Article Text

Abstract
Occupational exposure is an important risk factor for chronic obstructive pulmonary disease (COPD), and silica dust is one of the most important occupational respiratory toxins. Epidemiological and pathological studies suggest that silica dust exposure can lead to COPD, even in the absence of radiological signs of silicosis, and that the association between cumulative silica dust exposure and airflow obstruction is independent of silicosis. Recent clinicopathological and experimental studies have contributed further towards explaining the potential mechanism through which silica can cause pathological changes that may lead to the development of COPD. In this paper we review the epidemiological and pathological evidence relevant to the development of COPD in silica dust exposed workers within the context of recent findings. The evidence surveyed suggests that chronic levels of silica dust that do not cause disabling silicosis may cause the development of chronic bronchitis, emphysema, and/or small airways disease that can lead to airflow obstruction, even in the absence of radiological silicosis.
- crystalline silica dust
- chronic obstructive pulmonary disease
- airflow obstruction
- emphysema
- chronic bronchitis
- small airways disease
- α1-AT
- α1 protease inhibitor
- BHR, bronchial hyperresponsiveness
- COPD, chronic obstructive pulmonary disease
- CT, computed tomography
- DLCO, carbon monoxide diffusion in the lung
- ES, emphysema score
- FEF, forced expiratory flow
- FEV1, forced expiratory volume in one second
- FVC, forced vital capacity
- MDAD, mineral dust airways disease
- MMEF, maximal mid-expiratory flow
- NMRD, non-malignant respiratory disease
- TB, tuberculosis
- VC, vital capacity
Statistics from Altmetric.com
- crystalline silica dust
- chronic obstructive pulmonary disease
- airflow obstruction
- emphysema
- chronic bronchitis
- small airways disease
- α1-AT
- α1 protease inhibitor
- BHR, bronchial hyperresponsiveness
- COPD, chronic obstructive pulmonary disease
- CT, computed tomography
- DLCO, carbon monoxide diffusion in the lung
- ES, emphysema score
- FEF, forced expiratory flow
- FEV1, forced expiratory volume in one second
- FVC, forced vital capacity
- MDAD, mineral dust airways disease
- MMEF, maximal mid-expiratory flow
- NMRD, non-malignant respiratory disease
- TB, tuberculosis
- VC, vital capacity
Occupational exposure to crystalline silica (silica) dust occurs in many industrial operations worldwide.1 The reduction of silica dust exposure levels in most developed countries during the last century resulted in dramatic decreases in morbidity and mortality from silicosis and silica dust associated tuberculosis (TB). Despite this, chronic obstructive pulmonary disease (COPD) remains a health issue in workers exposed to silica dust.1–8
Epidemiological studies show that silica dust exposure can lead to airflow obstruction in the absence of radiological signs of silicosis,4–8 and that the association between cumulative silica dust exposure and airflow obstruction can be independent of silicosis.9,10 It is therefore likely that certain properties of silica dust are capable of causing COPD that may precede, or be independent of, silicosis development. Recent clinicopathological and experimental studies help to explain the potential for silica dust to cause pathological changes that may lead to the development of COPD.
The purpose of the present paper is to review the epidemiological and pathological evidence on the association between COPD and silica dust exposure in the light of recent clinical and experimental findings. The aim is to address the unresolved issue of whether silica dust can cause pathological changes in the lungs leading to the development of COPD at exposure levels that may not cause silicosis. The review will briefly define COPD, outline the potential pathological mechanisms by which silica dust can cause COPD, and present the evidence for airflow obstruction and the pathological changes.
DEFINITION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
The American Thoracic Society (ATS) defines COPD as a “disease state characterised by the presence of airflow obstruction due to chronic bronchitis or emphysema”.11 The European Respiratory Society (ERS) definition of COPD is based on progressive and irreversible reduction of maximum expiratory flow.12 In silica dust exposed workers, lung fibrosis and pulmonary tuberculosis can contribute to airflow obstruction. While it is not possible to quantify precisely the contribution of individual pathological changes to airflow obstruction in silica dust exposed workers, the review attempts to evaluate their relative importance.
POTENTIAL MECHANISMS OF SILICA PATHOGENICITY IN THE LUNGS—AN OUTLINE
The current thinking is that chronic inflammation and remodelling of small airways (bronchitis) and destruction of lung parenchyma (emphysema), in response to inhalant oxidants generated by smoking and other environmental exposures, leads to COPD.13,14 The predominant inflammatory cells involved in the airways remodelling and parenchymal destruction characteristic of COPD are neutrophils, macrophages, and T lymphocytes (CD8+ and CD4+).15 There are several potential mechanisms by which silica particles can initiate cell injury leading to COPD. These include cytotoxicity,16,17 leading to generation of reactive oxygen/nitrogen species,18,19 and secretion of proinflammatory factors, cytokines, chemokines, elastase,20–23 and fibrogenic factors.24,25 Potentially these mechanisms can initiate changes in lung tissue leading to airflow obstruction as follows: (a) silica particles can initiate toxic and inflammatory processes in conducting and peripheral airways, and alveolar tissue characterised by release of mediators leading to increased production of oxidants, cytokines, chemokines, and elastase, inducing airways inflammation16,17 and emphysema20–23; or (b) silica particles can cause epithelial cell injury that facilitates penetration of the silica particles through the walls of small airways and causes localised fibrosis.24,25 Restrictive disease has been associated with a production of collagen and fibroblast growth factors, leading to fibrosis in the alveolar walls,26 and formation of silicotic nodules.27,28 Depending on the exposure pattern and individual susceptibility there can be pathological states with opposing effects on pulmonary function: chronic bronchitis, bronchiolitis, and emphysema, which cause airflow obstruction; and fibrosis, which causes primarily restrictive changes.
EPIDEMIOLOGICAL EVIDENCE FOR EXPOSURE-RESPONSE RELATION FOR AIRFLOW OBSTRUCTION
The epidemiological studies of the exposure-response relation between silica dust exposure and airflow obstruction have been divided into those where radiological signs of silicosis were present, and those where radiological signs of silicosis were absent (table 1).
A summary of studies which estimated lung function loss associated with average cumulative dust exposure or average duration of exposure*
Studies where radiological silicosis was present
A study of white South African gold miners showed that the forced expiratory volume in one second (FEV1), and the FEV1/FVC ratio, adjusted for age, height, and tobacco smoking, decreased with increasing cumulative respirable dust exposure, in both smokers and non-smokers.29,30 The average cumulative dust exposure attributable loss in lung function, estimated for a 50 year old miner exposed for 24 years to an average respirable dust concentration of 0.6 mg/m3 was 236 ml of FEV1 (95% CI 135 to 338), 217 ml of FVC (95%CI 110 to 324), and 2.3% of FEV1/FVC (95% CI 0.8 to 3.8).30 This is equivalent to an average excess loss of 9.8 ml/y of FEV1 and 9.0 ml/y of FVC over 24 years of mining. In this study silicosis was not associated with significant loss of FEV1 or FVC.9,30 In a follow up study five years later similar estimates for lung function losses were found.30
To provide perspective on the above estimates, these were related to prediction curves for lung function decline with age for the general population of white males 31 (fig 1). The results show that regardless of smoking habits, young white South African gold miners (fig 1, curve D30,32) on average had better lung function than the general population. However, older miners (smokers and non-smokers) had a steeper decline in FEV1 with age than the general population.

Predicted values for gold miners, according to levels of dust exposure and smoking habits, projected onto predicted curves for general white male population. A, non-smokers; B, current smokers of one pack a day; C, current smokers of two packs a day. The D curve shows the mean observed FEV1 values for 20 and 30 year old white South African miners, smokers and non-smokers, joined with values for the 50 and 55 year old miners. Adapted from Hnizdo and colleagues.30
Similar losses in lung function were also observed among black South African gold miners,33 Canadian hard rock miners,34 and US molybdenum miners35 (table 1).
Studies where radiological silicosis was absent
In a 12 year follow up study, Swedish granite crushers exposed to mean cumulative respirable silica dust of 7.2 mg/m3-y had a greater loss of FEV1 by 150 ml (4.6%) and of FEV1/FVC % by 3.2 (5.4%) when compared to age and smoking matched unexposed controls.36 The functional changes were consistent with airflow obstruction in the granite crushers. In a cross sectional study of 45 380 Norwegian men of 30–46 years of age, 3445 had occupational exposure to silica dust.4 Workers with 15 or more years of silica dust exposure had a statistically significant excess loss of FEV1 of 4.3 ml/y (95% CI 1.1 to 7.5) over the years of exposure.4 In comparison, the loss due to smoking 20 cigarettes/day was estimated as 6.9 ml/y. The exposure-response trend for FEV1 and duration of silica dust exposure was similar among non-smokers, ex-smokers, and smokers. The loss in FEV1/FVC (but not in FVC), was also statistically significant among those with 15 or more years of exposure. Corroborative reports on silica dust associated airflow obstruction are from studies of 144 concrete workers,5 172 potato sorters exposed to diatomaceous earth,6 389 French pottery workers,7 and Chinese silica exposed workers.8
In summary, the epidemiological studies show an exposure-response relation between airflow obstruction (loss of FEV1 and FEV1/FVC) and cumulative silica dust exposure in smokers as well as in non-smokers. The relation was observed in groups of relatively young silica dust exposed workers who did not have radiological signs of silicosis, and at average exposure levels between 0.2 to 0.1 mg/m3 of respirable silica (table 1). The variability between studies in the estimated excess loss may be due to differences in sample size, exposure levels, dust toxicity,37,38 and the prevalence of silicosis.
COMBINED EFFECT OF SILICA DUST EXPOSURE AND SMOKING ON AIRFLOW OBSTRUCTION
Several studies have shown that smoking can potentiate the effect of silica dust. Studies of Canadian and US hard rock miners found that the effect of silica dust on lung function pattern is different in smokers compared to non-smokers.34,35 In non-smokers, the observed decreases in residual lung capacity measurements were suggestive of a restrictive impairment.35 On the other hand, smokers had significantly reduced FEV1, FEV1/FVC, FVC, and maximal expiratory flow rates, and increased residual lung capacity measurements—a pattern suggestive of emphysema. These changes increased with increasing dust levels, suggesting that smoking potentiates the association between silica dust and emphysema-like functional changes.35
A study of South African gold miners estimated the fraction of cases with severe airflow obstruction attributable to dust only, smoking only, and the combined effect of the two exposures (that is, the attributable fractions), and the fraction of cases that could be prevented by removal from each exposure (that is, the preventable fractions).39 The attributable fractions for severe airflow obstruction (found in 20% of miners) were estimated as 8% for dust alone, 42% for smoking, 40% for the combined effect of silica dust and smoking, and 10% for unknown factors. Estimated preventable fractions show that elimination of silica dust exposure would prevent 48%, and elimination of smoking 82% of severe airflow obstruction.39
In summary, the evidence shows that smoking potentiates the effect of silica dust exposure on airflow obstruction. Thus, eliminating or decreasing both dust and smoking is important in preventing silica dust associated COPD. The magnitudes of attributable and preventable fractions, however, are population specific and depend on the prevalence and intensity of exposure.
MORTALITY FROM CHRONIC OBSTRUCTIVE LUNG DISEASE
Numerous mortality studies of cohorts of silica dust exposed workers report increased mortality from non-malignant respiratory disease (NMRD).40–43 Generally, NMRD combines deaths from pneumoconioses and COPD. In mortality studies of South African gold miners, deaths from pneumoconiosis (ICD9, 500–505) and COPD (ICD9, 416, 490–492, 496) were coded separately, based on death certificate and postmortem examination findings for pneumoconioses, emphysema, and airways disease.42 In a recent study, of total 2032 deaths, 138 were from COPD (SMR 161, 95% CI 135 to 190), and 16 were from pneumoconioses.42 The studies found increasing exposure-response trend for COPD mortality and cumulative dust exposure that was modified by tobacco smoking.44 The attributable fractions for COPD mortality were estimated as 5% for dust alone, 34% for smoking, 59% for the combined effect of silica dust and smoking, and 2% for unknown factors.44 In the absence of silica dust exposure, 64% of COPD deaths could be prevented, whereas in the absence of smoking, 93% of COPD deaths could be prevented.44
In summary, deaths from COPD likely constitute a large proportion of deaths from NMRD in silica dust exposed workers. Silica dust exposure increases mortality from COPD and the effect is modified by tobacco smoking.
CAUSE OF AIRFLOW OBSTRUCTION IN SILICA DUST EXPOSED WORKERS
Epidemiological and clinicopathological studies investigated whether silicosis or other silica dust associated pathological changes cause airflow obstruction in silica dust exposed workers. Two case-control studies compared lung function in South African gold miners with and without radiological signs of silicosis, who were matched for cumulative dust exposure, tobacco consumption, and age. No significant differences were found between silicotic and non-silicotic miners in spirometry,9,10 plethysmography, blood gas analysis, and exercise tests—except for the slope of phase III. The slope of phase III was significantly elevated with a corresponding increase in closing volume in silicotic miners, suggesting impairment in the ventilation of alveolar units.10 Thus after matching on cumulative silica dust exposure and smoking, radiological signs of silicosis were not associated with significant airflow obstruction. These results support the hypothesis that the effect of cumulative silica dust exposure on airflow obstruction seen in the cohort of South African gold miners29,30 is independent of silicosis.
However, undetected silicotic nodules in the lungs may potentially explain airflow obstruction in silica exposed workers without radiological signs of silicosis. This issue was addressed by clinicopathological studies that correlated computed tomography (CT) findings for silicosis and emphysema with pulmonary function in silica exposed workers. In these studies, CT scan grades for silicosis and emphysema were found to correlate with standard radiographic45,46 and pathological scores,47 respectively, but the CT scan was found to be more sensitive in detecting confluent silicosis.48 Among 17 silicotic subjects, poor correlations were found between spirometry and profusion of nodules on the chest radiograph and CT scan, while there was a significant correlation between CT emphysema score and decreasing FEV1 and DLCO.49 In a study of 30 silicotics, the emphysema score rather than the degree of silicosis was associated with decreased FEV1 and FVC; however, decrease in DLCO was associated with severe silicosis with PMF.50 In non-smokers with progressive massive fibrosis (PMF), emphysema was present even in non-fibrotic areas of the lung. A study of 111 silica exposed workers evaluated the prevalence and severity of emphysema according to smoking status and severity of silicosis.45 There was no emphysema and no airflow abnormalities in non-smokers without silicosis (n = 7), whereas all non-smoking silicotics (n = 6) had emphysema affecting on average 25% of the lung. In smokers, the prevalence and severity of emphysema increased with severity of silicosis. Emphysema and associated airflow obstruction were especially prevalent in confluent silicosis (that was often not detectable radiologically). These authors concluded that in simple radiographic silicosis, emphysema, rather than silicosis, is associated with reduced FEV1/FVC ratio, and maximal mid-expiratory flow (MMEF) and DLCO.48 The study also found that silica dust exposure was associated with more emphysema than asbestos dust.48 In a study of 70 black South African gold miners, CT scan scores for silicosis of 0, 1, 2, and 3 were associated with mean emphysema CT scores of 14%, 46%, 48%, and 67%, respectively.51 Emphysema, rather than silicosis, was reported to be associated with reduction of FEV1/FVC and MMEF. In Chinese silica dust exposed workers, radiological signs of hyperinflation were associated with significant airflow obstruction and increasing grades of silicosis.52
In summary, the above studies show that emphysema, rather than silicosis, correlates with airflow obstruction observed among silica dust exposed workers, including subjects with silicosis. The CT scan studies were small, however, and did not consider the effect of cumulative dust exposure.
EXTENT OF EMPHYSEMA DUE TO SILICA DUST EXPOSURE AND ASSOCIATED AIRFLOW OBSTRUCTION
Three epidemiological studies of South African gold miners investigated the exposure-response relation between silica dust exposure and emphysema found at autopsy.53–55 A standardised assessment of emphysema was done on paper mounted whole lung sections and the resulting emphysema score (ES) represents the percentage of the lung affected by emphysema. These studies estimated that working for 20 years in jobs with high silica dust exposure increases risk of emphysema (ES >30) between 3.5 times (95% CI 1.6 and 6.6)54,55 and 12.7 times (95% CI 3 to 52)53 in comparison to those with low dust exposure.
The amount of emphysema attributable to smoking and silica dust was estimated by a study of 1553 postmortem examinations.55 The mean ES, adjusted for the effect of dust, silicosis, and age, was 7.1 for non-smokers and 36.5 for smokers of 20+ cigarettes/day—that is, an increase of nearly 30 ES units attributable to smoking. In comparison, the adjusted mean ES was 24.4 for the lowest dust exposed group and 29.3 for the highest dust exposed group—that is, an increase of 4.9 ES units attributable to high dust exposure. In addition, the dust adjusted increase associated with marked silicosis was 4.8 ES units. Thus, the amount of emphysema attributable to the combined effects of high dust exposure and marked silicosis was approximately 10 ES units. These results are supported by a study of 242 lifelong never smoking gold miners of an average age at death of 65.9 and ∼23 years of mining, where the median ES at autopsy was 5 (fig 2).56 Thirty per cent of the workers had ES of 0, 55% had ES between 1 and 20, and 15% had ES above 20.
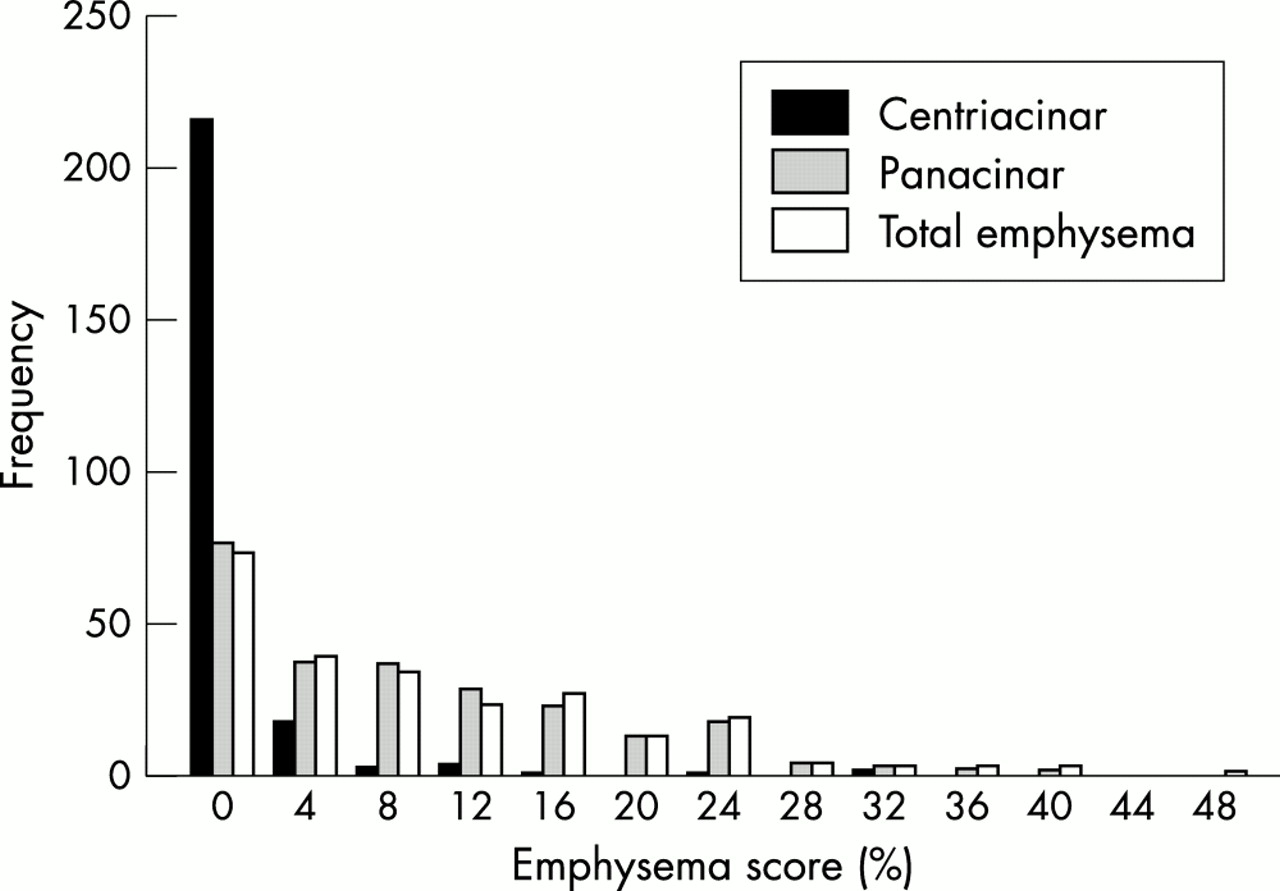
Frequency distribution for the centriacinar, panacinar, and total emphysema scores found in non-smokers with long duration of silica dust exposure. From Hnizdo and colleagues.56
Relating the attributable emphysema scores to estimated loss of lung function observed in life further illustrates the relative contribution of smoking and silica dust. Figure 3 shows the relation between mean percentage predicted FEV1 observed five years prior to death and the mean emphysema score found at autopsy among 726 South African gold miners.57 FEV1 % predicted is categorised into impairment categories used for workers’ compensation. As illustrated in fig 3, ES of 30 units attributed to smoking can cause moderate to severe airways obstruction. Adding 10 ES units attributable to the combined effects of high dust and silicosis would make the obstruction more severe. On the other hand, without the effect of smoking, the effect of silica dust exposure and silicosis—that is, ∼10 ES units, would result mainly in mild obstruction. Figure 3 also shows that even a small increase in the average ES score caused by silica dust alone can result in measurable lung function loss. Thus the cut off point of 30 ES used in the above exposure-response studies53–55 may have led to an under estimation of the association between silica dust exposure and emphysema.

{kind=link}
{kind=link}
{kind=link}
Observed (*) and estimated mean FEV1 % predicted and 85% mean CI in relation to emphysema score found within five years at postmortem examination in 726 South African gold miners. In-life compensation categories (normal, mild, moderate, severe) are indicated. From Hnizdo and colleagues.57
The importance of emphysema, mucus gland hyperplasia, and silicosis found at postmortem examination to airflow obstruction observed five years prior to death was also investigated in a clinicopathological study of 724 South African gold miners with a mean age of 64 years and ∼24 years of mining.57 In this study the emphysema score was the most important explanatory variable for loss of FEV1 observed in life. Emphysema was associated mainly with reported symptoms of dyspnoea, rather than cough and phlegm, during life.
In summary, postmortem examination studies show an association between silica dust exposure, silicosis, and emphysema. The amount of emphysema found among never-smokers with long silica dust exposure can lead to mild to moderate airflow obstruction. The postmortem examination findings are consistent with the CT scan studies that among silica dust exposed workers emphysema correlates better with airflow obstruction than silicosis.
MECHANISMS BY WHICH SILICA DUST CAN INDUCE EMPHYSEMA
The mechanism by which silica can produce emphysema is not well understood.22 Current evidence suggests that the mechanism is similar to that of cigarette smoke—that is, the destruction of α1 protease inhibitor (α1-AT) by oxidants generated by inflammatory cells as well as silica dust.22 Emphysema induced by cigarette smoke is initiated by the oxidants in cigarette smoke causing a protease-antiprotease inbalance and decreased anti-elastase activity.58 It is postulated that silica may induce emphysema by the release of proteolytic enzymes from dust evoked inflammatory cells and by oxidative inactivation of α1-AT by the excessive oxygen free radicals generated by silica particles and inflammatory cells.20–23 This hypothesis is supported by a recent animal study of markers of connective tissue breakdown (desmosine, hydroxyproline) in response to silica instillation and their correlation with an increase of neutrophil driven protease.23 Experimental studies on rats show that intratracheal instillation of quartz in increasing doses can cause emphysema and thickened airways walls, leading to significantly reduced lung function.59 Changes compatible with emphysema were observed at lower doses of quartz than small airways fibrosis and early silicotic nodules.59 This is consistent with the high potential of silica compared to coal to cause cytotoxicity, and release of proinflammatory mediators, cytokines, and reactive species at a sustained level by the repeated frustrated phagocytosis of silica.16,18 Acute inflammatory reactions elicited by silica can lead to an increased α1-AT breakdown and decreased anti-elastase activity, providing support to epidemiological and pathological observations.
In summary, experimental studies show that silica can cause elastic tissue destruction by inactivation of α1-AT, which could lead to emphysema in the absence of fibrosis by a pathological mechanism similar to smoking induced emphysema.
EFFECT OF SILICA ON AIRWAYS DISEASE
Chronic bronchitis
Epidemiological studies show that the prevalence of chronic bronchitis (chronic productive cough) increases with intensity and duration of silica exposure.29,33,35,60,61 A clinicopathological study of COPD among South African gold miners found that in the absence of emphysema, a marked degree of mucus glands hyperplasia is associated with little airflow obstruction.57 Furthermore, marked mucus glands hyperplasia was associated mainly with rhonchi, sputum production, and cough during life, but less with symptoms of breathlessness which were associated strongly with emphysema.57 In addition, chronic bronchitis in the absence of airflow obstruction was not associated with increased mortality from COPD in these miners.62
Current evidence on COPD pathology indicates that mucus derived from mucus secreting submucosal glands and goblet cells in conducting airways is associated with symptoms of chronic bronchitis—that is, cough and sputum.13,14 However, inflammation and structural alterations occurring in peripheral airways and lung parenchyma are considered the most important contributors of airflow obstruction in COPD.14,15,63,64 Infiltration of T lymphocytes and macrophages in the subepithelial wall have also been implicated in the characteristic changes in conducting airways.15,65
In summary, silica dust exposure increases the risk of chronic bronchitis. The evidence suggests that mucus gland hyperplasia in conducting airways without emphysema and/or small airways disease is unlikely to cause a significant airflow obstruction.
Mineral dust airways disease
Experimental and clinical studies show that mineral dusts, including silica, can cause small lesions in all types of small airways, but affecting mostly the walls of membranous and respiratory bronchioles and alveolar ducts.66 These lesions consist of deposits of fibrous tissue, often accompanied by pigment, and variably accompanied by inflammatory infiltrates. Respiratory bronchioles appear to get affected before the alveolar ducts. This condition, defined as mineral dust airways disease (MDAD), is morphologically distinguishable from the small airway disease produced by tobacco smoke.66,67
In a clinicopathological study, MDAD was found in 25% (13 of 53) of workers with previous occupational mineral dust exposure, and in 0.8% (one of 121) of those without such exposure.67 In dust exposed subjects, those with MDAD had significantly decreased FEV1, FEF25–75, VC, and DLCO, and increased residual capacity when compared to those without MDAD matched on smoking and age. Not all subjects exposed to mineral dust show MDAD, but in affected subjects MDAD is widespread, affecting 70% of the respiratory and 40–70% of the membranous bronchioles.67 In contrast, micronodules (that is, fibrotic lesions in respiratory bronchioles) diagnosed by CT scan were not related to airways obstruction in 35 silica exposed workers.68 CT scan assessed emphysema, on the other hand, was associated with decreased lung function (FEV1, FEV/FVC, and DLCO) and the association was not affected by the presence of micronodules. A study of small airways obstruction in 153 granite quarry workers, by a computerised electronic digitiser of flow rates at low lung volumes, reported that obstruction was increased among silica dust exposed workers, even in the absence of radiological signs of silicosis and large airways obstruction.69
Silica particles are strongly fibrogenic and can penetrate airway epithelium, triggering generation of reactive oxygen species, proliferative and fibrogenic growth factors, and inflammatory mediators.23,24 It is generally assumed that inflammatory cells are the initiators of the fibrogenic response. However, airway wall fibrosis due to silica may occur in the absence of any increase in inflammatory cells in the airspace or circulation and may be independent of inflammation and emphysema.23
In summary, the evidence shows that silica dust exposure can cause widespread fibrotic lesions in small airways, affecting mostly the walls of membranous and respiratory bronchioles and to a lesser degree alveolar ducts. These changes may lead to airflow obstruction. The exposure-response relation for silica dust exposure and MDAD, and the associated airflow obstruction has not been well established.
THE ROLE OF ATOPY AND BRONCHIAL HYPERRESPONSIVNESS IN DEVELOPMENT OF COPD
Atopy and non-specific bronchial hyperresponsivness (BHR) have been identified as risk factors for COPD.70–72 It has been proposed that atopy and BHR can modify the effect of cigarette smoking on COPD.70–72 There is a question whether atopy and BHR modify the effect of silica on the development of COPD. In silica dust exposed South African gold miners, the presence of reactive airways was associated with reduced FVC, FEV1, and FEV1/FVC, but duration of silica dust exposure was not related to reactive airways.73 In addition, respiratory challenge with gold mine dust was not associated with a significant decrease in FEV1 or FVC, even in those who had COPD.74 In a study of 3445 Norwegian silica dust exposed workers, neither asthma (or wheezing), nor atopy were found to be significant modifiers of the effect of silica on spirometry.4 Similar results were found in a study of potato sorters exposed to diatomaceous earth.6
In summary, the evidence from cross sectional studies does not support the hypothesis that asthma, atopy, or BHR modify the effect of silica dust on lung function loss. Since selection bias due to healthy worker effect could account for these findings, a prospective study is required to establish this conclusively.
EFFECT OF PULMONARY TB ON AIRFLOW OBSTRUCTION
Silica dust exposed workers are at increased risk of developing TB,1 even in the absence of silicosis.75 Residual damage from treated TB is associated with airflow obstruction and restriction in the general population.76 In black South African gold miners, chronic lung function loss increased with the number of episodes of treated TB.77 The mean chronic deficits in FEV1 after one, two, and three episodes were 153 ml, 326 ml, and 410 ml, respectively, with a corresponding FVC deficit of 96 ml, 286 ml, and 345 ml.77 TB was found also to be an important predictor of airflow obstruction in former South African gold miners.78,79
CONCLUSION
It is well recognised that severe silicosis can cause significant lung function impairment.80,81 There are, however, questions as to whether silica dust can cause other pathological changes in the lungs leading to the development of COPD, and whether these changes precede development of silicosis and can occur at exposure levels that may not cause silicosis.
The evidence from epidemiological studies of workers exposed to average respirable silica dust concentrations ranging between 0.2 and 0.1 mg/m3 shows a significant exposure-response relation for cumulative dust exposure and airflow obstruction that is independent of radiological signs of silicosis. Exposure-response trend was observed, especially in younger populations, of silica dust exposed workers who did not have radiological signs of silicosis (table 1) and in mortality studies. Smoking potentiates the effect of silica dust on airflow obstruction and death from COPD.
Emphysema appears to be the predominant pathology associated with airflow obstruction in silica dust exposed workers. Postmortem examination studies found an exposure-response relation between cumulative silica dust exposure, silicosis, and emphysema. The amount of emphysema found in silica dust exposed never-smokers could be associated with mild to moderate obstruction in life. Emphysema usually coexists with inflammation in small airways and small airways disease is important in COPD.14 However, the exposure-response for small airways disease, and its role in airflow obstruction observed in silica dust exposed workers, is still not clear. In experimental studies, silica was shown to be capable of inducing inflammatory changes in epithelial cells that may potentially lead to small airway disease. A clinicopathological study shows that MDAD can be widespread and may lead to airflow obstruction. There is also evidence of increased prevalence of small airway obstruction among silica dust exposed workers.
It was shown that in rats exposed to silica dust, emphysema occurs at lower silica doses than does fibrosis in small airways or early silicotic nodules.59 This suggests that silica dust induced emphysema could precede MDAD and silicosis in humans. However, in high dust levels and severe silicosis, the restrictive pattern can make it difficult to detect airflow obstruction caused by emphysema that has been induced by silica dust.82 It is of interest therefore that most of the epidemiological studies that did not find radiological signs of silicosis, found statistically significant airflow obstruction (decreased FEV1/FVC ratio) with increasing silica dust exposure (table 1), even in relatively young workers.4 Apart from silica dust dose, variability in dust toxicity and contamination by other toxic particles83 may determine the amount and presence of the respiratory injury.
In summary, the evidence surveyed here suggests that chronic lower levels of silica exposure may lead to the development of emphysema, chronic bronchitis, and/or MDAD that can lead to airflow obstruction, even in the absence of radiological signs of silicosis.
Acknowledgments
The authors would like to thank Drs Robert Castellan, Vince Castranova, Mike Attfield, Paul Henneberger, and Patricia Sullivan for their critical editorial reviews and comments on the manuscript.