Article Text

Abstract
It has been suggested that certain types of work may increase the risk of common mental disorders, but the exact nature of the relationship has been contentious. The aim of this paper is to conduct the first comprehensive systematic meta-review of the evidence linking work to the development of common mental health problems, specifically depression, anxiety and/or work-related stress and to consider how the risk factors identified may relate to each other. MEDLINE, PsychInfo, Embase, the Cochrane Collaboration and grey literature databases were systematically searched for review articles that examined work-based risk factors for common mental health problems. All included reviews were subjected to a quality appraisal. 37 review studies were identified, of which 7 were at least moderate quality. 3 broad categories of work-related factors were identified to explain how work may contribute to the development of depression and/or anxiety: imbalanced job design, occupational uncertainty and lack of value and respect in the workplace. Within these broad categories, there was moderate level evidence from multiple prospective studies that high job demands, low job control, high effort–reward imbalance, low relational justice, low procedural justice, role stress, bullying and low social support in the workplace are associated with a greater risk of developing common mental health problems. While methodological limitations continue to preclude more definitive statements on causation between work and mental disorders, there is now a range of promising targets for individual and organisational-level interventions aimed at minimising mental health problems in the workplace.
Statistics from Altmetric.com
Introduction
Mental disorders have now replaced musculoskeletal problems as the leading cause of sickness absence and long-term work incapacity in most developed countries.1–4 The majority of mental ill health seen in the workforce is due to common psychiatric problems, such as depression, anxiety and other stress-related conditions, which are usually treatable and in some cases may be preventable.5–8 The rising costs of common mental disorders among the working population has created a major public health problem, with policymakers and health professionals increasingly demanding a better understanding of the links between modern work and mental health. The key issue of how work may contribute to the development of depression and anxiety is crucial to any consideration of the mental health of the working age population. Over the last 30 years, various work stress models have aimed to elucidate the complex relationship between psychological well-being and the workplace.9 ,10 While each of these models propose that a particular type of work ‘stress’ leads to an increase in mental disorders, the literature has continued to expand to include other potential work-related causal factors, including the type of work environment, level of job security, health perception, as well as the worker's cognitive ability and coping strategies and the availability of adequate social support.11–17
Despite increasing public, policy and academic interest, it is apparent that a consensus regarding which work factors influence mental health has not been reached. While there are reviews addressing specific work-related factors independently, an overarching review which collectively examines the influence of all relevant work factors on mental health has not yet be conducted. To address this issue, the present study aimed to undertake a detailed systematic meta-review on how work factors may contribute to the development of depression and anxiety disorders and symptoms. To the best of our knowledge, this is the first meta-review to be published in this topic. In addition to accurately summarising the current evidence base, the present review also aimed to examine how different workplace risk factors or risk models may overlap or be able to be combined into a more unified model.
Methods
Search strategy
A meta-review is a method of systematically appraising the results of existing reviews.18 Systematic searches were conducted in MEDLINE, PsychInfo and Embase electronic databases as well as Cochrane Collaboration Summaries. A comprehensive range of subject headings and key words combining mental health, work and review were devised for each database (see online supplementary file for the full search strategy). Grey literature was also systematically searched via the literature database ‘Open Grey’. In addition, subject matter experts were contacted with a request for any reviews, either published or unpublished, which they thought may be relevant to this topic. The reference lists of all the included reviews were also scrutinised in order to identify any reviews that had not been captured. The search in all databases was completed on 4 April 2016. There is a continuum of mental health symptoms that can present in the workplace and in the past, many studies have considered a variety of common mental health problems, rather than specific disorders. In order to ensure that this review captures as much of the available evidence as possible, we used a relatively broad definition of common mental health problems, which included both established diagnoses, such as depression and anxiety, as well as work-related stress. Where possible, results were reported separately for these different conditions.
supplementary file
The criteria used for inclusion in this meta-review were:
Publication considered common mental health problems, specifically depression, anxiety and/or work-related stress;
The role of work or the workplace risk factors were considered;
Was a literature review, systematic review or meta-analysis;
Published in the English language;
Published after 1 January 1990.
Papers which only considered volunteer work or which focused exclusively on a single occupational group were excluded from this review.
Selection process
Two researchers independently analysed each title and abstract in order to exclude papers which did not meet the above inclusion criteria. Of the remaining studies, the full text was obtained and analysed independently by the same two researchers in order to establish their relevance. In order to achieve consensus, any disagreement about a study's inclusion at either stage was referred to the senior researcher (SBH) for consideration.
Appraisal of quality
A measurement tool for the assessment of systematic reviews, the AMSTAR,19 was used by two researchers to assess the scientific quality of each review selected for inclusion. This checklist consists of 11 questions addressing different reporting methodology issues, with a score of 0–4 reflecting low-quality research, 5–8 moderate and 9–11 high quality (see table 1 for a general description of each category). The AMSTAR has been shown to have excellent reliability (R²=0.96) and construct validity.19 However, some epidemiologists have criticised the use of quality checklists20 as the items primarily evaluate the reporting of the methodology, with only a few questions relevant to the methodological rigour of the systematic reviews. For this reason, we have reported on the methodological quality of the included reviews throughout, with particular focus on the design of the studies (cross-sectional vs prospective), adjustment for potentially confounding variables and the measurement of exposure and outcomes (self-report vs objective).
Description of low, medium and high-quality studies
Overlap of primary research studies between reviews
In order to quantify any redundancies in the findings of the at least moderate-quality reviews, the primary research studies included were compared. Our reasons for limiting this assessment to the at least moderate-quality reviews are that those of low quality tended to provide little to no information about the included studies. The number of primary research studies that were included in more than one review was reported for each of the workplace risk factors, as a percentage of the total number of studies.
Development of a more unified model
As noted above, we felt it was important to attempt to bring the results of this meta-review together in the form of a new, more integrated model of the various risk factors identified. In order to achieve this, once the list of risk factors considered to have a reasonable evidence base was constructed, the authors of this review came together to examine how the concepts captured by each risk factor may overlap. Various models were proposed and debated within the group, with this iterative process continuing until a consensus was reached.
Results
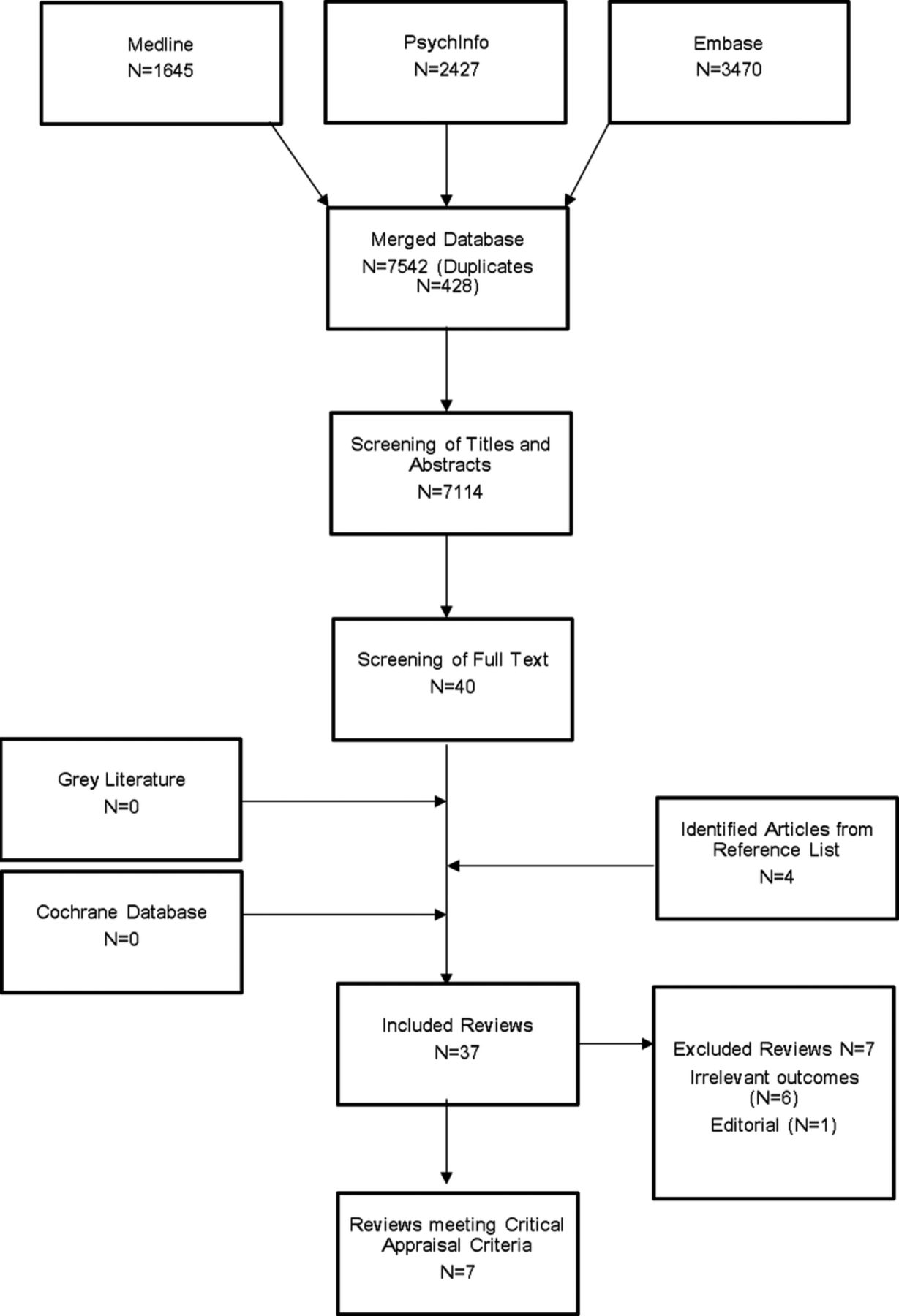
The initial systematic search identified 7542 potential academic papers and reports. Of these, 40 full texts were screened and 37 reviews (including 4 new articles from the reference lists) were found to meet the inclusion criteria. Seven review studies met the methodological assessment criteria of being at least of moderate quality (see online supplementary file for AMSTAR checklist scoring of all included systematic reviews).21–27 The details of these reviews are shown in table 2. In total, these reviews analysed 213 primary research studies, with evidence of only minimal overlap between the reviews for which the workplace risk factors assessed by each study could be clearly identified. Of the other 30 included reviews, all of which were rated as low quality, 12 were systematic reviews28–33 or meta-analyses,34–39 with the rest being narrative reviews. Six reviews were excluded during the full-text screening due to irrelevant outcomes,40–45 and one paper was excluded because it was an editorial rather than a review.46 The complete study selection process is summarised in figure 1. Twelve work-related risk factors were identified among the included reviews; high job demand, low job control, low workplace social support, effort–reward imbalance (ERI), low organisational procedural justice, low organisational relational justice, organisational change, job insecurity, temporary employment status, atypical working hours, workplace conflict/bullying and role stress.
Moderate or high-quality reviews that address how work contributes to the development of common mental health problems
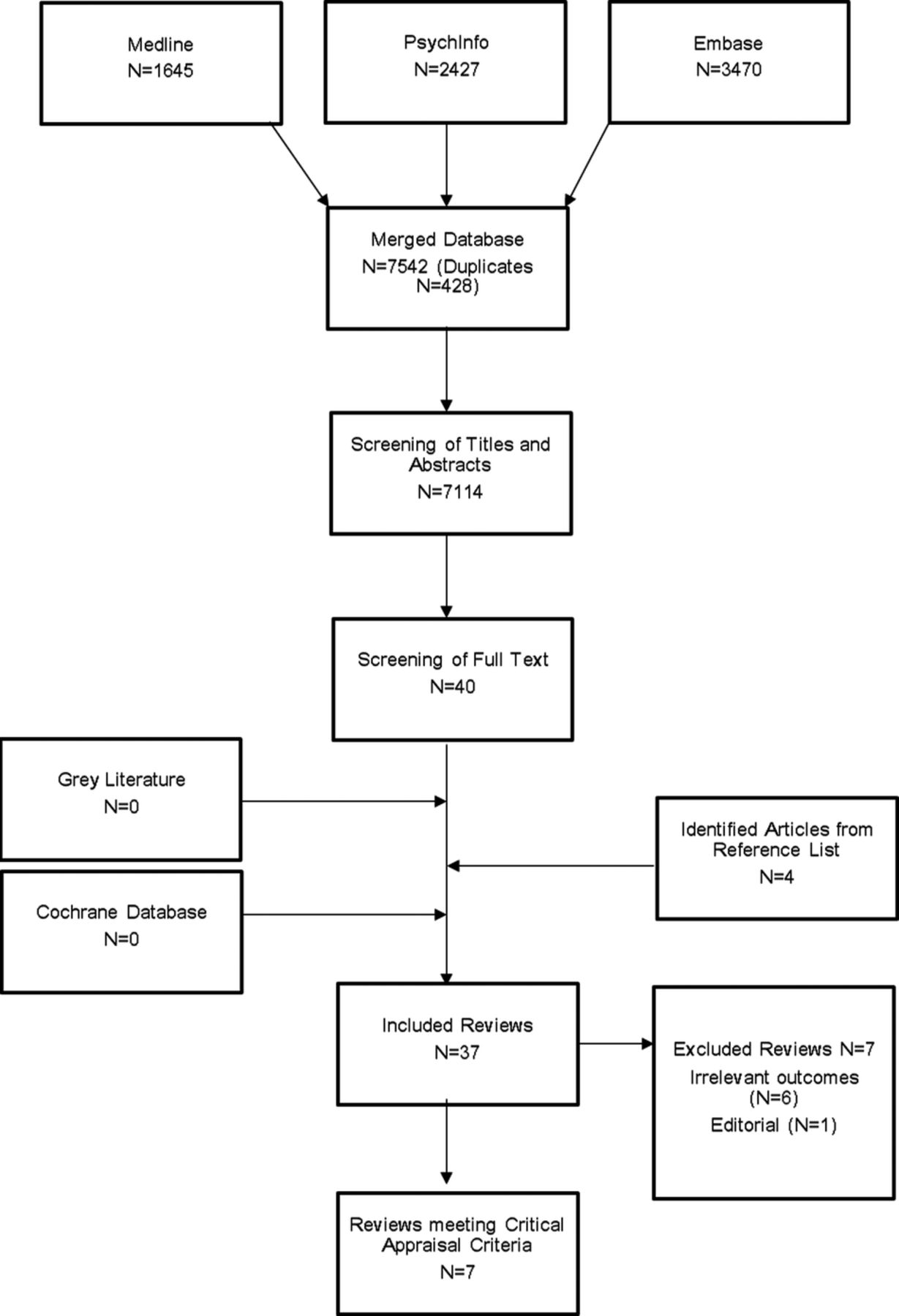
Flow chart of study selection.
The job demand–control–support model
The job demand–control–support (JDCS) model (previously termed the job demand–control model) proposes that jobs where high demands (increased workload/time pressure) are combined with low control (minimal decision-making) create a ‘high-strain’ situation and bear the greatest risk of illness and reduced well-being.9 Some researchers have extended this model and propose that high social support in the workplace may moderate the adverse impact of high-strain jobs.47 Our meta-review found four moderate-quality reviews that provided good evidence for a prospective association between high job demand, low job control and low social support and poorer employee mental ill health.21 ,24–26 It was difficult to determine the number of primary research studies that were included in more than one review due to differences in reporting of the workplace risk factors assessed. However, out of a total of the 42 primary research studies that could be clearly accounted for, only 7 were included in more than 1 review (17% overlap).
A meta-analysis of nine studies by Stansfeld and Candy26 found that an employee's risk of common mental disorders could be predicted by low job control (Summary OR=1.23), high psychological demands (OR=1.39) and low occupational social support (OR=1.32). While a high degree of heterogeneity was reported regarding psychological demands and social support, this review appraised the quality of all the primary research identified and only included high-quality longitudinal studies in the final meta-analysis, thereby adding strength to the overall findings. Another meta-analysis by Theorell et al,21 which included only prospective studies that had passed their quality assessment, found mixed evidence in support of the JDCS model. They reported moderately strong evidence, using the GRADE approach, for an association between either high job strain or low job control and increased depression symptoms. In addition, Nieuwenhuijsen et al's24 systematic review of three studies, all of which were prospective cohort studies, found that high job demands, low job control and low support from colleagues and supervisors predicted the occurrence of stress-related disorders and adjustment disorders. Another systematic review by Netterstrom et al25 focused specifically on how these factors may contribute to the development of depression. Of the nine longitudinal studies examined, the reviewers found moderate evidence for a relationship between high psychological demands and low social support in the workplace and the development of depression. However, the reviewers acknowledged that an indication of publication bias weakens these findings and that these psychosocial factors are frequently measured in different ways across studies, thus limiting interpretation and generalisability.
The search strategy also identified two additional systematic reviews which investigated the effect of ‘high strain’ jobs on an employee's mental health, but which were deemed to be of low methodological quality.28 ,30 One of these reviews had methodology that rated very close to the ‘moderate’ quality cut-off.28 This review reported an increased risk of depressive disorder in the setting of high job demands, low decision latitude and low levels of social support. While this review only included longitudinal studies and considered studies in which participants met clinical criteria for depression (as opposed to self-report symptom measures), it was limited by a lack of information on how the literature search was performed and how the methodological quality of studies was assessed. However, in spite of these limitations, the results described are comparable to those of other reviews.
ERI model
The ERI model is based on the worker's experience of the balance between effort made at work and the reward received.48 This model proposes that the most stressful work condition is the one in which the work reward does not match the effort made. Three reviews of moderate quality explored the influence of high ERI on the mental health of workers. In total, these reviews included eight primary research studies, out of which only two were included in more than one review (25% overlap). In their meta-analysis, Stansfeld and Candy26 concluded that high ERI is strongly associated with an increased risk of common mental disorders (OR=1.84, 95% CI 1.45 to 2.35). While this finding was based on only two studies, the primary studies were longitudinal in nature with a combined sample of over 12 000 employees, lending considerable weight to their conclusions. Similarly, Nieuwenhuijsen et al24 found a significant association between high ERI and stress-related disorders (including adjustment disorder) in the workplace. These results support a body of primary research which suggests that increased ERI in the workplace is associated with a greater risk of developing depression and anxiety disorders.49–51 Despite these findings, few studies have explored the impact of ERI on the development of depression and anxiety disorders specifically rather than the broad grouping of common mental disorders. One moderate-quality meta-analysis of three prospective studies was identified that found limited evidence for a relationship between ERI and increased depression symptoms.21
Organisational justice model
Organisational justice refers to the fairness of rules and social norms within companies, specifically in terms of resources and benefits distribution (distributive justice), the methods and processes governing that distribution (procedural justice) and interpersonal relationships (interactional justice).52 Interactional justice comprises two elements: relational justice, the level of respect and dignity received from management and informational justice, the presence or absence of adequate information from management about workplace procedures. In this meta-review, two moderate-quality reviews and one low-quality review were found that explore this relationship, with the majority of included studies focusing on relational justice and procedural justice. Only one of the six primary research studies referenced were included in more than one of the moderate-quality reviews (17% overlap).
A moderate-quality review by Nieuwenhuijsen et al24 found that low relational justice and low procedural justice were strongly associated with an increased likelihood of stress-related disorders including adjustment disorder. Although this was based on a single paper, it reported on two prospective cohort studies with very large (n>4000) samples and analyses that adjusted for potential confounding variables, thereby strengthening their conclusions. In contrast, a moderate-quality meta-analysis of five prospective studies by Theorell et al,21 which focused only on depression symptoms, found more limited evidence for an impact of either procedural or relational justice.
The low-quality systematic review of 11 prospective studies by Ndjaboue et al33 found that low procedural justice and low relational justice were associated with increased likelihood of mental health problems among employees and that this relationship existed independently of factors examined in the DCS and ERI models. In spite of these methodological strengths, the absence of an assessment of the methodological quality of the included studies and the lack of a meta-analysis reduced the AMSTAR quality score. Nonetheless, this review highlights organisational justice as a unique and important construct that may influence the mental health of employees.
Organisational change and job insecurity
Employees are increasingly subject to organisational change that can range from technology and management changes to downsizing or restructuring. A low-quality systematic review by Bamberger et al included 17 studies that assessed various types or organisational change including downsizing, relocation, mergers and increases in workload. Data were collected primarily by administering questionnaires to workplaces exposed to organisational change. Eleven of 17 included studies observed a negative relationship between organisational change and mental health.32 This association was weaker in the longitudinal studies included in this review, suggesting that a time-effect may exist or that confounding psychosocial factors or reverse causality around the time of change may influence the relationship between organisation change and mental health. This study received a low-quality AMSTAR score, primarily due to the lack of a methodological quality assessment of the included studies and the absence of a meta-analysis, but its conclusions are strengthened by this comparison between the results of the included cross-sectional and longitudinal studies.
Organisational change or external economic factors may also lead to a perception of job insecurity. Two moderate-quality reviews were identified by the systematic search that explored the effects of job insecurity on mental health. In total, these reviews included 10 primary research studies, none of which were included in more than 1 review (0% overlap). A moderate-quality meta-analysis examined three studies that assessed the impact of job insecurity on common mental disorders and reported a moderate-sized OR of 1.33 (95% CI 1.06 to 1.67).26 In contrast, based on the results of their moderate-quality meta-analysis of seven prospective studies, Theorell et al21 concluded that there was limited evidence for an association between job insecurity and depression symptoms. An additional meta-analysis examining the consequences of job insecurity was identified; however, it was rated as low methodological quality for a number of reasons such as the characteristics of the included studies not provided and there not being assessment of included studies methodological quality.35 This meta-analyses reported a medium population effect size between job insecurity and mental health of r=−0.2 (corrected for attenuation).
Employment status and atypical working hours
Temporary employment arrangements are increasingly common in developed countries.27 A meta-analysis by Virtanen et al included 27 studies, 14 of which were prospective studies, examined the association between temporary employment and mental health. The researchers reported that temporary employees have higher psychological morbidity, a term not operationalised in this particular review, compared with permanent employees (OR=1.25).27 However, limited inferences can be drawn from this finding due to the high levels of discrepancy between the included studies on measures such as health outcomes and type of temporary employment. Furthermore, it is likely that people with mental health problems are more often provided with temporary employment arrangements compared with healthy individuals. Therefore, the higher frequency of mental health problems among those with temporary employment may only be a result of work opportunities rather than the impact of job instability.
Three reviews were identified that investigated the relationship between atypical working hours and mental health problems. Theorell et al's21 moderate-quality meta-analysis of six prospective studies demonstrated limited evidence of an association between having a long working week and increased depression symptoms. However, the authors did not provide an operational definition of ‘long working week’, and so it is difficult to draw conclusions based on this result. Two low-quality reviews also examined the influence of long working hours and shift work on psychiatric symptomatology. A meta-analysis of 19 studies showed that working 48 hours or more per week had a small but significant correlation with psychological health (r=0.15).34 Similarly, a systematic review of three cross-sectional and four prospective studies concluded that working more than 40 hours per week or 8 hours per day increased the risk of developing symptoms of depression and anxiety.31 However, there are serious methodological limitations to these reviews, including a failure to differentiate between long working week and shift work in the meta-analysis,34 and the lack of an evaluation of the quality and/or heterogeneity of the included studies.31 ,34 No systematic reviews or meta-analyses that examined the impact of shift work were identified, but a narrative review of a few selected studies concluded that there was no association between either irregular work schedules or night shifts and mental disorders.53
Workplace conflict and bullying
Workplace conflict arises when disliked or injurious actions are perpetrated against an employee and, if this persists over a long period of time, it can progress to workplace bullying. Our meta-review search strategy identified five meta-analyses (two of moderate quality and three of low quality) that examined the influence of workplace conflict and bullying on the development of psychiatric symptomatology. In total, these moderate-quality reviews included 64 primary research articles, of which 2 were included in more than 1 review (3% overlap). A moderate-quality meta-analysis by Theorell et al21 found moderately strong evidence for an association between workplace bullying and increased depression symptoms. While only three prospective studies were included in the meta-analysis, the resulting effect was of a relatively large magnitude (weighted OR 2.82; 95% CI 2.21 to 3.59). In contrast, there was limited evidence for an impact of workplace conflict with superiors or coworkers on depression, based on the three prospective studies included.21 Verkuil et al22 also conducted meta-analyses on the relationship between workplace bullying and mental health problems; however, the researchers included cross-sectional and longitudinal data. They revealed that workplace bullying predicted increased symptoms of depression, anxiety and stress-related psychological symptoms in the 48 cross-sectional samples (r=0.36; p<0.001), as well as the 22 longitudinal samples (r=0.21; p<0.0001). In addition, a reversed association between mental health problems at baseline and workplace bullying at follow-up was also shown using a small number of studies (r=0.18; p<0.0001). However, a number of studies included were not able to account for residual confounding and there was substantial heterogeneity between studies which was compounded by the researchers' method of averaging the correlation coefficients of the multiple outcomes of interest to create a single mental health outcome. Four low-quality meta-analyses also reported significant relationships between workplace bullying and mental health problems.36–39 While their results are largely consistent with that of the moderate-quality meta-analyses, they are limited for various reasons such as a failure to operationally define the concept of workplace aggression,38 the exclusive use of a personal database to identify studies36 and the absence of assessments on the quality and/or heterogeneity of included studies.36–39
Role stress
More recently, studies have also considered the impact of role stress. Two of the most researched types of role stress are role ambiguity (when an employee lacks information about their role's responsibilities and objectives) and role conflict (when there are two or more opposing expectations about an employee's role). Only one moderate-quality meta-analysis of 32 studies explored the impact of role stress on mental health.23 Schmidt et al found that role conflict (r=0.3; p<0.001) and role ambiguity (r=0.3; p<0.001) were related to increased depression symptoms. There was a moderate intercorrelation between these two risk factors, although repeating the meta-analysis controlling for the influence of the other increased the size of the coefficients. The findings of Schmidt et al23 are strengthened by their comprehensive search strategy, which aimed to capture non-English articles, doctoral dissertations, conference booklets and experts' unpublished results. However, the possibility of reverse causation cannot be excluded, as only one longitudinal study was identified.
Discussion
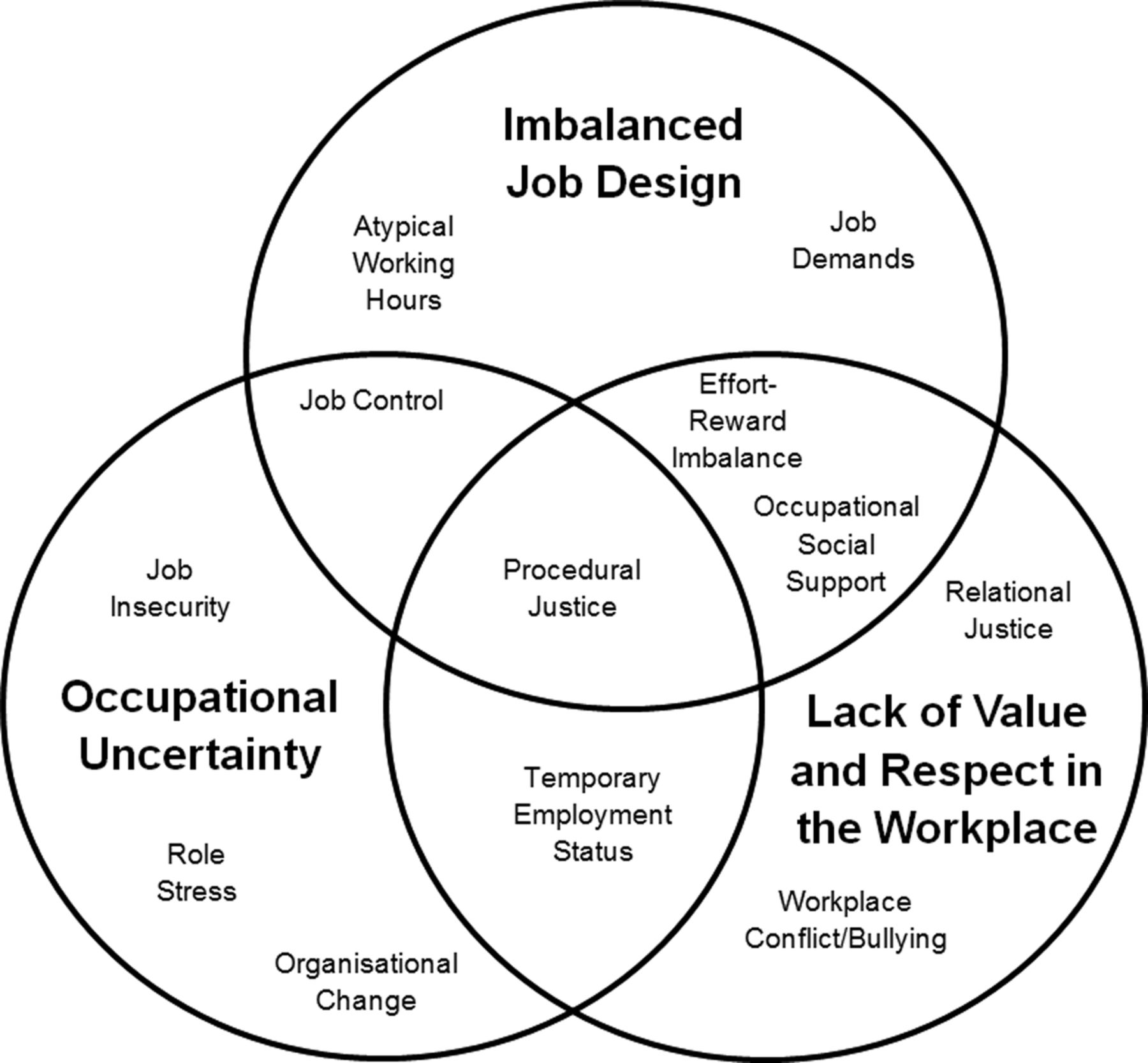
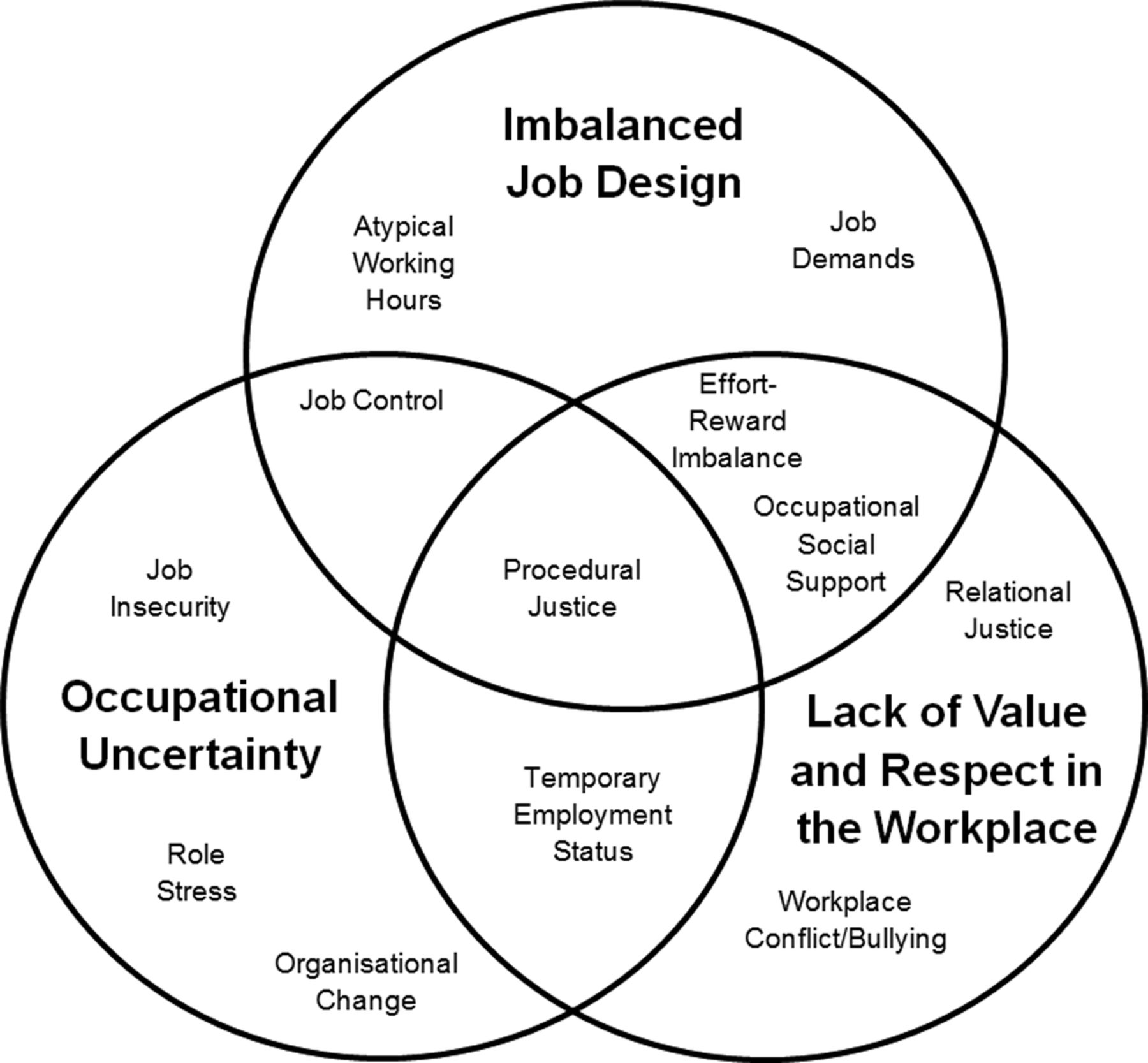
The question of how modern work may contribute to the development of common mental disorders has been the source of considerable debate and discussion over recent decades.11 This review brings together and systematically summarises, for the first time, the vast amount of academic literature that has been published on this topic. Based on a systematic search, 12 work-related risk factors were identified with reasonable levels of evidence for an association with increased rates of common mental health problems; high job demand, low job control, low workplace social support, ERI, low organisational procedural justice, low organisational relational justice, organisational change, job insecurity, temporary employment status, atypical working hours, bullying and role stress. The question of how these factors and separate models relate to each other can now be considered. It seems likely that some of the risk factors identified in this meta-review are measuring overlapping constructs, raising the possibility of a smaller number of upstream latent variables that are responsible for any links between work and mental ill health. The bringing together of the various models relating to workplace mental health is arguably long overdue. The present situation, where individual models are often considered in isolation, leads to employers or policymakers having an ever-increasing list of potential workplace variables they need to address. Based on the findings of this review, we propose a more unifying model of the psychosocial workplace with three overlapping clusters of workplace risk factors; imbalanced job design (incorporates job demands, job control, ERI, occupational social support), occupational uncertainty (job control, procedural justice, organisational change, job insecurity, temporary employment status) and a lack of value and respect within the workplace (ERI, procedural justice, relational justice, temporary employment status, occupational social support). A diagrammatic representation of this proposed unifying model is shown in figure 2.
{kind=link}
{kind=link}
Unifying model of workplace risk factors.
The use of meta-review methodology enabled this review to cover a breadth of topics concerning work and mental health that would be difficult to cover with standard systematic review techniques. However, there are a number of limitations inherent with this method of systematic review. Most notably, a meta-review can only report on literature that has been previously been captured in published or grey literature reviews, meaning recently published primary research studies that are not yet summarised in a review are not included. For this reason, meta-reviews are only appropriate for the study of areas that are sufficiently developed to have produced a comprehensive range of reviews. The wide variety of reviews captured by our systematic search suggests that workplace mental health was an appropriate topic for a meta-review. Despite conducting a comprehensive literature search and contacting experts in the field for any missed published or unpublished reviews, we acknowledge that the risk of publication bias remains. In particular, it is possible that negative reviews and negative primary research are less likely to be published, both of which would increase the chance of overestimating the impact of workplace risk factors.54 For practical reasons, we also limited the search strategy to English publications, and so there may have been non-English reviews examining this research question that were not identified. Additionally, in a meta-review, there may be substantial overlap in terms of the primary research studies included in the subsidiary reviews. Our attempts to determine the number of primary research papers that were cited in more than one included systematic review revealed only minimal overlap.
There are also a number of limitations within the primary research studies reported in the included reviews that are important to note. First, there was a tendency for researchers to be overly reliant on self-report symptom questionnaires when measuring rates of mental illness, which cannot be considered equivalent to diagnosable mental disorders. Similarly, self-report questionnaires were also often used to examine risk factors in the workplace. When an employee describes the characteristics of their own job or workplace, their appraisal will incorporate a range of individual beliefs, perceptions and attitudes to work.55 Therefore, it may be that personal or individual factors, such as perception of health and vulnerability,17 attitudes towards work,56 educational attainment16 and personality,57 may alter an employee's ability to accurately rate work-related factors and their risk of future mental illness. Reverse causation is also a possibility via early life mental illness increasing the risk of an individual finding themselves working in a suboptimal environment. Stansfeld et al58 have previously used life course data from birth cohort data to show that mental health symptoms in childhood and early adulthood did indeed predict adverse working conditions in adulthood, but this did not explain the association between work characteristics and depression and anxiety symptoms in adult life. Other studies have compared self-report and coworker measures of the work environment to assess the importance of reporting bias, though these results have been mixed, with some showing similar associations with mental health outcomes using both measures,59 and others finding that self-report measures inflate the association between work characteristics and mental health outcomes.60 Finally, while a number of longitudinal studies were identified, the long-term impact (beyond 2 years) of workplace risk factors on employee mental health remains unknown.
The results of this meta-review, when taken together with the methodological concerns outlined above, suggest that four conclusions can be drawn regarding the relationship between work and common mental disorders. First, there is now consistent evidence that certain work situations are associated with an increased risk of common mental disorders. Specifically, there is at least moderate level evidence from multiple prospective studies that high job demands, low job control, high ERI, low relational justice, low procedural justice, role stress, bullying and low social support in the workplace are associated with a greater risk of developing depression and anxiety symptomatology. However, while the evidence for a prospective relationship is strong, the methodological issues outlined about, preclude definite statements about casual inference. A previous systematic review came to similar conclusions 7 years ago,28 but unfortunately similar methodological problems have continued. Second, there are a range of other work-related factors, including low distributive justice, low informational justice, organisational change, job insecurity, temporary employment status and atypical working hours which appear likely to be important risk factors, but which require further methodologically robust assessment to conform their role as independent risk factors. Third, while there does not appear to be one common ‘toxic factor’ among the variety of work-related risk factors identified, overlapping concepts are beginning to appear, as outlined in our proposed new unifying model (figure 2). Finally, it is likely that work-related risk factors interact with individual personality characteristics, attitudes and coping styles to produce specific mental health outcomes, although to date the majority of research has not adequately considered this. While better designed observational studies may be able to address residual confounders and interactions, it is likely that randomised controlled trials assessing whether altering these risk factors leads to differing rates of mental disorder provide the best hope of more certainty regarding causative relationships.
There is increasing interest in the notion of preventing common mental disorders,61 with some suggesting that the workplace is an obvious domain in which prevention strategies should be focused.8 While strategies to improve individual levels of resilience have received much attention,62 ,63 any intervention programme should also include efforts to reduce known risk factors. The work-based risk factors identified in this review should be the starting point for developing such interventions. To date, interventions studies have tended to focus on only one of the risk factors identified in this review, job control. The possibility of other types of interventions being developed to address some of the additional risk factors identified in this review needs urgent consideration.
For most individuals, being employed and at work improves their mental health and well-being.64 Given this, our results should not be interpreted as suggesting those with or at risk of mental disorder need to avoid work. On the contrary, we hope this clarification around the role and overlap of various work-based risk factors will allow the development of interventions that will allow the workplace to be more promoting of good mental health.
Acknowledgments
The authors wish to thank Natalia Yee and Jane Forster for their assistance in carrying out the systematic search and Nick Arvaniti (Beyondblue) for his assistance throughout the project.
References
Footnotes
Contributors SBH devised the study, with assistance from AM, RAB, HC and PBM. MM, SJ and JSM-S designed and carried out the systematic literature search under the supervision of SBH. SBH, MM, SJ, JSM-S and LT analysed and interpreted the data, and wrote the first draft of the manuscript. AM, RAB, HC and PBM contributed detailed academic input to subsequent versions. All authors approved the final manuscript.
Funding Funding for this project was provided by Beyond Blue Limited ACN 093 865840, who are an Australian-based mental health charity, as part of a larger project. The authors remained independent of the funders in their reporting of results.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.