Article Text

Abstract
Objectives To investigate patterns of alcohol use within the coal mining industry, and associations with the personal, social, workplace and employment characteristics.
Design 8 mine sites across 3 eastern Australian states were surveyed, selected to encompass key geographic characteristics (accessibility and remoteness) and mine type (open cut and underground). Problematic alcohol use was measured using the Alcohol Use Disorders Identification Test (AUDIT) to determine: (1) overall risky or hazardous drinking behaviour; and (2) frequency of single-occasion drinking (6 or more drinks on 1 occasion).
Results A total of 1457 employees completed the survey, of which 45.7% of male and 17.0% of female participants reported levels of alcohol use within the range considered as risky or hazardous, considerably higher than the national average. Hierarchical linear regression revealed a significant contribution of many individual level factors associated with AUDIT scores: younger age, male, current smoking status; illicit substance use; previous alcohol and other drug use (AOD) problems; and higher psychological distress. Workplace factors associated with alcohol use included working in mining primarily for the high remuneration, and the type of mining, with underground miners reporting higher alcohol use than open-cut miners.
Conclusions Our findings provide support for the need to address alcohol use in the coal mining industry over and above routine on-site testing for alcohol use.
- Mining
- Workplace Health
- Illicit drugs
Statistics from Altmetric.com
What this paper adds
Substance use problems are a leading cause of global disability, and represent a substantial economic burden.
No previous study has examined both the patterns of alcohol and other drug use within the Australian coal mining industry, and the associated personal, social, workplace and employment characteristics.
In total, 45.7% of male and 17.0% of female participants reported levels of alcohol use within the range considered as risky or hazardous, considerably higher than the national average.
Our multivariate analysis showed that a complex interplay of factors, including a combination of personal individual factors, as well as a number of workplace and employment factors were associated with alcohol use.
These results provide evidence to inform the development of specific workplace strategies to address problematic alcohol use within the mining industry and male-dominated industry more broadly.
Introduction
Substance use problems and related disorders are a leading cause of global disability and account for an estimated 4.3% of the Australian disease burden.1 Workplace concerns about substance use have traditionally focused on the links between substance use and workplace injury.2 While there are inconsistencies in the literature, there is some evidence to suggest a linkage between alcohol use and absenteeism, presenteeism (suboptimal productivity while at work)3 and more frequent interpersonal and disciplinary problems (see ref. 4 for review).
A compelling body of evidence has shown that the prevalence of alcohol-related problems is significantly higher in male-dominated industries, specifically construction,5 ,6 police services7 and transport6 industries. In Australia, mining is a male-dominated, high-income industry, and currently employs ∼2% of the national population,8 with coal the largest export earner in New South Wales (NSW) and Queensland (QLD). In terms of safety, evidence shows that the Australian coal mining industry is associated with less loss-time injuries than in the USA.9 The Australian mining industry has invested significant resources to address the impact of alcohol consumption on the health and safety of employees. Comprehensive systems are in place to control alcohol usage, including mandatory breath testing as part of the logging on process prior to shift start, and the requirement of a blood alcohol concentration (BAC) of 0.00 g/100 mL. Many workplaces also routinely perform random illicit drug testing.10 While these policies reflect an understanding of the need to improve workplace safety, they do not address workplace factors that maximise workplace opportunities to promote the mental and physical health of employees (which includes substance use).
Among the first to investigate alcohol use within the Australian mining industry, Lennings et al,11 in a study of a single-mine site, identified high levels of alcohol use among employees compared with the general population. More recently, evidence has emerged that miners who work in ‘fly-in fly-out’ (FIFO) or ‘drive-in drive-out’ (DIDO) operations (ie, their workplace is remote to their home residence, and they live on a mine site during rostered periods) are more likely to drink alcohol at risky levels than those in other employment types.12 Research until now has identified a substantial problem in this industry, but there has been limited attention to the relative contribution of work characteristics to these patterns of alcohol use. Such information is important to guide industry-based policy that can support prevention and early intervention initiatives targeting substance use.
The mining industry is diverse and complex. Most mines operate 24 hours, 7 days per week, and employees often work long hours (ie, 12 hours or longer shifts),13 with rosters that are both rotating (work periods that consist of both day and night shifts)13 and compressed (a high number of shifts over consecutive days). Mines are often located in isolated regions, where employees are separated from family and social support networks, and the availability of professional support services is limited.14 Consequently, employees typically face challenges such as: long working hours, shift work, geographical isolation, limited contact with families and social supports, and a highly demanding role. Little is known about how these factors influence patterns of alcohol or other drug use. While the psychosocial, physical and organisational characteristics may present risks to health, the workplace has the opportunity to support health-promoting behaviours and risk-mitigation strategies that can enhance health outcomes.15 Such workplace strategies require attention to the interaction of workplace characteristics, the work–family–community interface and individual behaviours.15
Linked to such an approach, the workplace psychosocial safety climate (PSC) model16 provides a broad theoretical framework for consideration of the workplace characteristics related to health outcomes, including management/organisational support, specific job demands and resources. This study aimed to better understand factors associated with alcohol use within the coal-mining industry, including a range of personal, social, workplace and employment characteristics within the PSC framework, with the aim of informing workplace health policy and interventions. This work aligns with the development of an industry-based Blueprint for Mental Health, as a national planning framework to promote mental health and well-being in the mining and resources sector of Australia.17
Methods
This research was approved by the Human Research Ethics Committee, University of Newcastle (H-2013-0135).
Setting and sample
Mines
Using quota sampling, sites were selected to ensure a representative cross-section of the coal mining industry. Stratification variables included location (NSW and QLD), mine type (underground or open cut) and employee commute arrangements (daily or long distance commute (ie, FIFO/DIDO)).
Mine recruitment
Consent was obtained at the company level first, primarily through occupational health and safety managers. Consent was then requested at the individual mine level, whereby a member of the research team visited sites to provide an overview of the project to mine management. Once approved, the research team organised data collection logistics with key delegates from each mine.
Participant recruitment and data collection
The data collection methodology was designed to accommodate the unique logistical considerations of each site, while minimising disruption to production. Where available, sites participated as a component of their routinely scheduled training/utility days, which are rostered days allocated for staff development. Across all other sites, data collection occurred while participants were on shift, or during their daily preshift meetings. All staff participated in the research during their rostered hours.
Two weeks before starting data collection, each mine was sent promotional materials (eg, PowerPoint slides, information flyers) to be displayed in employee common areas. The data collection process involved a member of the research team visiting the site and providing all participants with a written information statement and a brief presentation outlining the purpose of the research. This material stated that the research was voluntary, confidential and that participants were free to withdraw at any time. Participation involved completing a 15 min pen-and-paper survey, with the return of a completed survey considered implied consent. Participants were asked to provide a self-generated code (consisting of initials and day/month of birth), to allow potential linkage with future surveys.
Data collection occurred between December 2013 and March 2015.
Measures
Elements of the workplace PSC model16 provided a broad theoretical framework for the assessment domains in this study. This model postulates that employees' work and health outcomes are influenced by a mixture of factors including management/organisational support, specific job demands and resources.
For the current analyses, four conceptually related sets of variables were used to examine associations with alcohol use: (1) sociodemographic factors; (2) health history; (3) participant's current health and (4) workplace factors and attitudes. This grouping reflected the aim of examining associations between problematic alcohol use and workplace factors and attitudes, after accounting for the effects of the other factors.
The majority of the standardised measures in the study are well established and have acceptable psychometric properties. For the Job Content Questionnaire, only the domains relating to job–strain ratio were included.
Outcome variables
Hazardous or harmful drinking
Alcohol use within the past 12 months was measured with the 10-item Alcohol Use Disorders Identification Test (AUDIT), a widely used indicator of hazardous and/or harmful drinking behaviour18 (α=0.80). This instrument combines measurement of the quantity and frequency of alcohol consumption, as well as the personal and social problems associated with alcohol use.
Single-occasion drinking
Single-occasion drinking (sometimes referred to as binge drinking) was defined as the consumption of more than five alcoholic drinks on one occasion. This was measured using an individual AUDIT item that asks participants to self-report the frequency at which they have ‘six or more drinks on one occasion’.
Independent variables
Sociodemographic factors
Demographic information collected included age, gender, number of dependent children and the highest level of education completed. Social network characteristics were measured using the Social Network Index (SNI) using conventional scoring criteria.19
Health history
Participants were asked if they had ever been diagnosed with depression, anxiety, drug and/or alcohol problems or a chronic physical condition (such as: heart attack, other heart disease, high cholesterol, high blood pressure, stroke, cancer, diabetes and/or obesity).
Current health
Current health included an assessment of behaviours that may impact on health, as well as current symptoms of mental health problems, comprising smoking status (categorised as: never smoked; ex-smoker; currently smoke, but less often than daily; or current daily smoker) and frequency of use of three categories of illicit drugs including (1) cannabis; (2) synthetic drugs (eg, Kronik, synthetic cannabis); or (3) other illicit drugs (with frequency categorised as: have never tried it; used, but not in the past month; or used in the past month).
Current mental health symptoms were assessed using the Kessler-10+ (K10+).20 Item scores on the K10+ were summed to give a possible cumulative score range of 10–50, with higher scores indicating greater psychological distress (α=0.89).
Workplace factors and attitudes
A set of workplace factors, as well as employees' attitudes towards working in the industry, were assessed as described in table 1.
Description of the workplace factors and attitudes measured
Data analysis
Data entry, aggregation and analysis were performed using Statistical Package for the Social Sciences (IBM SPSS V.22.0; Armonk, New York, USA).
The AUDIT was scored using conventional criteria,18 ,21 with each item scored from 0 to 4, giving a cumulative range of 0–40. Total scores were then categorised into four separate strata, including: no known risk (0–7); risky or hazardous (8–14); high risk or harmful (15–18); and high risk, dependence likely (19–40). The AUDIT includes three subscales22 including domain 1 (questions 1–3), which measures both the quantity and frequency of alcohol consumption; domain 2 (questions 4–6), which measures drinking-related behaviour; and domain 3 (questions 7–10), which measures lifetime negative consequences associated with alcohol use.
Descriptive analysis was used to characterise patterns of alcohol use, focusing on response frequencies, with χ2 analysis used where appropriate.
Hierarchical linear regression was undertaken to examine the contribution of independent variables to alcohol use, using a predetermined order of entry for associative variables. The order of entry reflected the aim of the research, which was to investigate the association between workplace factors and attitudes, and the two primary outcome variables ‘total AUDIT score’ and ‘single-occasion drinking’, after controlling for the effects of the participants': (1) sociodemographics; (2) health history and (3) current health. For all categorical variables, comparisons were based on a conceptual basis a priori, with variables coded using dummy variables to measure their association with AUDIT scores, as outlined in table 4.
As a partial control for the number of statistical tests, the α criterion was set at p<0.01.
Missing data
Since the AUDIT consists of multiple independent subscales, participants' data were excluded if they missed more than one question from any of the three domains. In cases where participants met the inclusion criteria, domain scores were based on averaged (or prorated) responses for the available items.
Results
Sample characteristics
Mines
Ten mine sites were approached and eight mines agreed to participate in the study. The non-participating mines could not allocate sufficient time during the data collection window. The final sample consisted of sites from NSW (5) and QLD (3), and included open cut (3) and underground mines (5). Three sites operated primarily through a DIDO arrangement, whereby most staff were transported to and from the site by bus, and then resided in purpose-built mine accommodation (camps) for the duration of their scheduled roster. The remaining five sites were considered ‘daily commute’, whereby most staff would drive to and from work each day, and live in their own personal accommodation.
Participants
A total of 1457 employees participated across the eight sites. Of the five sites where participation occurred during training days, 929 of the 982 employees consented to participate (average response rate: 95%, range 92–98%). For the remaining three sites, a participation rate was calculated by dividing the number of people who completed the survey by the total number of employees. Of the 2386 people employed across the three sites, 528 completed the survey (average participation rate 22%, range 18–30%).
Incomplete AUDIT scores resulted in the exclusion of 47 participants. Sample characteristics of the 1410 participants who completed the AUDIT are shown in table 2.
Sample characteristics of participants who completed the AUDIT (n=1410)*
Illicit drug use
Only a minority of participants reported current illicit drug use (table 2). While 35.8% indicated that they had used cannabis, of these, only 2.3% reported usage within the past month. Fewer participants reported use of synthetic cannabis or other illicit drugs.
Hazardous or harmful drinking
Overall, 95.7% of males and 89.8% of females reported that they drink alcohol (table 3). Over half (53.4%) of the males and a third of the females (34.6%) reported consuming alcohol at least 2–3 times per week.
Quantity and frequency of alcohol use, stratified by gender, % (n)
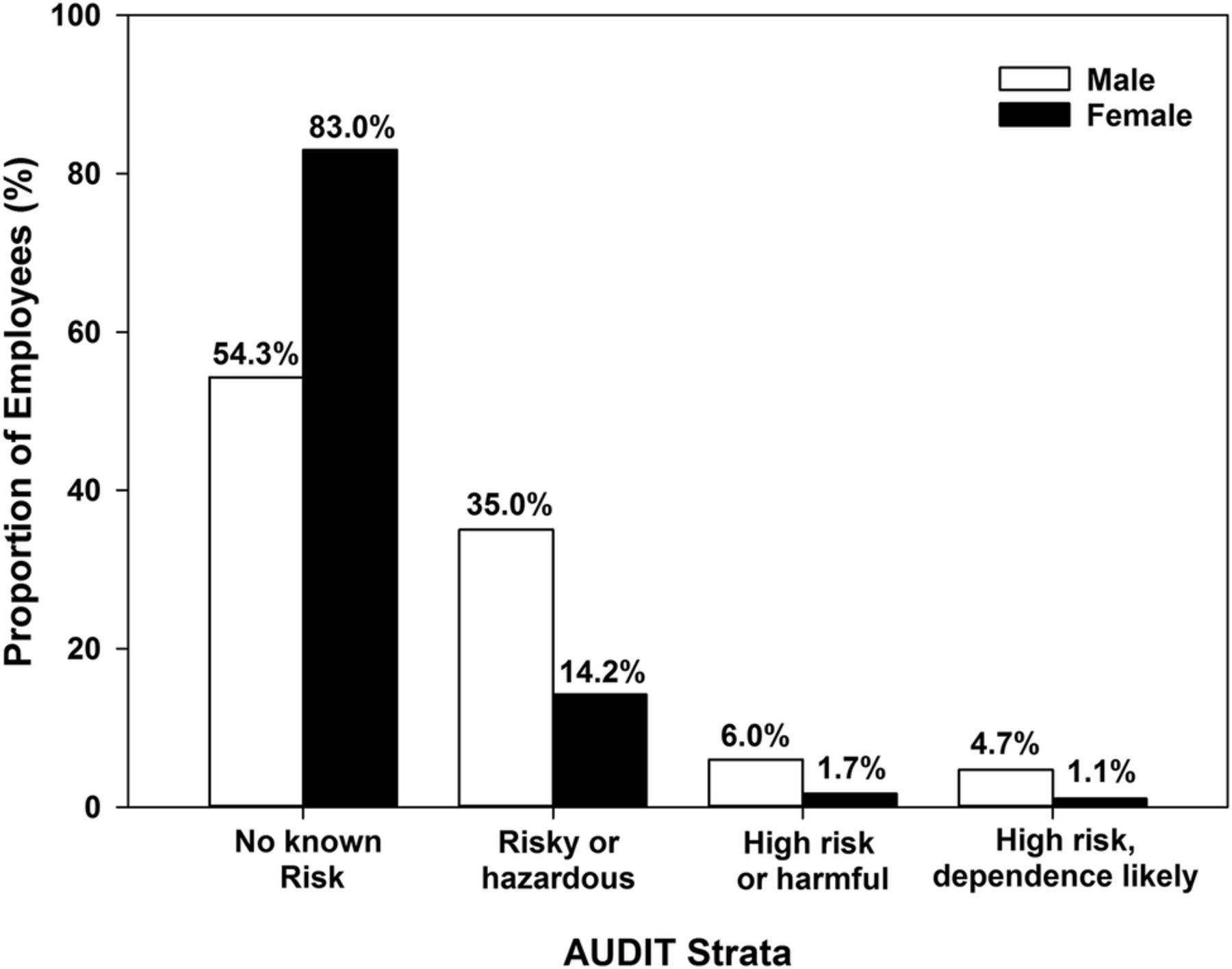
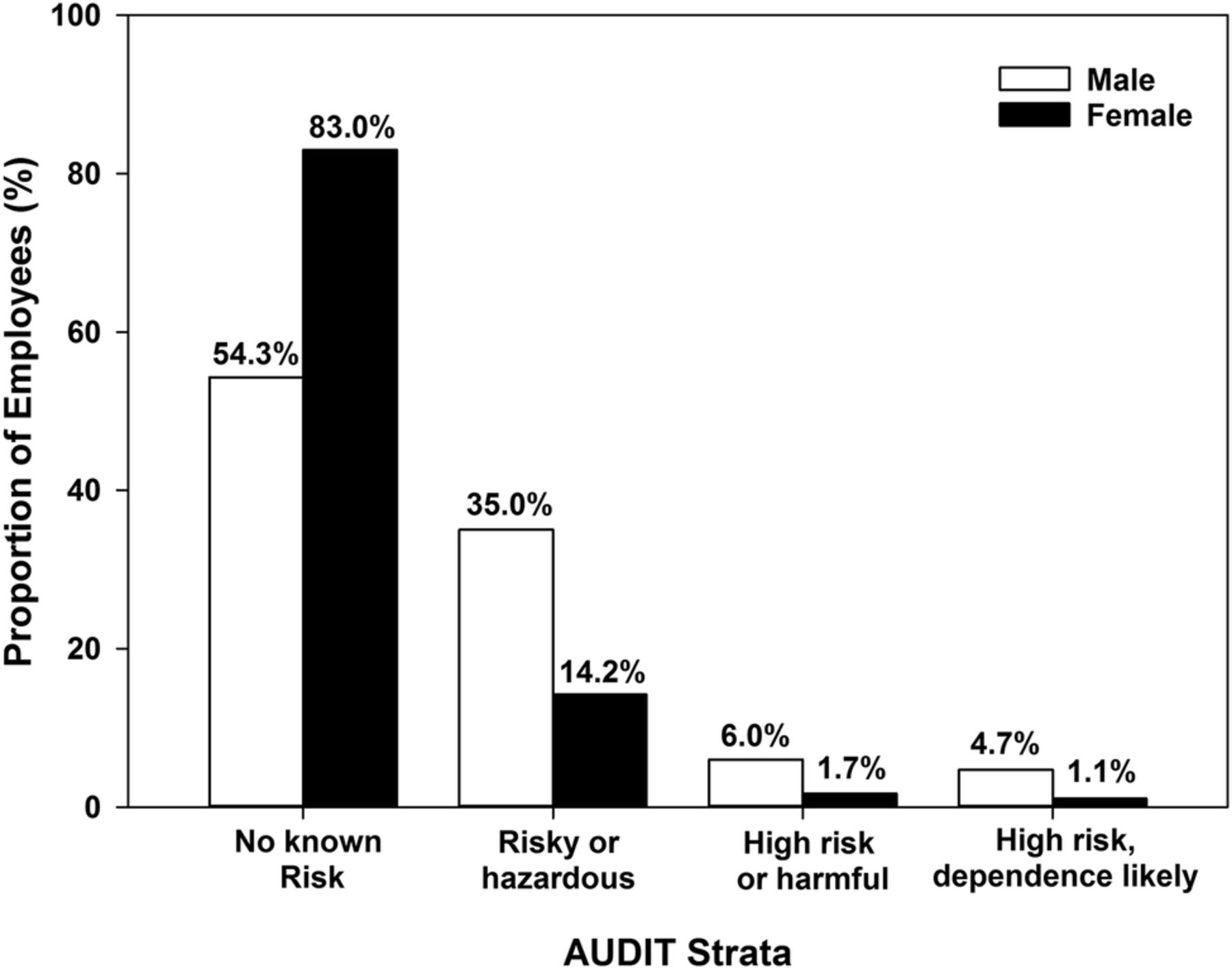
Almost half (45.7%) of the males and 17.0% of the females scored above the threshold for risky or hazardous alcohol use (AUDIT total ≥8; figure 1). The association between gender and alcohol use was significant χ2(3)=52.09, p<0.001.
{kind=link}
The prevalence of alcohol use within the risky or hazardous range by gender. AUDIT, Alcohol Use Disorders Identification Test.
Single-occasion drinking
There was a significant association between gender and single-occasion drinking χ2(4)=83.70, p<0.001. A greater proportion of male participants reported single-occasion drinking (88.3% vs 67.6%), and were also more likely to report single-occasion drinking more frequently, with 55.9% of males reporting single-occasion drinking at least once a month (including 28.5% weekly or more often) compared with 23.9% of female participants (including 9.1% weekly or more often) (table 3).
Characteristics associated with alcohol use
Sociodemographic factors
Significant bivariate associations were detected between the two outcomes ‘total AUDIT scores’ and ‘single-occasion drinking’, with participants' age, gender and highest level of education, with SNI scores associated with single-occasion drinking only (table 4).
Factors associated with participants’ total AUDIT and binge drinking scores—results from a four-step hierarchical linear regression analysis; n=(1410)
Within the multivariate analysis, sociodemographics accounted for 6.7% of the variance in total AUDIT scores and 7.6% of the variance in single-occasion drinking, with age and gender independently associated with both outcome variables. Single-occasion drinking and hazardous or harmful alcohol consumption were significantly associated with younger age and male gender.
Health history
Individual health history accounted for an additional 3.8% of the variance in total AUDIT scores and 0.7% of the variance in single-occasion drinking. Previous diagnosis of a drug and/or alcohol problem had a significant independent association with total AUDIT scores, but not single-occasion drinking, indicating that those who had previously been diagnosed with a drug and/or alcohol problem were significantly more likely to report hazardous or harmful drinking, but not current single-occasion drinking.
Current health
Significant bivariate associations were detected between the two outcome variables and the participants’ self-reported illicit drug use and smoking status, with a significant bivariate association between psychological distress and total AUDIT scores only (table 4).
Within the multivariate analysis (see table 4), current health characteristics made a unique contribution of 10.7% of the variance on total AUDIT scores, and 7.3% of the variance in single-occasion drinking scores. There was a significant positive association between outcome variables and current smoking status, and self-reported cannabis usage, indicating that those who smoked tobacco or used cannabis were significantly more likely to report hazardous or harmful alcohol use and single-occasion drinking. Other illicit drug use and current psychological distress had a significant positive association with total AUDIT scores, but had no significant association with single-occasion drinking.
Workplace factors and attitudes
Workplace factors including the type of mine and the employee type, as well as attitudes towards working in the industry, including the perception of control and demands and the primary reasons for working in the industry, had a significant bivariate association with both outcome variables (see table 4).
However, the multivariate analysis (see table 4) detected only a modest contribution by workplace factors and attitudes to the model, accounting for an additional 2.9% of the total variance in total AUDIT scores, and 2.5% of the variance in single-occasion drinking. Underground miners reported significantly higher total AUDIT and single-occasion drinking scores than those who worked in open-cut mining. The perceptions and experience at work were also important, with those who worked in mining primarily for financial reasons having significantly higher scores across both outcome variables.
For readers more familiar with using the AUDIT as a binary indicator of hazardous alcohol risk (ie, AUDIT=8 or above), we conducted a parallel hierarchical logistic regression analysis including only the nine significant variables in table 4 (see online supplementary table S1). All of these variables were significant, with the exception of ‘other illicit drugs’ and mine type. As an illustration, the variables with the highest and lowest significant standardised regression weights in the continuous analysis had these relative risk ratios in the logistic analysis: male versus female (45.7% vs 17.0%; OR=0.23, p<0.001); endorsement of working in mining for financial reasons low versus high (31.1% vs 50.6%; OR=1.82, p<0.001).
supplementary table
Adjusted odds ratio of factors significantly associated with total AUDIT scores – results from a four-step hierarchical logistic regression analysis; n=(1,410).
Recruitment method
Differences between recruitment methods were investigated using the same hierarchical regression model, with the exception of type of mining, which was moved to the first level given significant differences in the composition of the workforce for open-cut and underground mines. After controlling for type of mine, significant differences observed according to recruitment method indicated that participants from training days were less likely to have a degree (10.7% vs 19.9%) or to be concerned about losing their job (13.0% vs 24.2%); however, neither of these variables were associated with alcohol use (see table 4).
Discussion
This study is the first to report on the factors associated with alcohol-related problems among coal mine employees in Australia. The findings indicate that 45.7% of males and 17.0% of females reported levels of alcohol within the range considered as risky or hazardous. For females, this is closely aligned with available national community data.23 For males, the number within the at-risk range was almost double gender matched data previously reported on an Australian community sample (24%).23 While specific mining industry comparisons are limited, one study involving mining employees from a single mine in central QLD, Australia, published nearly two decades ago, found that 37% of males reported hazardous or harmful alcohol use (no female data were reported),11 considerably less than that found in this study. The results were, however, largely consistent with a more recent study involving employees from a single gold mine in Western Australia, which, using the AUDIT, showed that the proportion of harmful drinking was similar to that observed in this study (44.9% males and 23.9% females).24
To assess short-term risky alcohol consumption, we also measured the frequency of single-occasion drinking, defined as consuming six or more drinks on one occasion. Most participants had engaged in single-occasion drinking at least once in the preceding 12 months, with males (88.3%) more likely than females (67.6%). Single-occasion drinking has been associated with a number of serious health consequences,25 and can have a profound impact on workplace productivity.26 While this is a contentious area of research4 there is some evidence to show that following a night of excessive alcohol use, performance in tasks involving repetition, reaction time and decision-making may be significantly impaired.27 The high proportion of employees who reported single-occasion drinking in this study provides further support that the industry may benefit from implementing health promotion programmes which include a focus on alcohol use outside of the workplace.
The study was based on a conceptual model that integrated workplace characteristics, work–family–community interface and personal characteristics,15 using an analytic strategy that explored the independent effect of work characteristics and modifiable work environment factors. This incorporated key elements of the workplace PSC framework that provides a model for the workplace pathways to employee psychosocial outcomes.16 The findings demonstrated that there is a complex interplay between personal, social, workplace and employment factors contributing to alcohol use. Consistent with previous research,28 individual-level factors were most strongly associated with problematic alcohol use, with those who reported risky or hazardous alcohol use significantly more likely to be male, younger in age, have a history of drug and/or alcohol problems, be a current daily smoker, report higher psychological distress and report current or previous usage of illicit substances.
The link between problematic alcohol use and psychological distress is a key finding in this study, with those who reported higher alcohol use significantly more likely to report higher psychological distress. Interestingly, psychological distress was significantly associated with total AUDIT scores, but not single-occasion drinking. This discrepancy may reflect the properties of the AUDIT tool, which, in addition to measuring frequency and quantity of consumption, also assess the social and behavioural consequences of alcohol use, which might be more closely associated with psychological distress. It is unknown whether the problematic use of alcohol preceded psychological distress, or that the participants consumed alcohol to relieve tension in response to stress, as has been reported previously.29 Nevertheless, the linkage between problematic alcohol use and mental ill health is well established, with many national and international studies reporting the interaction.29–32 Given that self-reported alcohol and tobacco use, as well as psychological distress, are high in this sample, an integrated response to mental health, tobacco and alcohol use in this industry is warranted.
This study also identified a link between the primary method of mining and alcohol use, with higher rates of harmful use among those who work in underground mining, possibly reflecting differences in the workplace culture. It has previously been suggested that some workplace cultures may exert formal or informal pressure to encourage team bonding and relaxation both outside and within the workplace that revolve around alcohol use.2 These can develop as drinking subcultures where drinking alcohol is considered appropriate and expected,33 and may include consumption of alcohol outside of work hours that are influenced by workplace social norms.34 Previous studies have indicated that workplace cultures and norms of risky drinking may explain differences between workplaces.35
Personal financial factors were linked with alcohol use in our findings. This relationship between consumption of alcohol and financial pressure has been consistently reported in the literature.36 Interestingly, those working in mining in Australia report salaries nearly double the national average.37 A possible explanation specific to this high-income industry is a concept referred to as ‘golden handcuffs’ and job insecurity, particularly in an industry subject to patterns of ‘boom and bust’.38 This refers to individuals who enter the industry attracted by lucrative remuneration packages, and their lifestyles adapt and become dependent on high salaries. This may present a somewhat unique stressor, whereby employees are required to continue working in the industry to sustain their lifestyle despite the impact on other aspects of their life, with limited opportunities in other industries that offer equivalent salaries, and may use alcohol to alleviate this stress.
Current self-reported illicit drug use was low in this study, with cannabis the most commonly reported substance used within the past month at 2.3%. It has been suggested that one of the limitations of workplace drug testing is that it may encourage employees to modify their drug-taking behaviour to avoid detection, by substituting drugs that have a long window of detection (eg, cannabis) with drugs that have a shorter window of detection (eg, methamphetamines).39 Despite this evidence, the proportion of participants who self-reported current illicit drug use was low.
Limitations
First, the current research was cross-sectional, which does not allow temporal sequence to be determined, and therefore the results may not reflect causal associations. For example, the range of current health characteristics that were assessed may be contributing to alcohol use, could be a consequence of alcohol consumption or may simply co-occur. Nevertheless, these sets of behaviours are highly modifiable and as a group may represent a useful target for preventative intervention in the workplace.
Second, one of the major limitations of any research involving the usage of self-report data is possible social desirability bias. Given that usage of illicit substances, and alcohol at hazardous levels is a sensitive social issue, it is possible that participants may have been unwilling to disclose their true substance use behaviours. This may be exacerbated by strict workplace restrictions on alcohol and, further, by the current significant downturn in the mining industry. While it is possible that the downturn may have motivated participants to under-report substance use, it is equally possible that the downturn was associated with an increase in alcohol use, as has been previously shown in those who maintain employment during periods of recession.40 Given the high proportion of participants who scored within the ‘at-risk’ categories for hazardous alcohol use in this study, it is less likely that participants' responses were influenced by a social desirability bias. The low self-reported illicit drug use may potentially reflect under-reporting of actual current use, or may equally reflect an actual low use of illicit substances in an effort to avoid possible drug detection at work.
A third limitation was the recruitment protocol. While there was considerable variation in the response rate dependent on the data collection method, we observed no statistical differences in AUDIT scores between the two recruitment methods. Furthermore, all factors significantly associated with recruitment were not associated with alcohol use. In further support of the representativeness of the sample, we found a strong correlation between the age, gender and employment category profile for each of the mines that participated in the study with state based employment data. This suggests that although the response rate was lower at some mines, the sample still contained a representative cross-section of all employees at the site.
Conclusion
The coal mining industry has invested considerable resources to minimise the use of alcohol and its immediate impact on safety, with the use of regular breath testing a common element of alcohol policy at many mine sites.10 The significant levels of alcohol-related problems identified in this study occur in the context of compulsory alcohol testing before work begins, and random testing for illicit substances. While alcohol testing may address the immediate risk of impairment due to alcohol use while at work, they neglect the impact of drinking outside of work on the physical and mental health of employees. Frequent and high quantities of alcohol consumption are likely to impact on other areas of workplace health and safety including fatigue, mood and cognitive ability.41 Important for the industry will be broadening its approach to address alcohol consumption as part of the overall commitment to occupational health and safety of employees. While factors involving workplace culture or behaviours outside of work were not specifically assessed in this study, they are important for future research.
Our findings can provide some guidance to address alcohol and its impact on health, safety and productivity in the industry. These results indicate that a high proportion of male miners consume alcohol at a risky or hazardous level, which suggests that the industry may benefit from implementation of programmes to address alcohol use beyond those that focus on detection of alcohol levels or intoxication in the workplace. This is encompassed within the industry's national framework within the Blueprint for Mental Health in the Mining Industry17 that identifies targets for workplace mental health programmes. While the coal mining industry has made substantial gains in implementing policy regarding on-site alcohol monitoring (eg, mandatory breath testing), the workplace can shape attitudes to alcohol use more broadly through workplace health promotion, and tailored intervention programmes through the employee assistance programme, which may bring financial and social benefits through impacts on employee health and performance.
Acknowledgments
The Newcastle Institute of Energy and Resources through the support of Dr Alan Broadfoot, and Gerry Bobsien, through their extensive collaboration with resource industry partners, was fundamental in ensuring engagement between the research team and the coal mining industry. The investigator team would also like to acknowledge the support of a number of health professionals who provided assistance at various stages of the project including Trevor Hazell, Prasuna Reddy, Katie McGill, Jennifer Robinson and Genelle Sharrock. The team would also like to acknowledge the support of industry representatives who provided guidance and support for the research including Shane Apps, Judy Bertram, Shane Hansford, Andrew McMahon, Liam Wilson and Simon Worland. Professor Brian Kelly is the Aspen Medical Chair of the Centre for Resources Health and Safety, University of Newcastle. The centre was established in partnership with Aspen Medical, a leading provider of healthcare solutions in the Mining and Resources sector.
References
Footnotes
Contributors RJT is the main author and contributed to all aspects of study design, data acquisition, data analysis and interpretation, and preparation of the manuscript. RC and BJK led the study conception and design, with RC involved in data collection. TJL and JW provided assistance with study design, data collation, analysis and interpretation. FK-L, ALB, JS, DP, KI and CJ provided strategic guidance throughout the project, and assisted with preparation of the manuscript.
Funding Australian Coal Association Research Program (ACARP), grant number c22045.
Competing interests None declared.
Ethics approval University of Newcastle Human Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.