Article Text

Abstract
Aims: To investigate whether Australian Gulf War veterans have a higher than expected prevalence of recent symptoms and medical conditions that were first diagnosed in the period following the 1991 Gulf War; and if so, whether these effects were associated with exposures and experiences that occurred in the Gulf War.
Methods: Cross-sectional study of 1456 Australian Gulf War veterans and a comparison group who were in operational units at the time of the Gulf War, but were not deployed to that conflict (n = 1588). A postal questionnaire was administered and the likelihood of the diagnosis of self-reported medical conditions was assessed and rated by a medical practitioner.
Results: Gulf War veterans had a higher prevalence of all self-reported health symptoms than the comparison group, and more of the Gulf War veterans had severe symptoms. Increased symptom reporting was associated with several exposures, including having more than 10 immunisations, pyridostigmine bromide tablets, anti-biological warfare tablets, pesticides, insect repellents, reportedly being in a chemical weapons area, and stressful military service experiences in a strong dose-response relation. Gulf War veterans reported psychological (particularly post-traumatic stress disorder), skin, eye, and sinus conditions first diagnosed in 1991 or later more commonly than the comparison group. Over 90% of medical conditions reported by both study groups were rated by a medical practitioner as having a high likelihood of diagnosis.
Conclusion: More than 10 years after the 1991 Gulf War, Australian veterans self-report all symptoms and some medical conditions more commonly than the comparison group. Further analysis of the severity of symptoms and likelihood of the diagnosis of medical conditions suggested that these findings are not due to over-reporting or to participation bias.
- ADF, Australian Defence Force
- adj OR, adjusted odds ratio
- DU, depleted uranium
- DVA, Department of Veterans’ Affairs
- HSA, Health Services Australia
- MSE questionnaire, Military Service Experience questionnaire
- OR, odds ratio
- PTSD, post-traumatic stress disorder
- SD, standard deviation
- SF-12, 12-item version of the Short-Form Health Survey
- Gulf War
- symptoms
- medical conditions
Statistics from Altmetric.com
- ADF, Australian Defence Force
- adj OR, adjusted odds ratio
- DU, depleted uranium
- DVA, Department of Veterans’ Affairs
- HSA, Health Services Australia
- MSE questionnaire, Military Service Experience questionnaire
- OR, odds ratio
- PTSD, post-traumatic stress disorder
- SD, standard deviation
- SF-12, 12-item version of the Short-Form Health Survey
In the 1991 Gulf War, Australia deployed 1871 Australian Defence Force personnel to the Gulf area as part of a larger multinational response to the invasion of Kuwait by Iraq on 2 August 1990.
Since 1992 there has been a sustained international effort to investigate the health complaints of Gulf War veterans, with self-reported symptoms, medical conditions, and other general health outcomes measured in postal or telephone surveys conducted through cross-sectional studies of Gulf War veterans from the UK,1–3 the USA,4–8 Denmark,9 and Canada.10 A common finding of these studies is that health problems such as self-reported symptoms, medical conditions, functional impairment, and perception of poor health are more common among Gulf War veterans than their military comparison groups; and that adverse health outcomes are associated with a number of Gulf War exposures including immunisations, smoke from oil well fires, pyridostigmine bromide, pesticides, and stressful experiences.
Gulf War health research has done much to clarify the health problems of Gulf War veterans, but has had some limitations.11–13 These limitations have included health outcomes and exposure data based solely or mainly on self-report, self-referred populations in registry studies, problems in objectively measuring exposures, and difficulties locating and contacting study participants. Typically, participation by the non-deployed comparison groups have been low,1,4,9,10,14 rendering the results of these studies vulnerable to participation bias.
The current study investigated whether Australian Gulf War veterans have a higher than expected prevalence of self-reported symptoms and of medical conditions that were first diagnosed in the period since the Gulf War. If adverse health effects were found to be higher in Gulf War veterans, associations with exposures and experiences that occurred in the Gulf War were explored. In addition, the characteristics of self-reported symptoms and medical conditions, and the effect of possible participation bias, were investigated further.
METHODS
The study was approved by the Standing Committee on Ethics in Research Involving Humans at Monash University, the Department of Veterans’ Affairs (DVA) Human Research Ethics Committee, and the Australian Defence Human Research Ethics Committee.
Study population
The study population was the entire cohort of 1871 Australian veterans who served in the Gulf region during the period from 2 August 1990 to 4 September 1991. A comparison group of 2924 subjects was randomly selected from 26 411 Australian Defence Force (ADF) personnel who were in operational units at the time of the Gulf War, but were not deployed to that conflict. They were frequency matched to the Gulf War group by service type, sex, and three year age band, and additionally by officer/non-officer status within the Army subgroup and by aircrew/non-aircrew status within the Air Force subgroup. The comparison group was over-sampled in anticipation of lower participation within this group.
Main messages
-
Australian Gulf War veterans report all symptoms more commonly than expected, and more of the Gulf War veterans report symptoms that are more severe in nature.
-
Australian Gulf War veterans report psychological (particularly post-traumatic stress disorder), skin, eye, and sinus conditions more commonly than expected.
-
The likelihood of the diagnosis of self-reported medical conditions is high in both study groups, and increased reporting of medical conditions by Gulf War veterans does not appear to be explained by over-reporting.
-
Increased symptom reporting in Gulf War veterans is associated with several medical, environmental, and chemical exposures and stressful military service experiences reported in relation to the 1991 Gulf War.
Recruitment
Recruitment commenced in August 2000 and concluded in April 2002. Subjects were recruited via mailed invitations with two further mailings and follow up phone contact for non-responders. Measures to maximise participation included personally addressed invitations to participate, a letter of endorsement from the Minister for Veterans’ Affairs, and reimbursement of expenses or income lost as a result of participation. Last known addresses were obtained from several databases including those of DVA and Department of Defence, the electoral roll, health authorities, and telephone directories.
Data collection
Participation in the study included completing a postal questionnaire and undergoing a comprehensive health assessment which was carried out by specially trained doctors, nurses, and psychologists at 10 Health Services Australia (HSA) clinics located around Australia. Some subjects, who were unable or unwilling to attend the health assessment, completed the postal questionnaire only.
Instruments
The self-administered postal questionnaire asked about demographic and military service details, exposure history, tobacco use, alcohol consumption, health symptoms, and medical conditions.
The 63 item self-report symptom questionnaire asked about the occurrence of symptoms in the past month, and whether the severity of those symptoms was “mild”, “moderate”, or “severe”. The 58 item medical condition questionnaire asked about problems or conditions that had been diagnosed or treated by a medical doctor, and the year in which the condition was first diagnosed. The symptom and medical questionnaires were based on those used by Unwin and colleagues,1 but included additional items considered relevant to Australian veterans.
Policy implications
-
Efforts should be made to ensure that record keeping in relation to immunisations and other exposures experienced during deployment is complete.
-
Defence health services should ensure that there is optimal preparation for deployment, means are in place to detect increased symptom or medical conditions reporting in returning veterans, and treatment facilities are available for medical conditions we found to be in excess.
Gulf War veterans were asked to refer to their immunisation booklet, if available, for details about the total number of immunisations received, the timing of these in relation to their Gulf War deployment, the time period over which they received them, and the individual immunisations received. Veterans were also asked about the duration and quantity of any anti-nerve agent (pyridostigmine bromide) tablets taken, and the duration in days of any antimalarial or anti-biological warfare tablets taken. A 28 item chemical and environmental exposure questionnaire asked veterans to identify exposures that they experienced during the Gulf War including dust storms, intense smoke from burning oil wells, pesticides, insect repellents, being in an area where chemical warfare agents had probably been used, and possible exposure to depleted uranium.
In investigating the relation between self-reported exposures and total number of symptoms in Gulf War veterans, possible exposure to depleted uranium was defined on the basis of whether the veteran was in Camp Doha, Kuwait when the tank compound caught fire or was involved in the subsequent clean up operations, or if they reported either using depleted uranium munitions or entering or inspecting destroyed enemy equipment and had been in either Kuwait or in the battle zone areas. DVA Nominal Roll deployment information was used to group veterans according to whether their deployment was completed before or after the commencement of the air war against Iraq on 17 January 1991. A cluster of immunisations was defined as more than five immunisations within one week or less.
Exposure to psychological stressors during the Gulf War was measured using the 44 item Military Service Experience (MSE) questionnaire which was developed specifically for this study15 as existing war-stress questionnaires appeared to inadequately explore the experiences of navy groups in particular. Themes included fear and threat of injury or death or attack, including the threat of nuclear, biological, or chemical attack, feelings of helplessness and lack of control, poor preparation, malevolent environment, lack of support, and lack of unit cohesion. The instrument was derived from various sources including the findings from a focus group of Australian Gulf War veterans and modified items from pre-existing combat exposure questionnaires.16–20 The MSE questionnaire was scored by summing the number of positive responses, providing a score range of 0 to 44.
During the medical assessment, the HSA doctor, who was blinded to the Gulf War status of the participant, asked the subject further questions about each reported medical condition and classified the self-reported diagnosis as “non-medical” if the condition had not been diagnosed or treated by a medical doctor. If the reported condition had been diagnosed or treated by a medical doctor, the likelihood of the diagnosis was classified as “unlikely”, “possible”, or “probable” according to specified criteria that related to consistency of history of the condition with the diagnosis, and whether confirmatory investigations, treatment, or specialist referral had been undertaken by the person’s doctor in relation to the condition. This was done to improve the accuracy of the classification of these self-reported diagnoses.
Statistical methods
Statistical analyses were performed using Stata version 7.21 Associations between Gulf War deployment and symptoms and medical conditions, adjusting for potentially confounding factors, were assessed using logistic regression22 and reported as adjusted prevalence odds ratios (adj OR) with 95% confidence intervals (95% CI). In the analysis of medical conditions first diagnosed in 1991 or later, medical conditions that were first diagnosed in 1990 or earlier (that is, prior to the Gulf War) were excluded from the analysis. Where less than five subjects in either study group experienced the outcome of interest, exact logistic regression was performed.23 Likelihood ratio tests22 were performed to investigate homogeneity of the effects of study group across categories of age, rank, and service type for total symptom count. These were performed using interaction terms added to the logistic regression model. The ratio of means for total symptom count and total number of medical conditions were adjusted for possible confounders by negative binomial regression, which is a statistical technique that allows for greater dispersion of counted values than does a Poisson regression.24 The ratio of means is reported as this is a natural summary measure for analysis of counts using negative binomial regression.25 The values of the crude, and the adjusted, odds ratios and ratio of means were found to be highly similar, and so only the adjusted results are reported.
To explore the relation between total symptom count and Gulf War related exposure to immunisations, psychological stressors, pyridostigmine bromide, and antimalarial and anti-biological warfare tablets in Gulf War veterans, exposure-response trends were computed using the number of immunisations and the MSE questionnaire score as linear variables and the number of pyridostigmine bromide tablets taken (none, 1–80, 81–180, >180 tablets), and the number of days antimalarial and anti-biological warfare tablets were taken (none, 1–30, 31–90, >90 days of tablets taken) as categorical variables in the relevant regressions.
To investigate the possible effects of participation bias on our results, we collected brief demographic and health status (Short-Form 12 (SF-12) Health Survey26,27) data from a telephone survey of non-participants. Study participants who completed the postal questionnaire also completed the SF-12. A prediction model was used to compute age, rank, and service adjusted odds ratios for the relative health outcomes of Gulf War veterans versus comparison group subjects, as if the study had achieved full participation. The predicted “full participation” adjusted odds ratios were averaged over 100 replications of the analyses, as described previously.15
RESULTS
Participation
From the original study sample of 1871 Gulf War veterans, 1456 (80.5%) of 1808 recruitable (not reportedly deceased or overseas) subjects participated, including 1414 (78.2%) who completed the health assessment and postal questionnaire, and 42 (2.3%) who completed the postal questionnaire alone. Of the 2924 comparison group subjects, 1588 (56.8%) of 2796 recruitable subjects participated, with 1411 (50.5%) completing the health assessment and postal questionnaire, and 177 (6.3%) completing the postal questionnaire alone.
Demographic characteristics
Due to the very small number of female veterans, the analyses were limited to male subjects. Demographic and socioeconomic characteristics of male participants have been reported previously.15 Among male subjects who completed the postal questionnaire, Gulf War veterans were slightly younger than comparison group participants, more likely to have served in the Navy, been of lower rank, and less likely to have a tertiary education—that is, an undergraduate or postgraduate degree. There were no differences in other demographic or socioeconomic characteristics of participants. Subjects who were younger and of lower rank were least likely to participate in both study groups. Air Force subjects were least likely to participate in the Gulf War veteran group, and most likely to participate in the comparison group.
Investigation of possible effects of participation bias
The telephone survey for non-participants, on which part of the prediction model for assessing possible participation bias was based, was completed by approximately one quarter (n = 411) of all study non-participants, and the prediction model assumed that the telephone respondents’ answers were representative of those of the remainder of the non-participants.
The predicted full participation adjusted odds ratio for self-reported fatigue in the past month was 1.36, which was only marginally lower than the observed odds ratio of 1.42 found among participants. For doctor diagnosed back/neck problems and doctor diagnosed post-traumatic stress disorder (PTSD), the corresponding results were 0.97 (predicted) versus 0.99 (observed), and 2.85 (predicted) versus 2.86 (observed), respectively.
Symptoms
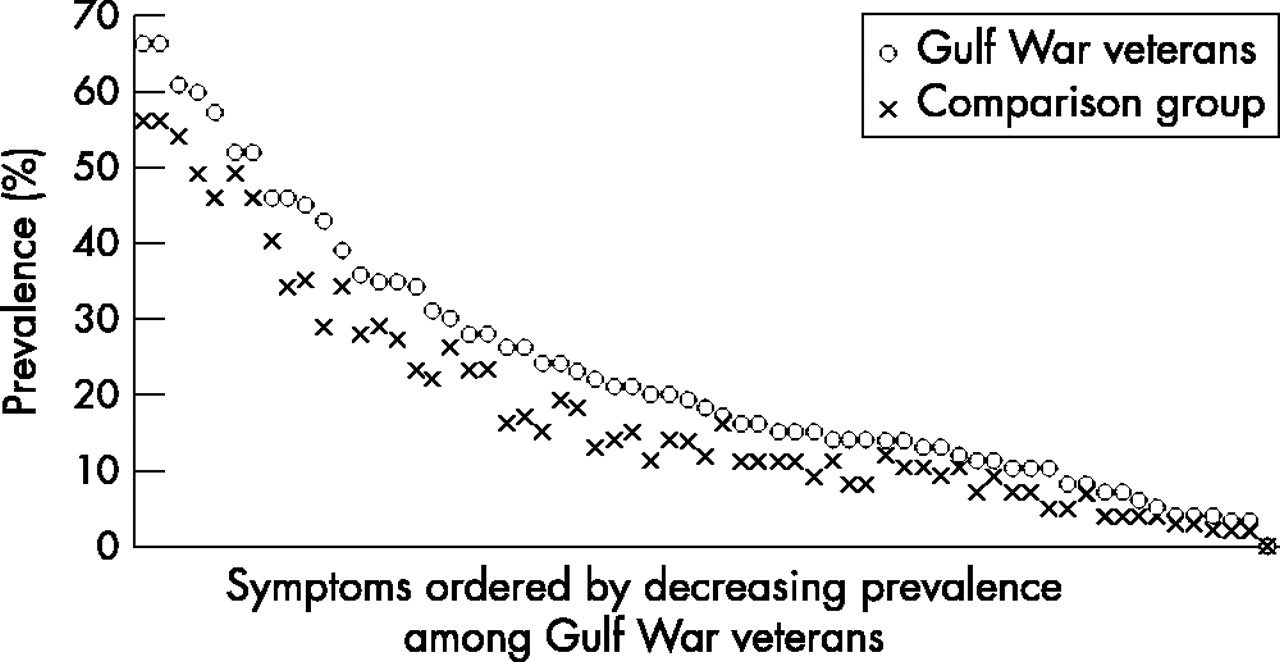
The pattern of symptom reporting (fig 1) shows that Gulf War veterans reported all 63 symptoms more commonly than the comparison group, and all but seven of the differences were statistically significant. Table 1 shows the results for the 15 most frequently reported symptoms in the past month. When the analysis was confined to moderate or severe symptoms, most of the odds ratios increased, indicating that more Gulf War veterans reported severe symptoms.
Prevalences, odds ratios (OR), and 95% confidence intervals (95% CI) of the 15 most frequently self-reported symptoms in the past month ordered by decreasing prevalence in the Gulf War group

{kind=link}
Pattern of self-reported symptoms in the past month by Gulf War deployment status.
The mean total number of self-reported symptoms was significantly higher for Gulf War veterans (table 2). The differences across subgroups of age and rank approached statistical significance, with higher symptom reporting in younger veterans and in more junior ranks.
Association between total number of self-reported symptoms and service type, rank, and age
Medical conditions first diagnosed in 1991 or later
Of the 15 most commonly self-reported medical conditions in the Gulf War veteran group, shown in table 3, the most commonly reported were musculoskeletal, skin, and psychological conditions. Increased reporting in Gulf War veterans was statistically significant for about half of these conditions, and the strongest association was for post-traumatic stress disorder (PTSD). When the analysis was confined to conditions that had been rated as a “possible” or “probable” diagnosis, the results were very similar (table 3).
Prevalences, odds ratios (OR), and 95% confidence intervals (95% CI) of the 15 most frequently self-reported doctor diagnosed or treated medical conditions first diagnosed in 1991 or later
Gulf War veterans reported a 20% higher mean total number of conditions first diagnosed in 1991 or later (mean (SD) 2.4 (2.4) v 2.0 (2.0), adjusted ratio of means 1.2 (95% CI 1.1 to 1.3), p < 0.001), as well as a 20% higher mean total number of “possible” or “probable” conditions first diagnosed in 1991 or later (mean 2.2 (2.2) v 1.9 (1.8), adjusted ratio of means 1.2 (95% CI 1.1 to 1.3), p < 0.001).
The results of the medical assessment of the likelihood of the diagnosis showed that of the medical conditions reported by Gulf War veterans, 91.3% were medically assessed to be “possible” or “probable” diagnoses, which was a little lower than the 93.2% of the comparison group.
Gulf War exposures
Of 1418 Gulf War veteran subjects, 726 (51.2%) indicated that they had their immunisation booklets to refer to. Veterans who had their immunisation booklets reported higher numbers of immunisations, and were also less likely to report that they had not received any immunisations, than subjects who did not have their immunisation booklets (data not shown).
Table 4 shows that the total number of health symptoms self-reported in the past month by Gulf War veterans was associated with increasing numbers of immunisations in a dose-response relation, indicating that there is an expected increase of 4% in the expected number of symptoms reported per each additional immunisation received among those reporting at least one immunisation. The total number of symptoms was associated with having at least 10 immunisations, but not with having any immunisations or with having a cluster of immunisations. The total number of symptoms was also greater in those who reported that they did not know the number of immunisations they received.
Association of Gulf War veterans’ total number of health symptoms with reported number of immunisations received in relation to their Gulf War deployment
Table 5 shows that the total number of health symptoms self-reported in the past month was associated with several other Gulf War exposures. These exposures included taking pyridostigmine bromide or anti-biological warfare tablets, exposure to pesticides, using insect repellents, and reportedly being in a chemical weapons area. The total number of health symptoms was associated with an increasing number of days that anti-biological warfare tablets were taken, in a dose-response relation, and with increasing numbers of stressful military service experiences during the Gulf War, as measured by an increasing MSE questionnaire score, in a strong dose-response relation. The total number of symptoms was also greater in those who reported that they did not know whether they had received medications such as pyridostigmine bromide or anti-biological warfare tablets. There was no association with other exposures such as taking antimalarials or possible exposure to depleted uranium.
Association of Gulf War veterans’ total number of health symptoms with reported Gulf War exposures and experiences
DISCUSSION
Our study has found that Australian Gulf War veterans reported significantly more health symptoms than ADF personnel who did not deploy to the 1991 Gulf War. The medical conditions with the largest associations with Gulf War service included post-traumatic stress disorder and skin conditions. While back, neck, and other joint problems were the most commonly reported medical conditions in the Gulf War veterans, these were also the most commonly reported conditions in the comparison group, with little difference between the two study groups. The combination of self-reported health outcomes from a postal questionnaire with data obtained through a face-to-face medical assessment, allowed more objective assessment of self-reported medical conditions than previous research in this field.
Gulf War veterans do not appear to be over-reporting medical conditions or symptoms of a mild nature compared with the comparison group. Gulf War veterans are more likely to report symptoms that are more severe in nature and are about as likely to report medical conditions that were subsequently assessed as “possible” or “probable” diagnoses as the comparison group. A similar and high proportion (over 90%) of medical conditions reported by both study groups were medically assessed as being “possible” or “probable” diagnoses, indicating a similar and small amount of over-reporting in both study groups. Our results show odds ratios typically less than two in magnitude, and mean number of symptoms in the order of 30% higher in Gulf War veterans than the comparison group. These figures still represent increases of substantive importance however.
Several previous studies have also found increased reporting of multiple symptoms by Gulf War veterans1,2,4,6 and a similar ordering of symptoms reported by the Gulf War and their comparison groups.1,2 Symptoms most commonly reported by Gulf War veterans in our study are also among the symptoms most commonly reported by US, UK, and Danish Gulf War veterans.1,2,4,5,9,28 The use of different terminology and definitions for symptoms in the different studies can make comparisons difficult. However, the symptom questionnaire in our study was based on that used by Unwin and colleagues.1 A comparison of our results with their published data1 for these most common symptoms shows that the symptoms most commonly reported in both studies were similar. Our comparison group of non-deployed ADF personnel had higher symptom prevalences than the UK “Era” comparison group who were not deployed to either the Gulf War or Bosnia. The odds ratios (and also absolute difference in prevalences) for individual symptoms in our study were lower than those for the same symptoms in UK Gulf War veterans. We think that this finding probably relates more to the relatively higher prevalence of symptoms in our comparison group, than to the later timing of our study and any reduction in the differences between study groups over time.
In several other studies, the pattern of self-reported medical conditions has been similar to that of symptoms, with Gulf War veterans reporting many4,6 or all1 of the medical conditions more frequently than non-Gulf veterans. Again, the use of different terminology or definitions for medical conditions1,4 limits direct comparisons between studies, but there appears to be less similarity in the ordering of medical conditions between our study and that of Unwin and colleagues1 than was found for the ordering of symptoms.
We found that the difference between Gulf War veterans and the comparison group in the total number of symptoms reported was more marked in the younger age group (<20 years) and in those of lower rank. These differences did not differ significantly across the subgroups of age, rank, or service type. Increased symptom reporting has been found to be greater in younger veterans (<25 years),2 Army veterans,2,4 and ranks other than officers.2 A strong association between rank and ill health has been reported in UK Gulf War veterans.29 We had relatively small numbers of Army and Air Force participants, which limited our ability to explore possible differences between the study groups for these service types.
Our finding of an association between having 10 or more immunisations and increased symptom reporting in Gulf War veterans is in general agreement with previous studies’ findings of an association between multiple (>6) immunisations and a multi-symptom illness,1 and number of immunisations and symptom severity score.3 We did not find having a cluster of immunisations to be associated with increased symptom reporting, although multiple immunisations during deployment has previously been found to be associated strongly with a multi-symptom illness.30 The total number of symptoms in our study was also greater in those who reported that they did not know the number of immunisations they received. The Gulf War veterans’ uncertainty and the poor quality of the immunisation data makes it difficult to draw firm conclusions.
Our finding of an association between increased symptom reporting and taking anti-biological warfare tablets, or increasing numbers of anti-biological warfare tablets in a dose-response relation, has not been reported elsewhere.1,3,6 We found that increased symptom reporting was associated with increasing number of stressful Gulf War military service experiences in a strong dose-response relation. While some studies report associations with a limited range of specific individual experiences, such as feelings that life was in danger3 or seeing dismembered bodies,1 these studies have not used a comprehensive measure of Gulf War related stressors to investigate the dose-response relation.
Some exposures that we found to be associated with increased symptom reporting have also been found in some of these other studies, although variation in outcomes reported, from symptom severity scores2 to symptom or instrument based definitions of medical and psychiatric conditions,1,6 limit direct comparisons. Our findings of an association with reportedly being in a chemical weapons area concurs with an association with belief of exposure to a chemical attack in UK veterans1 and exposure to chemical warfare agents in US veterans.6 Our finding of an association between pyridostigmine bromide tablets and exposure to pesticides and increased symptom reporting has also been reported in UK1,3 and US6 veterans. Lack of an association with antimalarial tablets has also been reported in relation to UK veterans.3
Many Gulf War exposures could have occurred together, and therefore attribution of a specific health outcome to a specific exposure is problematic.1,3,6,7,10,31,32 One finding that argues against attributing adverse health outcomes in Gulf War veterans to a single specific medical, chemical, or environmental exposure is the association of increased symptom reporting with a number of Gulf War exposures.1,3,6
When considering the impact of these Gulf War exposures and experiences on health, it is important to remember that many studies relied on self-report, for which little, if any, objective documentation was available. Worsening self-perception of health (though not worsening physical health or psychological morbidity) over time in UK Gulf War veterans has been associated with increased reporting of Gulf War exposures.33 The reliability of recall of exposures, assessed using kappa (κ) as a measure of agreement,34,35 has, however, varied for individual exposures. For example, smoke and oil from burning oil wells (SMOIL) was reliably recalled in both UK (κ = 0.79)33 and US (κ = 0.69)36 Gulf War veterans, and being given pyridostigmine bromide tablets was reliably recalled in US Gulf War veterans (κ = 0.86).36 Exposure to depleted uranium was poorly recalled in UK (κ = 0.48)33 and US (κ = 0.07)36 Gulf War veterans. In our study, self-reported exposure to depleted uranium was complemented by an algorithm based on location and activities during the Gulf War, to eliminate implausible exposure and further define the likelihood of possible exposure. In relation to immunisations, Gulf War veterans were asked to refer to their immunisation booklet. Veterans’ uncertainty in relation to their medical exposures could have influenced our results. There are several reasons for this uncertainty, including the time that has elapsed since the Gulf War and poor record keeping at the time of the Gulf War. These aspects of exposure assessment highlights the importance of medical record keeping in the defence forces.
Recall bias may have occurred,37 whereby veterans who report symptoms or medical conditions are also more likely to recall more exposures, particularly those considered potentially harmful, than veterans who do not report adverse health outcomes.38,39 Veterans who recall a specific exposure may also be more likely to associate their symptoms with exposure than those who did not. The effect of perception of vaccination on increased reporting of health outcomes has recently been reported in relation to the anthrax vaccine.40 In determining the year of first diagnosis, the Gulf War group had a well defined reference point, whereas the comparison group did not. Gulf War veterans may be more likely to date the development of any conditions post-Gulf War as this is a very prominent event for them, and this may have led to an overestimation of the association with medical outcomes. Another potential problem is that our analyses involved multiple comparisons and some of the significant associations that we observed could be due to chance alone.
Despite a rigorous and extended contact and recruitment strategy applied to both study groups, the participation rate in our comparison group was lower than that of the Gulf War veteran group. This has been the experience of other research groups.1,4,9,10 The difference in participation rates contributed to some differences in the demographic composition of the two study groups, rendering the results of the study vulnerable to the effects of participation bias. Our formal evaluation of participation bias suggests that our study results may be robust despite some non-participation in the comparison group, and that participation bias is unlikely to explain the differences (or lack of differences) between the two groups in our study.
In conclusion, more than 10 years after the 1991 Gulf War, Australian Gulf War veterans report all symptoms and some medical conditions, including psychological (particularly post-traumatic stress disorder), skin, eye, and sinus conditions more commonly than a comparable group of ADF personnel who were eligible for active duty at the time, but did not go to the Gulf. Increased reporting of symptoms and medical conditions by Gulf War veterans does not appear to be due to over-reporting or participation bias. We have found associations between total number of self-reported symptoms in the past month and several exposures experienced in the Gulf War, including immunisations, prophylactic medications, chemical exposures, and stressful experiences during their deployment. There does not appear to be a unique single exposure associated with increased symptom reporting.
Acknowledgments
This study was funded by the Australian Government–Department of Veterans’ Affairs, and was overseen by a Scientific Advisory Committee and by a Veterans’ Consultative Forum, and we are grateful to members for their contributions and support. We acknowledge the contribution of Health Services Australia who conducted the medical assessments. We wish to thank the international researchers, in particular Professor Simon Wessely and Ms Catherine Unwin of the Gulf War Illness Research Unit, London, UK for their assistance and advice on the development of the study. We wish to thank Dr Keith Horsley, Dr Warren Harrex, Mr Bob Connolly, and his contact and recruitment team at DVA. Finally, and very importantly, we thank the Gulf War veterans and members of the comparison group for the time and effort they made to participate in the study.
REFERENCES
Linked Articles
- Work in brief