Article Text

Abstract
Objectives Asbestos is the name given to a group of naturally occurring silicate mineral fibres that were widely used in industry during the 20th century due to their desirable physical properties. Although use in the USA has fallen over the last three decades, significant exposure in the developing world continues and the burden of disease is considerable. Asbestos is a known risk factor for several malignant diseases, including lung cancer and mesothelioma, and has more recently been implicated in pharyngeal and laryngeal cancer. However, studies of asbestos and cancers of the larynx or pharynx with adequate sample size that control for major head and neck squamous cell carcinoma (HNSCC) risk factors remain relatively sparse.
Methods We report findings from a case–control study of 674 incident male HNSCC cases from the greater Boston region and 857 population-based male controls, matched on age (±3 years), sex, and town or neighbourhood of residence. Multivariable logistic regression was used to assess the association between occupational asbestos exposure and HNSCC by primary tumour site.
Results 190 cases (28.2%) and 203 controls (23.7%) reported occupational exposure to asbestos. Occupational asbestos exposure was associated with elevated risk of pharyngeal carcinoma in men (OR 1.41, 95% CI 1.01 to 1.97), adjusted for age, race, smoking, alcohol consumption, education, income and HPV16 serology, with borderline increasing risk for each decade in the exposed occupation (OR 1.10, 95% CI 0.99 to 1.23).
Conclusions These observations are consistent with mounting evidence that asbestos is a risk factor for pharyngeal cancer.
Statistics from Altmetric.com
What this paper adds
-
There is evidence in the literature of an association between occupational asbestos exposure and pharyngeal and laryngeal cancer, although studies are limited and few adequately control for major risk factors for these diseases, particularly for pharyngeal cancer.
-
Additional studies are needed to better establish asbestos as a risk factor for pharyngeal and laryngeal cancer and increase the precision of the estimated risk.
-
We observed an increased risk of pharyngeal carcinoma associated with occupational asbestos exposure in a large case–control study of men from the greater Boston area.
-
This study is the first of its kind to include adjustment for HPV16 exposure, along with control for other major head and neck cancer risk factors.
-
Our observations are consistent with the mounting evidence that asbestos is a risk factor for pharyngeal cancer and have important implications for occupational risk assessment and policy.
Introduction
Asbestos is the name given to a group of naturally occurring fibrous silicate mineral compounds. Its use dates back thousands of years but became wide-spread in the late 19th century through the late 20th century1 due to its favourable industrial properties, including its strength, flexibility and thermal properties, with peak use in the USA occurring in the 1970s. Asbestos has been associated with a number of chronic respiratory diseases,2 including malignancy, and was first linked to mesothelioma3 and lung cancer4 in the early to mid part of the 20th century. Despite the known health risks, an estimated 125 million people are still occupationally exposed worldwide.5 While asbestos is tightly regulated or banned in parts of the developed world, its unregulated use continues in many developing countries, with annual global production currently estimated at 2 million metric tons.6
Asbestos has also been implicated as a risk factor for squamous cancers of the upper airway, in particular laryngeal and pharyngeal carcinoma, as indicated by recent meta-analyses.7 ,8 While the association between asbestos exposure and laryngeal cancer is now fairly well established, the data associating pharyngeal cancer with asbestos exposure are somewhat sparse. Many, if not most, currently available studies have relatively small sample sizes, and proper control of potentially confounding factors has been somewhat inconsistent.1 ,7 A number of cohort studies are available in the literature but generally offer a very limited number of cases with no adjustment for potential confounding. Case–control studies have been more successful in addressing confounding issues but are, to date, relatively few in number, particularly for pharyngeal cancer9–15; only one study has specifically examined the relationship with oral cancer.10 Further, among the studies that do adjust for confounding, none to date have included past exposure to HPV16, a major risk factor for head and neck cancer,16 ,17 in their analyses. These limitations of the current literature, along with the compelling public health implications, indicate a need for continued study of asbestos exposure to enhance the evidence pool and add to the precision of risk estimates for head and neck cancer. Thus, the objective of our study was to assess the risk of head and neck cancer associated with occupational asbestos exposure in a large, well-controlled, population-based case–control study of men from the greater Boston area.
Methods
Study population
Incident cases of head and neck squamous cell carcinoma (HNSCC; ICD-9 codes 141, 143–146, 148, 149, 161) were enrolled through major teaching hospitals located in Boston, Massachusetts (Brigham and Women's Hospital, Beth Israel Deaconess Medical Center, Boston Medical Center, Dana-Farber Cancer Institute, Massachusetts Eye and Ear Infirmary, Massachusetts General Hospital and New England Medical Center, which together see the vast majority of HNSCC cases in the region) as part of a population-based case–control study of head and neck cancer in the greater Boston area.18 ,19 For inclusion in the study, cases were required to reside in Boston or any of 162 contiguous cities and towns within an approximately 1 h drive of Boston at the time of diagnosis. Control subjects with no prior history of HNSCC were matched to each index case on age (within ±3 years), gender and neighbourhood/town of residence (determined by zip code) through town records (Massachusetts towns/municipalities maintain publicly available annual residential records). Due to minimal occupational asbestos exposure among female participants, we have restricted the present interrogation to male cases and controls. The study includes data collected from two periods of recruitment from the same population: phase I was conducted between December 1999 and December 2003 (381 male cases and 493 male controls) and phase II was conducted between October 2006 and June 2011 (373 male cases and 420 male controls). Men who did not provide a response for occupational asbestos exposure in the questionnaire were excluded (80 cases and 56 controls), leaving 674 cases and 857 controls for analysis. Participation rates for cases and controls were 78% and 47%, respectively. All cases and controls enrolled in the study provided written informed consent as approved by the Institutional Review Boards of the participating institutions.
Data collection
Subjects completed a self-administered, interviewer reviewed questionnaire that provided detailed data on sociodemographics and personal characteristics, alcohol and tobacco use, personal and family cancer history, occupational history of asbestos exposure, and other relevant dietary, health behaviour, occupational, residential and medical history. An in depth occupational history was collected for each different occupation held by each study subject, including start and end dates (available for 99.5% of subjects reporting occupational asbestos exposure), job titles and industries, and self-reported exposure to occupational dusts, exhausts/fumes and asbestos. Duration of work at an asbestos-exposed occupation was calculated for each subject by subtracting the start from the end date for each occupation for which asbestos exposure was reported and summing up the total duration across all occupations.
HPV16 serology
Serological HPV16 testing for L1 viral protein antibodies was performed on study subjects as a measure of past HPV16 exposure. Sandwich ELISA assays were used for detection of HPV16 antibodies as previously described.20 ,21 Positive HPV16 L1 serology is considered to be a proxy for past exposure to the virus.
Statistical analysis
Crude ORs were generated for the association between each covariate and case status (adjusted for age, which was a matching factor). Univariate statistics for normally distributed continuous covariates (ie, age) were assessed by two-way ANOVA for differences by primary tumour site among cases and by the non-parametric Kruskal–Wallis test when not normally distributed, with normality determined by the skewness-kurtosis test.22 Categorical differences by site were assessed by Fisher's exact test. All tests were two-sided and significance was considered where p≤0.05.
Unconditional multivariable logistic regression was applied to estimate HNSCC risk for each respective primary tumour site (ie, oral cavity, pharynx, larynx) associated with self-reported occupational asbestos exposure, adjusted for age (continuous, centred at the median), race (White vs non-White), cigarette smoking (modelled both as a binary ever/never smoking term and continuously as pack-years, considered additively), alcohol consumption (categorised as: non-drinker, ≤14 drinks/week and >14 drinks/week), highest level of education (high school or less vs greater than high school), annual household income (categorised as: <US$25 000, US$25 000–US$79 999 and ≥US$80 000) and HPV16 L1 serology (negative vs positive). For the purpose of quantifying alcohol consumption, an alcoholic beverage was defined as a 12 oz. beer, 5 oz. glass of wine or 1.5 oz. of spirits. Occupational asbestos exposure, the primary independent variable in these analyses, was separately modelled as both a binary variable (ever vs never occupationally exposed) and continuously, by total years at an occupation(s) with asbestos exposure. The functional form of continuous covariates included in the model was assessed in the multivariable setting using fractional polynomial analysis,23 where any polynomial term offering a significantly improved fit over the linear term was considered (p≤0.05).
Values were missing for race (1 case, 1 control), alcohol consumption (2 cases, 2 controls), education (1 control), annual household income (81 cases, 92 controls) and HPV16 L1 serology (106 cases, 77 controls); data were complete for age and smoking. To compensate for the missing values in the logistic regression models, multiple imputation (5 imputations) was employed using multivariate normal regression, based on age and smoking data (ever/never+pack-years); multiple imputation results in less biased findings when dealing with missing covariate data.24
To explore the possibility of biological interaction between major HNSCC risk factors, we generated joint effects models for heavy smoking and/or drinking with asbestos and HPV16 serology with asbestos and then estimated the relative excess risk due to interaction (RERI), a measure of biological interaction as determined by departure from additivity;25 separate models including multiplicative terms between history of occupational asbestos exposure and heavy smoking/drinking and HPV16 L1 serology were also generated to assess potential multiplicative interaction. The joint effects models generated for the RERI estimates exclude subjects missing the covariate data included in the models. A very high number of imputations (ie, in the hundreds) are needed to obtain reliable variance–covariance matrices required for the RERI calculations, making it computationally prohibitive. For the purpose of the joint effect models, heavy drinking was defined as consumption of more than 14 alcoholic beverages in a typical week. Heavy smokers were defined as subjects with more than 18.3 total pack-years of smoking; this cut-point was based on the top two tertiles of pack-years among ever-smoking control subjects.
CIs for the RERI analyses were estimated using the biological interaction tool available through EpiNET (http://www.epinet.se). All other statistical analyses were conducted in Stata 11 (College Station, Texas, USA).
Results
A total of 190 cases (28.2%) and 203 controls (23.7%) reported an occupational exposure to asbestos. Cases were more likely than controls to be ever-smokers and smoked more, were more likely to be heavy drinkers, were less educated, had a lower annual household income, and were more likely to have positive HPV16 L1 serology. Among cases, there were significant differences across primary tumour sites (oral cavity, pharynx and larynx) by smoking habit (p<0.001), alcohol consumption (p=0.003), educational level (p=0.01), annual household income (p<0.001) and HPV16 serology (p<0.001). A detailed description of the study population is provided in table 1. Study subjects missing occupational asbestos data did not significantly differ from those reporting these data with respect to the covariates considered in table 1 (data not shown).
Description of the study population by case–control status and primary tumour site
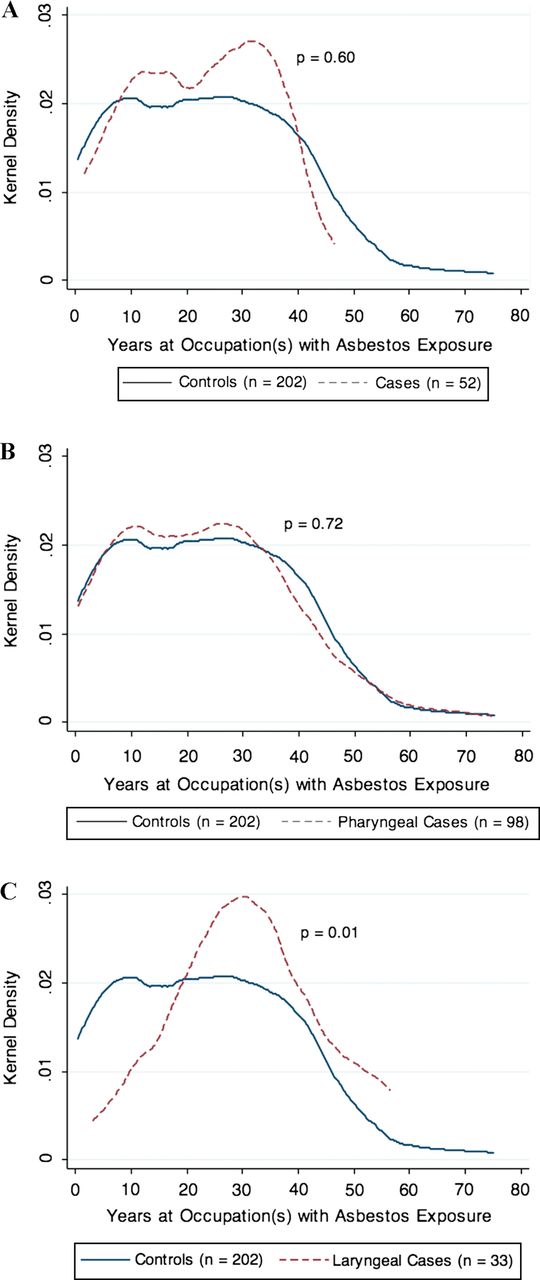
An elevated OR was observed between occupational asbestos exposure and pharyngeal squamous cell carcinoma (OR 1.41, 95% CI 1.01 to 1.97), after adjusting for age, race, smoking, alcohol consumption, education, income, and HPV16 serology (table 2). There was also a borderline dose–response relationship observed for each decade working in an occupation with asbestos exposure and pharyngeal carcinoma (OR 1.10, 95% CI 0.99 to 1.23); the distribution of duration of occupational asbestos exposure by case–control status is provided in figure 1. No significant associations were observed between occupational asbestos exposure and HNSCC originating in the oral cavity or larynx, although sample sizes may have limited our ability to examine these relationships, in particular for laryngeal carcinoma.
Self-reported occupational exposure of men to asbestos and head and neck squamous cell carcinoma (HNSCC) by primary tumour site, for any occupational asbestos exposure and by duration spent at an asbestos-exposed occupation
{kind=link}
Distribution of duration working at an occupation(s) with asbestos exposure in years by case–control status among study subjects reporting ever having been exposed. The plots represent the kernel density of duration of exposure for controls and (A) oral cavity carcinoma cases, (B) pharyngeal carcinoma cases and (C) laryngeal carcinoma cases. The p value for difference between cases and controls was determined by the Wilcoxon rank sum test and is presented on each respective corresponding plot.
Since unconditional logistic regression can potentially result in overestimation of the OR, we performed a sensitivity analysis using conditional logistic regression, in which we were able to pair 94% of our cases with controls. The conditional analyses yielded nearly identical point estimates (in fact the magnitude of the point estimate for the association of asbestos exposure and pharyngeal SCC is slightly higher for the conditional model), alleviating concern that estimates were inflated (data not shown).
The models examining asbestos and heavy smoking and/or drinking did not distinguish risk patterns of biological interdependence for any HNSCC site (neither on the additive nor multiplicative scale). The joint effects models and RERI estimates of biological interaction between major risk factors for HNSCC and occupational asbestos exposure are presented in table 3.
Self-reported occupational exposure of men to asbestos and HNSCC risk stratified by heavy smoking and/or heavy drinking status and by HPV16 serology
Discussion
The International Agency for Research on Cancer (IARC) considers asbestos to be carcinogenic to humans in all forms,1 with a well established link with mesothelioma and cancers of the lung, larynx and ovary. Although mounting, the evidence is not as clear for an association with pharyngeal cancer and little has been done to examine the risk (if any) that is specifically associated with oral cancer. Here, we strengthen this evidence with our observed association between occupational asbestos exposure and pharyngeal squamous cell carcinoma in men from a large, population-based case–control study of the greater Boston area, with an apparent dose–response relationship. Further, to our knowledge, this is the first study of asbestos and head and neck cancer that accounts for past HPV exposure, a major risk factor for the disease, particularly for cancers originating in the pharynx.
Our findings are in line with other case–control studies in the literature regarding asbestos exposure and pharyngeal cancer risk,9 ,13 ,15 with point estimates similar in magnitude to the summary estimates reported in recent meta-analyses,7 ,8 although the meta-analyses did not show a clear dose–response relationship.8 While we did not observe a significant relationship between asbestos and laryngeal squamous cell carcinoma, we do not believe that this finding calls into question the validity of our pharyngeal cancer results, as it is improbable that differential misclassification or bias would occur for pharyngeal (the lesser established association) and not for laryngeal carcinoma (the better established association). It should be noted that our statistical power to detect such a relationship was limited by our sample size (118 laryngeal cancers with only 35 men reporting an occupational asbestos exposure) and that our estimated CI for asbestos and laryngeal carcinoma overlaps the summary estimate obtained in a meta-analysis of ever-exposure by the Institute of Medicine (metaOR 1.43, 95% CI 1.15 to 1.78).7 We also observed no association with oral squamous cell carcinoma, which is consistent with the published literature.10 ,26
Case–control studies, although subject to certain limitations, offer considerable advantages over occupational cohort studies in the assessment of asbestos and head and neck cancer risk. Our use of a case–control study design enabled us to enrich our study population with a large number of cases of head and neck cancer, a relatively rare disease, allowing us to overcome the limitation of a cohort study design, for which few cases would be observed, even for comparatively large cohorts. Additionally, the relatively large sample size of our study enhanced our ability to detect an association with pharyngeal cancer, while the population-based nature of the study provided us with a generalisable risk estimate. Further, the well-annotated subject-specific data on major risk factors for head and neck cancer, including HPV16 serology, enabled thorough control of potential confounding in the examination of HNSCC risk associated with occupational asbestos exposure.
A potential limitation of our study design was the use of self-reported occupational exposure. If the misclassification is non-differential between case and control subjects, we believe that this would result in underestimation of the true risk, as study subjects are more likely to under-report asbestos exposure (ie, not realise that they were exposed). However, we cannot rule out the potential for differential misclassification or recall bias due to the retrospective nature of the case–control study design. We were also limited by our inability to gather direct information on the dose and type of asbestos that subjects were exposed to. Nonetheless, we were able to indirectly estimate dosage using duration of work at occupations where asbestos exposure occurred. Despite our inability to discriminate exposure by form of asbestos, it should be noted that IARC considers all types of asbestos to be carcinogenic and, moreover, we would likely have had insufficient statistical power to assess risk associated with individual subtypes. Regardless, future studies should aim to quantify the magnitude of risk associated with the various forms of asbestos with respect to pharyngeal and laryngeal cancer.
These observations are consistent with the mounting evidence that asbestos is a risk factor for pharyngeal cancer. Despite its known toxicity, asbestos is not universally banned and is still in use, particularly in developing countries. Continued efforts to study the health effects of asbestos are still indicated and have clear implications for policy and risk assessment.
References
Footnotes
-
Contributors All authors contributed to the conception, design, analysis and interpretation of data and to drafting the article or revising it critically for important intellectual content.
-
Funding This work was supported by the National Cancer Institute (R01CA121147, R01CA100679 and R01CA078609 to KTK), National Institute of Environmental Health Sciences (T32ES07272 to SML) and National Institute of Occupational Safety and Health (K01OH009390 to KMA).
-
Competing interests None.
-
Ethics approval This study was approved by Brown University Institutional Review Board, and the Institutional Review Boards of each participating medical institution.
-
Provenance and peer review Not commissioned; externally peer reviewed.