% CI 1.10 to 4.40). For five RRs reported in four studies for samples of men and women combined, the pooled RR was 1.081 (95% CI 0.825 to 1.416), which was not significant (z=0.57, p=0.572), and had almost no heterogeneity (I2=0.0%, χ2 (4)=2.81, p=0.591). Meta-analyses stratified by geographical areas, indicated that the pooled RR for Asian countries (Japan only) was similar (RR=1.066, 95% CI 0.727 to 1.562; based on 4 RRs derived from 3 studies, z=0.33, p=0.745) to that for the western countries (RR=1.049, 95% CI 0.682 to 1.613; based on 5 RRs derived from 4 studies, z=0.22, p=0.827). In the sensitivity analysis using the overtime criteria of working 50 hours or more per week (5 RRs derived from 4 studies), the pooled RR was 1.241 (95% CI 0.880 to 1.750) and not significant (z=1.23, p=0.218), with no significant heterogeneity (I2=0.0%, χ2 (4)=3.86, p=0.425). Only one study21 reported a RR of depressive disorder associated with working 60 or more hours per week (RR=0.92; 95% CI 0.32 to 2.70, p=0.885).
A meta-regression analysis of nine log-transformed RRs from all seven studies was conducted on follow-up length and publication year. The coefficient of the follow-up length on the RRs was slightly negative (−0.064, SE=0.075) but not significant (p=0.423). Publication year was not significantly correlated with RRs (coefficient −0.006; SE 0.021, p=0.785).
Discussion
The estimated pooled RR of the newly onset of depressive disorder associated with overtime work from the seven studies was small and not significant (pooled RR=1.075 in the random effects model). The analysis using the fixed-effect model yielded a slightly significant, but similar pooled RR (1.084). The observed RR of depressive disorder was smaller than the RRs of stroke (1.33) and coronary heart disease (1.13) associated with overtime work reported from a recent meta-analysis of studies in Europe, the USA, and Australia.27 Previous meta-analytic studies showed that the association between working hours and depressive symptoms was significant and positive.12 ,15 However, this study found that the effect of overtime work on depressive disorder was still inconclusive and may be small or negligible. The criteria for defining overtime work used in the selected studies varied: working 41 hours/week or longer in three studies, 48 or longer in one study; and 52–53 or longer in four studies. It should be noted that the estimated pooled RR was a summary of associations observed in the studies, and it may not be an accurate estimate of the effect of a certain level of overtime work on the onset of depressive disorder. This makes it difficult to interpret the present finding. A meta-analysis study applying a same definition of overtime work should replicate the present finding in future.
The small pooled association between working hours and depressive disorder may be explained by moderators of the association. Studies have reported potential moderators of the association, such as baseline depression and psychosocial factors at work. Several studies reported a stronger association between working hours and depressive disorder at baseline among respondents with depression compared with those without.21 ,28 Kawakami et al21 reported a marginally significantly increased risk of sick leave due to depressive disorder associated with working 60 or more hours per week among respondents with high symptoms of depression (RR=2.97, 95% CI 0.89 to 9.84, p=0.076). The risk was much smaller among respondents without symptoms of depression (RR=0.33, 95% CI 0.05 to 2.46, p=0.281). The other study which was not included in the systematic review and meta-analysis28 found a significant association between longer working hours (>35 vs ≤35 hours/week) and depressive disorder among respondents with current and/or a lifetime major depressive disorder, but no significant association among respondents without major depressive disorder.25 Although further empirical evidence is required, overtime work may be a risk factor for the occurrence or recurrence of depressive disorder in individuals with underlying depression. A further potential moderator is the psychosocial work environment. A significant interaction effect between working hours and job strain on depressive disorder has been reported.25
Only one study17 reported the association between overtime work and depressive disorder for women (RR=2.20), which was greater than the association for men in the same study (RR=0.60). Women may be more vulnerable to developing depressive disorder due to overtime work compared with men because of psychological and physiological differences between sexes. Several possible reasons for the greater effect of overtime work on mental health have been suggested. First, women are more likely to have household and other family responsibilities than men.8 ,29 Therefore, women could have less time to recover from the effects of overtime work than men. Second, overtime work might lead to work–family conflicts and depressive disorder in women.30 ,31 Several studies have suggested that the effect of work–family conflicts on depression is greater for women.32–34 Wang et al,25 in their study included in this review, reported that work–family conflicts were associated with an elevated risk of major depressive disorder among women but not men. Third, because women are less likely to have job control compared with men, the effect of overtime work on mental health could become greater. Further research is urgently needed to accumulate evidence of the association between overtime work and depressive disorder among women as well as investigate the possible mechanisms.
When the overtime criteria of working 50 or more hours per week were used, the pooled RR was slightly increased (1.241), but the difference was not significant. The studies included in this analysis generally reported with 95% CIs, and there seemed to be two groups of studies reporting high (>2.00) and moderate (0.92 to 1.20) RRs. Only one of these studies21 calculated a RR associated with working 60 or more hours per week, which was not significant. It was still not clear from this meta-analysis if there was a dose-relationship association between longer work hours (eg, 50 or more hours per week) and the risk of depressive disorder. It is not clear whether working for extremely long hours (eg, 70–80 hours/week) is associated with depressive disorder.
Several limitations should be considered. First, as we stated earlier, studies that were included used different criteria to define overtime work. The studies also used different measures of depressive disorder, from a diagnosis based on a standardised structured interview to treatment or sick leave due to the disorder. Such heterogeneities in measurements among the studies make the interpretation of the present findings difficult. These may also result in an inaccurate estimation of the pooled RR. Second, the results of individual studies might be biased by common methodological problems. Attrition is the most likely bias that could occur in this type of cohort study. For instance, individuals working longer hours and developing depressive disorder were more likely to leave their jobs and be lost to follow-up. Alternatively, the healthy worker effect could affect the findings, as only individuals adapting to long working hours may continue to work long work hours. Moreover, working hours may change over time, resulting in an underestimation of the association. The lack of a clear association between work hours and the risk of depressive disorder in this study may be due to such attrition bias. Other types of biases or measurement errors may also affect the findings of individual studies. We were unable to control this problem since we did not conduct quality and methodological assessments of the included studies. Third, this systematic review and meta-analysis did not consider situational factors. We were unable to collect information on whether overtime work was paid or unpaid, forced or voluntary. Overtime work intensity was also not assessed. Fourth, there were a limited number of studies from Asia, all of which were from Japan, and no studies from Latin America or Africa. Finally, workers with depression may have refused to work longer, blinding the true association.
Conclusions and research implications
This systematic review and meta-analysis found that overtime work was associated with a small, non-significant increase in the risk of depressive disorder. There was considerable heterogeneity in the methodology of the selected studies, specifically, in terms of the measurements and definition of overtime work and the assessment of depressive disorder. Future studies on working hours and depressive disorder need to use common criteria for overtime work and common measures of outcome. It would also be useful to measure possible moderators (such as depression at baseline or psychosocial factors at work). In practice, reducing working hours may not be effective in preventing depressive disorder in the workplace; however, this assumption has not been confirmed yet. Identifying high-risk workers with long working hours and targeting interventions to this high-risk group may be an alternative approach.
Acknowledgments
The authors thank Professors Toshiaki Furukawa from the School of Public Health, Kyoto University, and Manami Inoue from the Graduate School of Medicine, the University of Tokyo, for their valuable comments and advice on the manuscript.
References
Footnotes
Contributors KW, KI and NK have made substantial contributions to conception, design, analysis, interpretation of data, and reporting of the work described in the article. NK is responsible for the overall content as a guarantor.
Funding The present study was supported by the Health and Labor Sciences Research Grant 2015–2017 (H27-Rodo-Ippan-004) from the Ministry of Health, Labour and Welfare, Japan.
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.