Article Text

Abstract
Objectives: To compare respiratory symptoms and upper airway inflammation in domestic waste collectors and controls, and to find the association between measures of upper airway inflammation on the one hand and exposure concentrations of organic dust or respiratory symptoms on the other hand.
Methods: In a cross sectional study among 47 waste collectors and 15 controls, questionnaire data on respiratory symptoms were collected. Nasal lavage (NAL), to assess upper airway inflammation, was performed before and after a work shift at the beginning and at the end of the working week. In NAL fluid, cells were counted and differentiated and concentrations of interleukin 6 (IL6), IL8, tumour necrosis factor-α (TNFα), and IL1β were measured. In collectors, inhalable dust samples were collected in which bacterial endotoxin and mould β(1→3)-glucan were assessed.
Results: Prevalence of respiratory symptoms was higher in waste collectors than in controls. Geometric mean exposure concentrations were 0.58 mg/m3 for dust, 39 EU/m3 for endotoxin, and 1.3 μg/m3 for β(1→3)-glucan. At the end of the week collectors had higher concentrations of total cells and IL8 in NAL before and after a shift than controls (cells, before 1.9-fold p<0.10, after 3.3-fold p<0.01; IL8, before and after 1.8-fold p<0.05), and after/before work shift ratios of total cells were also higher (2.3-fold p=0.06) in collectors than in controls. Cells in NAL fluid consisted predominantly of neutrophils and epithelial cells, whereas eosinophils and mononuclear cells were rarely found. Exposure to dust and endotoxin was associated with concentrations of IL8 after the shift (p<0.05). Increased concentrations of IL8 (p<0.05) and total cells (p<0.10) after the shift were associated with respiratory symptoms. Concentrations of IL6, TNFα, and IL1β were not associated with waste collecting, symptoms, or exposure.
Conclusions: Waste collectors show signs of increased upper airway inflammation and respiratory symptoms compared with controls. Exposure to organic dust probably underlies the inflammation mediated by neutrophils that result in respiratory symptoms.
- upper airway inflammation
- waste collecting
- respiratory symptoms
- organic dust
- NAL, Nasal lavage
- IL1β, interleukin-1β
- IL6, interleukin-6
- IL8, interleukin-8
- TNFα, tumour necrosis factor-α
- PR, prevalence ratio
Statistics from Altmetric.com
- NAL, Nasal lavage
- IL1β, interleukin-1β
- IL6, interleukin-6
- IL8, interleukin-8
- TNFα, tumour necrosis factor-α
- PR, prevalence ratio
Increased numbers of workers are involved in the household waste recycling industry, due to the recently introduced separate collection of organic and non-organic household waste in several European countries, as part of national or local environmental management policies. The health risks associated with this type of industry are, however, not yet clear. The few studies that assessed health risks1–6 showed that workers in waste handling, particularly workers collecting and processing domestic organic waste for composting, are at risk of developing various health effects—such as respiratory symptoms, systemic influenza-like symptoms, and gastrointestinal problems.
It is not clear which specific exposures and underlying mechanisms may induce these health effects. Waste workers are exposed to a heterogeneous mixture of bioaerosols, gases, and vapours—such as microbial and non-microbial volatile organic compounds.7–9 Moulds may induce allergic reactions, and case reports of hypersensitivity pneumonitis and allergic bronchopulmonary aspergillosis have been published.2,10,11 However, allergic diseases are rarely reported in surveys and are unlikely to explain the occurrence of most respiratory symptoms. Alternatively, non-allergic inflammatory reactions may be important, especially due to dust containing endotoxins and β(1→3)-glucans, two known proinflammatory cell wall components of gram negative bacteria and most fungi, respectively.5–7,12–15 The production of proinflammatory cytokines—such as interleukin-1β (IL1β), interleukin-6 (IL6), interleukin-8 (IL8), and tumour necrosis factor-α (TNFα)—plays a major role in these inflammatory processes.16,17
Recently, two studies have specifically related exposure to bioaerosol to the presence of airway inflammation and subsequent symptoms in workers in the household waste collecting5 and organic waste composting industry.6 In these studies, airway inflammation seemed to be mainly mediated by neutrophils and was independent of specific antibodies, probably caused by direct interaction of inflammatory biological agents such as endotoxins or glucans with epithelial tissues and infiltrating white blood cells. As these studies were small and associations were weak, no firm conclusions could be drawn as to which agents and underlying mechanisms may be responsible for the symptoms. Furthermore, due to the small study populations, confounding variables—such as smoking, age, and atopy—could not be dealt with appropriately in these studies.
In the present study we therefore investigated prevalence of respiratory symptoms and upper airway inflammation in a larger population of domestic waste collectors and controls. In all subjects nasal lavage (NAL) was performed before and after the work shift, to assess acute across shift effects, and at the beginning and at the end of the week, to assess across week effects. We assessed differences between waste collectors and controls by comparing concentrations before and after the shift of NAL variables and after/before shift ratios of NAL variables. Associations between markers of upper airway inflammation and exposure concentrations of dust, endotoxin, and glucan, and prevalence of respiratory symptoms were also assessed.
Main messages
-
Household waste collectors are exposed to microbial agents—such as bacterial endotoxins and β(1–3)-glucans irrespective of the type of rubbish they handle.
-
Domestic waste collectors showed signs of increased prevalence of respiratory symptoms and showed increased concentrations of variables indicative of upper respiratory inflammation in nasal lavage compared with controls.
-
The exposure to microbial agents is probably associated with the increased prevalence of respiratory symptoms and variables indicative of upper respiratory inflammation in nasal lavage fluid.
-
Within the group of waste collectors a dose-response relation between exposure and increased concentrations of inflammatory variables in nasal lavage fluid was found.
-
People with respiratory symptoms more often had increased concentrations of inflammatory mediators, especially IL8 and increased numbers of cells in nasal lavage fluid.
Implications
-
Exposure of waste collectors to microbial agents is relatively low. Despite the low levels, a respiratory inflammatory response is measurable. The importance of this response for long term effects is not known but needs to be established.
METHODS
Subjects and process description
All domestic waste collectors of the municipal waste collecting facilities of four large Dutch cities (over 100 000 inhabitants) were approached to participate in the current study. Participants were approached by the facilities due to privacy regulations. As a result no information could be obtained on response rate, as the total number of people approached by the facility was not available to us, and consequently no information on characteristics of non-responders could be obtained.
Three major job tasks were distinguished: driving, loading, and driving/loading (driving and loading were carried out alternately on the same day). During the week, job task rotation occurred. Collected waste was either non-separated mixed waste or separated organic and non-organic/residual waste fractions. As well as the waste collectors, office workers of the same four facilities were included as unexposed controls. The offices of the office workers were about 100–600 m from the garage where the waste collecting trucks were parked, and thus were not likely to be as highly exposed to organic dust as waste collectors.
Study design
Fieldwork was performed from June to September 1997. All subjects filled out a health questionnaire and underwent nasal lavage (NAL) before and after the work shift at the beginning and at the end of the week, for a period of 1–2 weeks. The NAL was conducted on Monday or Tuesday (beginning of the working week) and on Wednesday, Thursday, or Friday (end of the working week), always allowing 2–3 days between NALs at the beginning and end of the working week. Each person had between two and eight NALs. In waste collectors only, personal exposure measurements were performed at the same days as the NALs resulting in 1–4 exposure measurements per collector. In total 47 waste collectors and 15 controls participated in the NAL, questionnaire, and exposure measurement (for collectors only) as part of the research protocol. Thirty six waste collectors and 11 controls also provided a blood sample for serology measurements. The medical ethics committee of Wageningen University approved the study and participants gave informed written consent.
Questionnaire
A self administered questionnaire was developed specifically for the waste recycling and composting industry18 and comprised questions from the British Medical Research Council respiratory symptoms questionnaire,19 questions about symptoms suggestive of respiratory allergies and hyperresponsiveness,20 and questions about upper and lower respiratory symptoms during the past year.2,4,21 Also, questions on job history and smoking habits were asked.
Serology
Serum samples were collected by venipuncture. In the serum total IgE and specific IgE against common allergens (grass pollen mix, birch pollen, house dust mite, and cat dander) and specific IgE against mould allergens (Cladosporium species (mixed Cladosporium cladosporiodes, Cladosporium elatum, Cladosporium herbarum), Aspergillus species (mixed Aspergillus versicolor, Aspergillus fumigatus, Aspergillus amstelodami, Aspergillus nidulans), Penicillium species (mixed Penicillium brevicompactum, Penicillium expansum, Penicillium notatum, Penicillium commune), and Aspergillus fumigatus) were measured by an enzyme immunoassay as described previously by Doekes et al.22 All allergens were obtained as lyophilised extracts from ALK (Nieuwegein, The Netherlands).
Nasal lavage
Nasal lavage (NAL) was performed as described previously.6 Cells in the NAL fluid were counted and a cytospin was made for cell differentials. Interleukin-6, IL8, IL1β, and TNFα were measured in the fluid by enzyme immunoassays (Biosource, Biosource Europe SA, Fleurus, Belgium). The limits of detection were 45 pg/ml for TNFα, 6.2 pg/ml for IL1β, 0.5 pg/ml for IL6, and 2.5 pg/ml for IL8.
Exposure measurements
Full shift personal inhalable dust samples were collected with Gillian P5 portable constant flow pumps at a flow rate of 3.5 l/min in combination with GSP-samplers23 equipped with Whatman GF/A glass fibre filters (37 mm diameter). Dust, endotoxin,24 and β(1→3)-glucan25 measurements were performed as described previously. Limits of detection were 0.2 mg/m3 for dust, 4 EU/m3 (endotoxin units) for endotoxin, and 0.26 μg/m3 for glucan.
Statistical analysis
Data were analysed with SAS statistical software (version 6.12; SAS institute, Cary, NC, USA). Concentrations that were below the limits of detection were assigned a value of two thirds of the detection limit.26 To assess acute (across shift) effects, after/before shift ratios of total cell, IL8, and IL6 concentrations were calculated. Levels of exposure, NAL variables, and NAL after/before shift ratios were natural log transformed before statistical analysis to ensure normality of the data. Because of high numbers of non-detectable concentrations of TNFα and IL1β in NAL measurements (both 74%), TNFα and IL1β data were dichotomised based on the limit of detection (detectable versus non-detectable), and acute effects were not studied.
A mixed effects models (an extension of multiple regression analysis for correlated observations) were used to analyse relations between NAL and being a collector or control, between NAL and exposure, and between exposure and exposure determinants correcting for first order autocorrelation between repeated measurements and with and without adjustment for potential confounding variables. By including an interaction term for exposure (collector v control) and day of the week (beginning v end of the week NAL) differences in across week changes were tested for. Also, we applied mixed models to obtain estimates of variance of the dependent variable within and between subjects. Mixed model linear regression analyses were used for continuous variables and mixed model multiple logistic regression analyses for dichotomised variables.27,28
Prevalence ratios (PR) for the respiratory symptoms were calculated by means of log binomial regression analyses29 to assess the association between health symptoms and outcomes of nasal lavage before and after the shift. As health symptoms were recorded only once per subject, NAL outcomes were first reduced to one value for before and after the work shift, by calculating the median value of repeated NAL measurements per subject. These median values were then dichotomised at the population median (based on the median value of each person): 1442 cells/ml, 190 pg/ml for IL8, 1.1 pg/ml for IL6, and detectable concentrations of TNFα and IL1β.
RESULTS
Descriptive characteristics of the research population are listed in table 1. Waste collectors were not sensitised to moulds as no specific IgE against mould allergens was found in waste collectors, whereas three control subjects (27%) had increased IgE against mould allergens (all single allergen sensitisation to either Aspergillus species, Cladosporium species or Aspergillus fumigatus). Sensitisation to common allergens was found in both waste collectors and controls; IgE against grass pollen was 22% in collectors and 45% in controls, house dust mite 17% and 9%, birch pollen 0% and 27%, and cat dander 8% and 0%. Total IgE was increased (>100 kU/l) in 25% of the collectors and 36% of the controls. Of the collectors and controls, 40% and 63% were atopic, defined as increased total IgE or specific IgE against common allergens or both.
Population characteristics and symptom prevalence in waste collectors and controls of four Dutch municipal waste facilities
In total 120 full shift personal exposure measurements were available for statistical analysis after excluding 11 samples due to technical measurement errors. No clear differences in exposure levels for different types of waste (organic versus non-organic or residual waste) were found. Highest dust, endotoxin, and glucan exposures (p<0.05, table 2) were found while loading waste. Estimated variance in components were 0.51 and 0.34 for dust, 1.08 and 0.22 for endotoxin, and 1.49 and 0.14 for glucan. Thus, day to day variability in exposure was large, relative to differences in exposure between people, especially for endotoxin and glucan.
Exposure levels of inhalable dust, endotoxin from microbial agents, and β(1→3)-glucans in domestic waste collectors
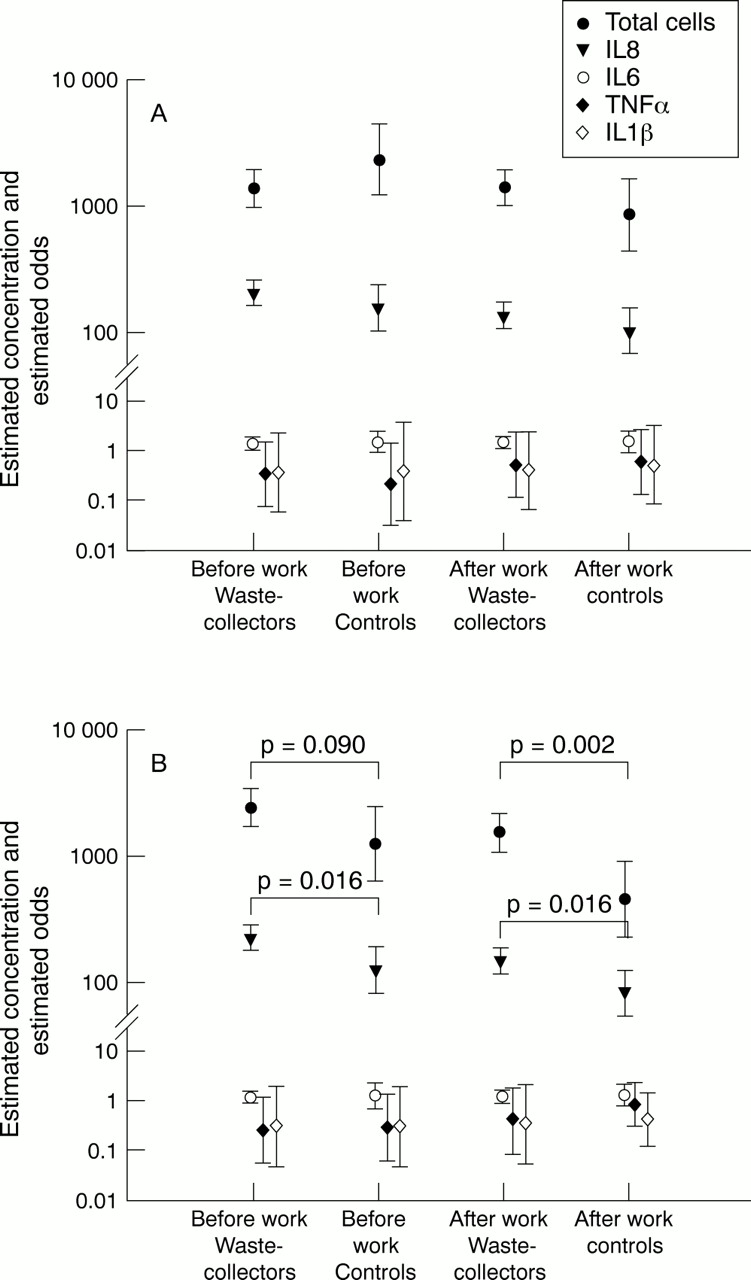
A total of 268 NAL fluids was collected from waste collectors and 57 from controls. The recovery of nasal lavage fluid was the same for waste collectors and controls both before and after the work shift. Average nasal lavage fluid recoveries were 5.8 ml (SD 1.5) and 5.8 ml (SD 1.4) before the work shift, and 6.2 ml (SD 1.4) and 6.0 ml (SD 1.1) after the work shift for waste collectors and controls, respectively. Cells in NAL fluid consisted predominantly of neutrophils (mean percentage 55% for collectors and 54% for controls) and epithelial cells (both 44%), whereas eosinophils (0.7% and 2.1 %) and mononuclear cells (0.3% and 0.2%) were only occasionally present. Results from the regression analyses adjusted for autocorrelation are presented in figure 1. At the beginning of the week, no significant differences between waste collectors and controls in NAL inflammatory marker concentrations were found. Whereas, at the end of the week, waste collectors had higher concentrations of total cells (before shift 1.9-fold p=0.090; and after shift 3.3-fold p=0.002), and higher concentrations of IL8 (before and after the shift 1.8-fold; p=0.016) than controls. Significant (p<0.10) different effects across the week in waste collectors versus controls were. No significant differences between collectors and controls were found in concentrations of IL6, TNFα, and IL1β. Estimated variance components between and within person were 0.89 and 1.00 for total cells, 0.53 and 0.23 for IL8, and 0.79 and 0.39 for IL6. Analyses restricted to people who had worked in their present job for more than 6 months (excluding about 21% of collectors, table 1) gave similar results. Two other possible confounding variables, smoking and age, were not associated with any of the lavage variables, and analyses adjusting for smoking and age did not significantly change the results (regression coefficients that reflect the difference between collectors and controls changed with maximal −7% to +14%, data not shown). Atopic people had higher values for IL8 and lower number of cells, but the differences were not significant. Correction for atopy and a separate analyses for atopic and non-atopic people did not give any different results.

Geometric mean (95% CI) of concentrations in NAL fluid of total cells (cells/ml), IL8 ( pg/ml), and IL6 (pg/ml), and the odds for detectable TNFα and IL1β, at the beginning (A) and at the end (B) of the week accounted for repeated measurements within subjects as estimated in mixed effects models.
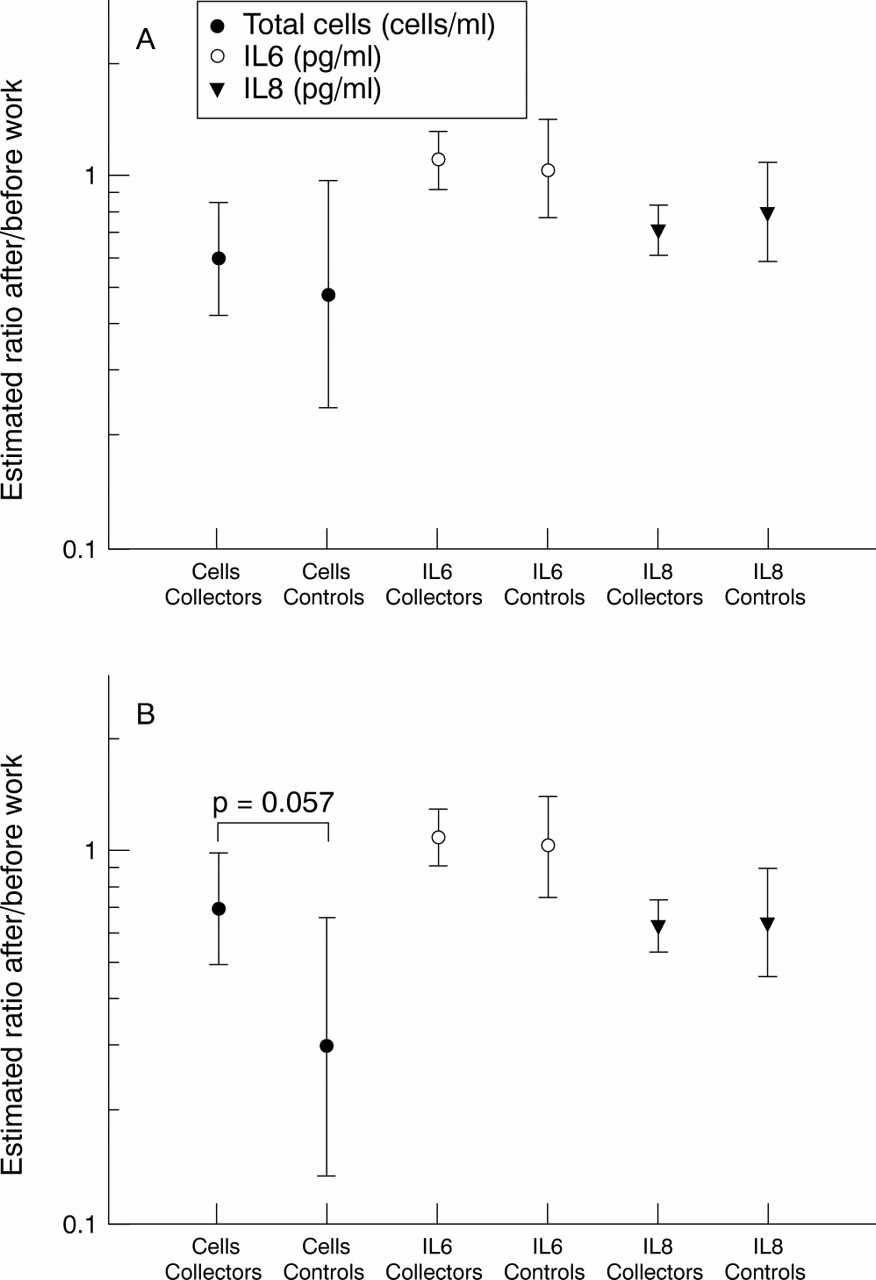
After/before work shift ratios, as a measure of acute effects of NAL inflammatory markers adjusted for autocorrelation are summarised in figure 2. No differences between waste collectors and controls were found at the beginning of the week. At the end of the week the after/before ratio of total cells was increased 2.3-fold (p=0.057) in waste collectors compared with controls. Adjustment for smoking and age did not significantly affect the results (data not shown). Estimates of the variance components between and within subjects were 0.14 and 1.80 for total cells, 0.07 and 0.30 for IL8, and 0.03 and 0.54 for IL6.

{kind=link}
{kind=link}
Geometric mean (95% CI) of work shift ratios of NAL total cells, IL6, and IL8 at the beginning (A) and end (B) of the week accounted for repeated measurements within people as estimated in mixed effects models.
As across week effects were found in NAL inflammatory markers before the work shift, associations between inflammatory markers and exposure concentrations were assessed with after work shift NAL concentrations only instead of after/before work shift ratios (table 3). Generally, after shift total cell and IL8 concentrations both at the beginning and at the end of the week, were positively associated with exposure concentrations of the same day as the NAL was performed (p<0.05 for IL8 and dust exposure). Moreover, after shift NAL concentrations at the end of the week were associated with approximates of week exposures (summed exposures of the beginning and end of the week); particularly IL8 concentrations were significantly associated with dust and endotoxin exposures (p<0.05). No clear associations between concentrations of IL6 and exposures were found. After shift NAL concentrations were not associated with job tasks or type of waste (data not shown).
Relation in waste collectors between concentrations after a work shift of total cells, IL6, and IL8 in NAL fluid and personal exposure concentrations on the same day as NAL was performed (day of exposure) or a proxy for accumulated exposure for a week (sum of exposures) approximated by summing the exposures at the beginning and the end of the week
Prevalence of respiratory symptoms and associations between respiratory symptoms and NAL inflammatory markers—total cells and IL8—are listed in table 4. Prevalence of health symptoms was slightly higher in waste collectors than in controls. Increased (above median) after shift IL8 concentrations were more common in subjects reporting respiratory symptoms, such as cough, cough with phlegm, wheezing, stuffy nose, and runny nose (PR range 1.6–7.7, p<0.05). Respiratory symptoms were also, but only weakly, associated with increased total cell concentrations after the shift (PR range 1.5–2.3, p<0.10). No associations were found between respiratory symptoms and dichotomised values of other inflammatory markers (IL6, TNFα, and IL1β). Analyses adjusting for collector/control status or current smoking and age showed similar results (data not shown). Separate analyses for collectors showed generally similar but slightly increased associations.
Prevalence of respiratory symptoms and prevalence ratios (PR) of respiratory symptoms for above versus below median NAL concentrations of total cells and IL8 in waste collectors and controls
DISCUSSION
In this study, we showed signs of increased upper airway inflammation and respiratory symptoms in waste collectors compared with controls. The inflammation was shown at the end of the working week by higher concentrations of total cells and IL8 before and after the shift, and higher cross shift cell counts in NAL fluid. No differences between waste collectors and controls were found for IL6, TNFα, and IL1β in NAL fluid. The main types of cells found in the NAL fluid were neutrophils and epithelial cells, whereas eosinophils were only occasionally found, which is indicative for a non-immune inflammation mediated by neutrophils as described previously in the waste industry.5,6 This was furthermore supported by the observed increased levels of IL8, a strong chemoattractant of neutrophils, and by the finding that IgE sensitisation against fungi was rarely found in either waste collectors and controls. Serum IgG antibody titres against fungi and actinomycetes were the same for waste collectors and controls (data not shown), which has recently also been shown by others.30
Although exposure concentrations of organic dust in waste collectors were lower than previously described for compost workers,6 signs of inflammatory responses were still found, but were less pronounced. Significant differences between waste collectors and controls in markers of upper airway inflammation (both before and after the shift) were found, but only at the end of the week, suggesting an across week effect. Concentrations of NAL variables in controls showed a strong decline during the week, probably due to a prolonged washout effect 2–3 days after the first NAL, which has been described previously in other studies.6,31,32 Assuming a comparable washout effect in both groups, the less pronounced decline in NAL concentrations during the week for waste collectors can only be explained by an enhanced and probably subchronic inflammatory process in the nasal mucosa of collectors. Similar across week effects were not found in our previous study in more highly exposed compost workers,6 which might have been due to the design of that particular study as controls were only measured at the beginning of the week. However, in that study signs of subchronic inflammation were shown by increased concentrations of inflammatory markers in the NAL of the most highly exposed workers compared with controls before the work shift.6
No differences between waste collectors and controls were found for the proinflammatory cytokines IL6, TNFα, and IL1β in NAL fluid. Although those cytokines are thought to play a crucial part in the inflammatory processes, concentrations of them in NAL fluid have been studied only rarely, showing no consistent results.33,34 Thus the reason for the lack in response of those cytokines remains uncertain.
In the present study in waste collectors, concentrations of inflammatory markers after the shift were positively associated with exposure concentrations. So far, associations between inflammatory markers in NAL fluid and occupational exposure concentrations have hardly been reported. The exposure-response relation found was more pronounced for total dust exposure than for endotoxin or glucan exposure alone, suggesting that other currently unidentified agents—for instance peptidoglycans—in the dust, besides endotoxin and glucan, may also play a part.35
The availability of repeated exposure and NAL measurements allowed calculation of variance components between and within subjects, where the variance between subjects reflects differences between people and the variance within subjects the day to day variation within a person. Our data showed that between and within subject variability was not the same for each NAL marker, as the total variance for IL6 and total cell concentrations was larger than for IL8 concentrations. Variability between subjects was about twice that of variability within subjects, thus showing larger differences in concentrations of NAL inflammatory markers between people than within people, which has been described previously.32 The variability of NAL inflammatory markers between and within subjects did not change after correction for being a collector or a control or time of NAL or exposure (data not shown), which has been reported previously by Hauser et al.32 This suggests that differences between people in responses exists independently of exposure, which may be due to other undetermined factors—such as individual susceptibility—that have been described for endotoxin related airway responsiveness.17,36,37
In the present study, an association between respiratory symptoms and NAL variables was shown by increased concentrations of IL8 and total cells after the shift in subjects reporting respiratory symptoms. An analysis including exposed workers only did overall yield higher risk ratios, suggesting that at least part of the association between NAL outcomes and respiratory symptoms is related to occupational exposure. To our knowledge, only one other small study in bakers has reported increased concentrations of NAL variables in the presence of nasal symptoms.38 In that study associations between symptoms and NAL were only found in bakers and not in controls.
In conclusion, waste collectors showed signs of increased upper airway inflammation and showed a slightly higher prevalence of respiratory symptoms compared with controls. Exposure to organic dust probably underlies the non-immune inflammation characterised by attraction and infiltration of neutrophils, resulting in respiratory symptoms.
Acknowledgments
We are indebted to the waste collectors and the waste collecting facilities for their participation and cooperation in the study. We also thank Isabella van Schothorst, Jack Spithoven, and Siegfried de Wind for their technical assistance in exposure measurements and laboratory analyses, and Professor B Brunekreef for reviewing the manuscript. This study was financially supported by the Ministry of Social Affairs and Employability, The Netherlands Organisation for Scientific Research (NWO), and the European Commission (BMH4-CT96-0105).
REFERENCES
Linked Articles
- Correction