Article Text

Abstract
The COVID-19 pandemic has heterogeneously affected use of basic health services worldwide, with disruptions in some countries beginning in the early stages of the emergency in March 2020. These disruptions have occurred on both the supply and demand sides of healthcare, and have often been related to resource shortages to provide care and lower patient turnout associated with mobility restrictions and fear of contracting COVID-19 at facilities. In this paper, we assess the impact of the COVID-19 pandemic on the use of maternal health services using a time series modelling approach developed to monitor health service use during the pandemic using routinely collected health information systems data. We focus on data from 37 non-governmental organisation-supported health facilities in Haiti, Lesotho, Liberia, Malawi, Mexico and Sierra Leone. Overall, our analyses indicate significant declines in first antenatal care visits in Haiti (18% drop) and Sierra Leone (32% drop) and facility-based deliveries in all countries except Malawi from March to December 2020. Different strategies were adopted to maintain continuity of maternal health services, including communication campaigns, continuity of community health worker services, human resource capacity building to ensure compliance with international and national guidelines for front-line health workers, adapting spaces for safe distancing and ensuring the availability of personal protective equipment. We employ a local lens, providing prepandemic context and reporting results and strategies by country, to highlight the importance of developing context-specific interventions to design effective mitigation strategies.
- COVID-19
- maternal health
- health services research
- health systems
- public health
Data availability statement
The data underlying this article will be shared on reasonable request to the corresponding author. We have provided an example dataset with code on our GitHub repository: [https://github.com/isabelfulcher/global_covid19_response].
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Current evidence from low-income and middle-income countries, although limited, indicates declines in facility-based deliveries, and first antenatal care visits were common during the early months of the COVID-19 pandemic.
In this study, we present novel data on maternal health service use from non-governmental organisation-supported health facilities in Haiti, Lesotho, Liberia, Malawi, Mexico and Sierra Leone from March through December 2020, comparing to up to 4 years of prior health service use data.
We observed a significant decline in the use of maternal health services in all countries included in the study except Malawi during the COVID-19 pandemic in 2020.
We discuss these analytical findings in a context-specific manner by focusing on both the national COVID-19 emergency responses of governments and local health measures implemented by the health facilities included in the analysis, which likely impacted maternal health service use in these countries and worldwide.
There is no single way to address the new challenges brought on by the pandemic, so consideration of context-specific factors is key to ensuring effective interventions that mitigate the varied impacts of the pandemic.
Introduction
Disruptions in maternal health services have been of major concern since the COVID-19 pandemic began in early 2020. In a survey conducted by the WHO, 53% of the 105 participating countries reported partial disruptions in antenatal care (ANC) and 32% in facility-based delivery (FBD) services during the first several months of the COVID-19 pandemic.1 Notably, these findings were provided by country informants based on self-assessment, not empirical data. In addition to the decline in the supply of services due to changes in treatment policies and lack of medical equipment, health products and personal protective equipment (PPE) for health workers, many facilities may have experienced a decline in demand, due to lockdowns, financial difficulties and fear of SARS-CoV-2 infection.1 2
Disruptions in service use were hypothesised to disproportionately impact persons living in low-income and middle-income countries (LMICs) due to limited essential health services, which were already difficult for many to access prior to COVID-19.3 Previous studies have documented numerous sociocultural, geographical and economic barriers for women in LMICs to access maternal health services, including lack of transportation, distance to a reliable healthcare facility, limited skilled workers in rural areas and financial barriers.4 During the pandemic, these barriers may be exacerbated for individuals living in LMICs who are more exposed to the economic difficulties associated with the pandemic.5 Further, experts predicted that such disruptions in the use of reproductive, maternal, newborn and child health services could increase under-5 mortality by 9.8%–44.7% and maternal mortality by 8.3%–38.6% per month based on data from previous outbreaks, such as the 2014 Ebola virus epidemic, the 2003 severe acute respiratory syndrome epidemic and the influenza pandemics.6
It is imperative to assess the severity of these disruptions to mitigate the impact on health outcomes as the pandemic continues. However, due to the relatively recent nature of the COVID-19 pandemic and the limited resources allocated to research,7 there are few scientific studies that quantify the impact of this health emergency on the use of maternal health services in LMICs. One of the main shortcomings is the lack of quality data that can be used to develop robust models to identify significant differences in service use before and after the advent of COVID-19.8–10 Expanding the current literature on this subject is key to maintaining maternal health services during future COVID-19 pandemic waves and improving health system preparedness for future infectious disease outbreaks.
In this analysis, we explore the effects of the COVID-19 pandemic on maternal health services at health facilities in six countries representing different regions of the world: Haiti, Lesotho, Liberia, Malawi, Mexico and Sierra Leone (table 1). We use the statistical methods described in Fulcher et al11 (1) to determine expected levels of ANC and FBD based on 4 years of historical data and (2) to estimate the deviation from expected during the COVID-19 pandemic in 2020, including data from March to December 2020 (methods details are described in the Methods section in online supplemental methods). For this analysis, we report on 37 facilities across the six countries; these facilities are supported by the international non-governmental organisation Partners In Health (PIH). We share the strategies employed to prevent and/or mitigate the effects of the pandemic on the supply and demand for maternal health services at the sites in each country (details on how information was collected in the Methods section in online supplemental methods). We apply a local lens, providing prepandemic context and reporting results and strategies by country, to emphasise the diversity of experience and to highlight the importance of developing site-specific and context-specific interventions to address health emergencies.
Supplemental material
Characterisation of participating PIH sites, cumulative predicted counts, cumulative deviation in maternal health service use, date of national lockdowns and strategies implemented by PIH-supported facilities that may have contributed to preventing and/or mitigating the effects of the COVID-19 pandemic on maternal health service use during the COVID-19 pandemic in 2020 (March 2020–December 2020) by country

Time series plots detailing deviations from expected counts (black) during March–December 2020 for first antenatal care visits (histograms on the left) and facility-based deliveries (histograms on the right). Data are from (A) Haiti, (B) Lesotho and (C) Liberia. The grey area indicates the 95% prediction interval. The red asterisk indicates the date on which the first case of COVID-19 was reported in the country (data retrieved from Our World in Data (https://ourworldindata.org/).
Haiti
PIH–Haiti, known locally as Zanmi Lasante (ZL), launched in 1990 the first women’s health programme in the Central Plateau region, called Sante Fanm, which includes antenatal, delivery and postnatal care among its services. In July 2018, ZL implemented the ‘Journey to 9 Plus’ group antenatal and neonatal care programme at one facility, achieving a 91% (77%–97%) ANC adherence rate and 96% FBD rate.
Maternal health use exhibited some seasonality over the past 5 years (figure 1A). Throughout this period, there have been recurrent declines in ANC visits each fall. These are mostly related to public protests and riots resulting from social unrest, often ending in local or national lockdowns that prevented women from attending their ANC appointments. In the past years, some of the most disrupting episodes took place in November 2016,12 September 2017,13 November 201814 and October 2019, which included a 3-month nationwide lockdown.15 FBDs appear to be less affected by events related to social unrest than ANC visits. Nevertheless, an increase in this number is observed each fall, likely associated with an increase in conception during Christmas and New Year holidays as well as Carnival in February.16

Time series plots detailing the observed (black) and predicted counts (grey) from 2016 to 2020 for first antenatal care visits (histograms on the left) and facility-based deliveries (histograms on the right). Data are from (A) Haiti, (B) Lesotho and (C) Liberia. The grey area indicates the 95% prediction interval. The red asterisk indicates the date on which the first case of COVID-19 was reported in the country (data retrieved from Our World in Data (https://ourworldindata.org/).
Outside of the aforementioned singularities, maternal health service use from March to December 2020 was lower than expected for both first ANC visits (18% significantly lower than expected) and FBD (17% significantly lower than expected) (table 1). Significant declines occurred from April to June 2020 and again in December 2020 for first ANC visits; declines were similarly observed from April to August 2020 for FBDs (figures 1A and 2A). This was likely due to the full lockdown initiated in mid-March 2020 by the national government in response to the rapid spread of the disease in other countries (table 1),17 as well as fear of COVID-19 infection in facilities treating patients with COVID-19, which may have reduced the number of women attending their ANC appointments and delivery at health facilities. In order to ensure minimal disruptions in the provision of maternal health services, ZL, in collaboration with the Haitian Ministry of Health (MoH), adapted spaces to ensure safe distancing between patients in the prenatal waiting area, as well as encouraging women to come to the Mirebalais University Hospital for delivery.
Lesotho
PIH began working in Lesotho by invitation of the MoH to support the national response to the HIV epidemic. HIV care and treatment were integrated into general primary health services including maternal healthcare (ANC, delivery and postnatal care) in the rural highlands. In 2014, Lesotho launched a national health reform with support of PIH. Facility-based maternal health services were complemented by a village health worker (VHW) programme, which focuses on training local VHWs to accompany women in the community through all stages of pregnancy. Since PIH began working in Lesotho, ANC visits have increased by 85% at PIH-supported facilities, and FBDs have experienced a 15-fold increase.18
Lesotho was the last country in reporting the first COVID-19 case in Africa (figures 1B and 2B).19 However, an alarming number of COVID-19 cases were detected after the influx of people travelling from South Africa for Christmas vacation.20 From March to December 2020, PIH-supported facilities in Lesotho did not experience significant declines in the number of first ANC visits (table 1). The number of FBDs was 12% lower than expected over the entire period due to the slightly lower than expected number of FBDs in April–October (figures 1B, 2B).
Regardless of the contained burden of the pandemic in the region, several measures to ensure routine maternal health service use were adopted. The VHW programme was strengthened by leading trainings on COVID-19 signs and symptoms, infection prevention and control, providing PPE and offering VHWs regular mentorship on screening and patient follow-up. Health facilities adopted international standards for maternal care during the pandemic, screening all patients, staff and clients before entering the facilities, adapting spaces to ensure a safe distance between patients and limit the risk of contagion, and testing everybody with COVID-19 symptoms.
Liberia
During the Ebola outbreak in 2014, the Liberian government requested PIH’s assistance in the southeast region of the country. PIH–Liberia focused its strategy on infectious disease control and strengthening the local health system, renovating some primary care clinics and hospitals in the region. Efforts to improve maternal and neonatal health focused on improved access to services such as ANC, skilled birth attendance, emergency obstetric and neonatal care, postnatal care, and comprehensive maternal and newborn immunisation services. In 2019, PIH–Liberia supported the government in introducing the community health promoter (CHP) programme, which included CHPs who serve as a link between health facilities and pregnant and postpartum women and their newborns.
In Liberia, the advent of COVID-19 was accompanied by misinformation campaigns about the disease, which spread disbelief about its potential severity and mistrust in the management of the pandemic by health authorities among the population.21 Mistrust in public health institutions may have negatively affected the demand for maternal health services, as opposed to the increased demand for services linked to the increase in teenage pregnancies, likely due to the reduced availability of family planning methods in the early months of the pandemic and school closures.
In this context, PIH–Liberia placed special emphasis on increasing public awareness about the new disease and the availability of services supported by the organisation. In addition, PIH–Liberia, in collaboration with Liberian public health institutions, built service providers’ capacity for compliance with maternal and neonatal care standards during the outbreak and ensured sufficient availability of essential medical supplies by anticipating the worst-case scenario of pandemic evolution. PIH-supported facilities experienced no significant disruptions in first ANC visits, while the number of FBDs was 21% lower than expected from March to December 2020 (table 1). Looking at monthly data, we found that first ANC visits experienced a decline in April 2020, whereas FBDs recorded significant declines in April, May, and July 2020 and remained lower than expected until December 2020 (figure 2C). However, reductions in maternal health service use may not be entirely attributable to the pandemic, as some declines were observed already during 2019 (figure 1C).
Malawi
PIH initially began working in Malawi to support the MoH in reducing the high burden of HIV and tuberculosis in Neno District. Since then, PIH–Malawi, locally known as Abwenzi Pa Za Umoyo (APZU), has built two hospitals in partnership with the government, revitalised other health facilities and introduced a CHW programme. Part of APZU’s mission is providing integrated maternal care to the women in Neno district, including antenatal, delivery and postnatal care. This is reinforced by the CHW programme that helps link pregnant women from their households to health facilities.22
In April 2020, the Malawi government announced plans to impose a national lockdown; however, the lockdown was cancelled on appeal to the country’s highest court with concern for limitations of human rights and lack of social support.23 The lack of nationally imposed restrictive measures likely facilitated maintained access to health services compared with other countries. The MoH developed guidelines for the care of women in the antenatal, delivery and postnatal periods in the face of COVID-19, which provided health workers with a clear pathway on best practices on the safe management of pregnant women and their babies during the pandemic. In addition, the government embarked on the emergency hiring of additional health workers.24
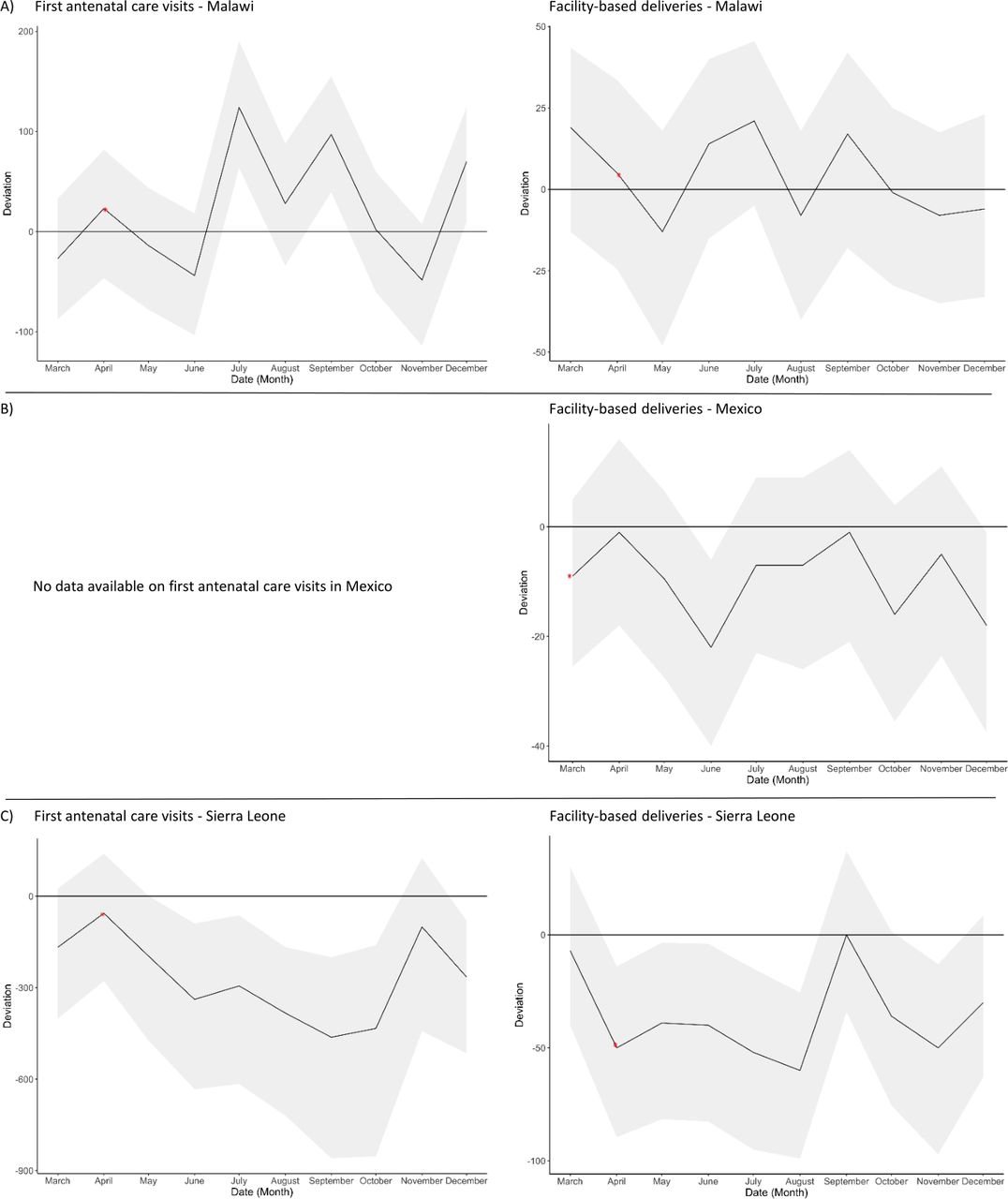
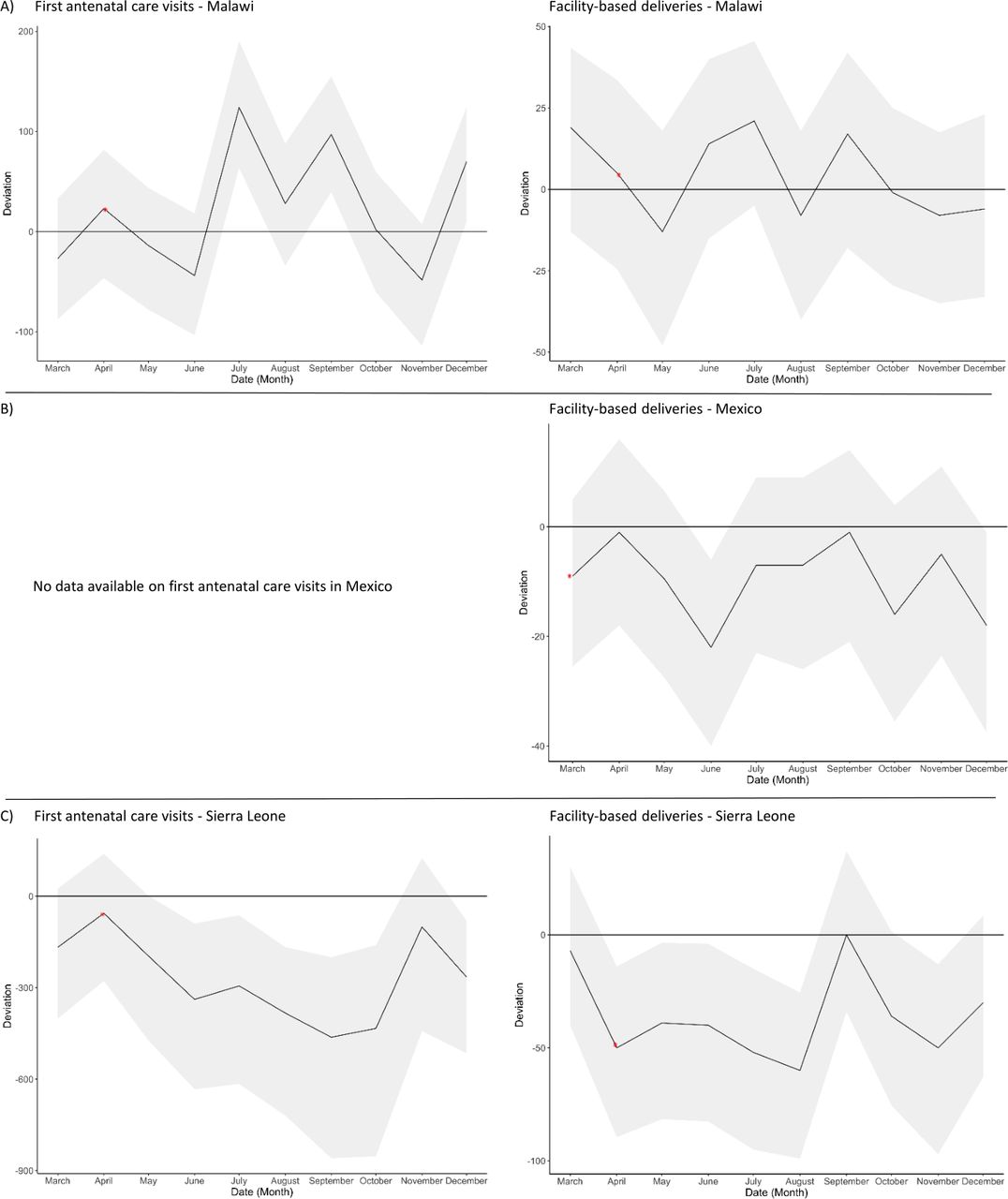
As shown in figures 3A and 4A, maternity care service use in APZU-supported facilities did not suffer any significant monthly declines after March 2020. It even experienced significant increases for first ANC visits in the months of July, September and December 2020. Looking at the entire study period, there were no significant variations in maternity care service use during the COVID-19 pandemic in 2020 (table 1). This is likely a result of the absence of a national lockdown coupled with the fact that maternal health services and CHW support were never suspended in Neno District; in addition, outreach visits to communities were intensified to deliver perinatal services during the pandemic. From the demand side, the APZU team developed a communication plan to provide reassurance about the safety of care-seeking and to dispel the fear of getting infected in health facilities.
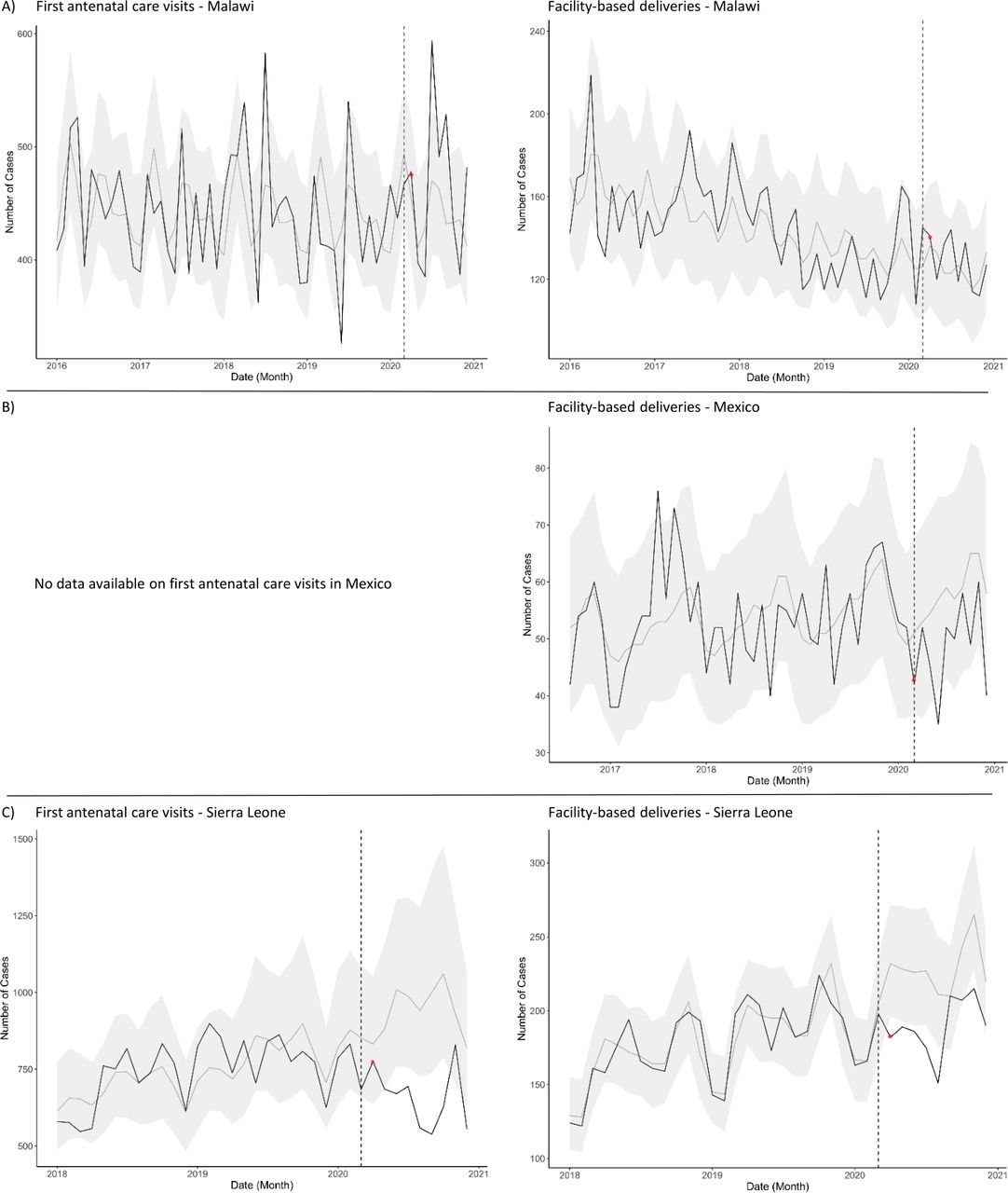
Time series plots detailing the observed (black) and predicted counts (grey) from 2016 to 2020 for first antenatal care visits (histograms on the left) and facility-based deliveries (histograms on the right). Data are from (A) Malawi, (B) Mexico and (C) Sierra Leone. The grey area indicates the 95% prediction interval. The red asterisk indicates the date on which the first case of COVID-19 was reported in the country (data retrieved from Our World in Data (https://ourworldindata.org/).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time series plots detailing deviations from expected counts (black) during March–December 2020 for first antenatal care visits (histograms on the left) and facility-based deliveries (histograms on the right). Data are from (A) Malawi, (B) Mexico and (C) Sierra Leone. The grey area indicates the 95% prediction interval. The red asterisk indicates the date on which the first case of COVID-19 was reported in the country (data retrieved from Our World in Data (https://ourworldindata.org/).
Mexico
PIH–Mexico, Compañeros En Salud (CES), works in nine rural communities and a town called Ángel Albino Corzo (AAC) in the Fraylesca and Sierra regions of the Mexican state of Chiapas. Maternal health services are provided through antenatal and postpartum care at primary care clinics and delivery care provided in a birthing centre and in the adjacent basic community hospital in AAC. This is complemented by work in rural communities led by CHWs, who promote adherence to ANC and facility delivery. The CES obstetric nursing team at the birthing centre hosted a weekly slot on the local radio before the pandemic to discuss the patient-centred delivery model provided at the facility.
After the COVID-19 pandemic was officially declared a national emergency by the government on March 2020,25 fear and uncertainty spread throughout the areas served by CES. The radio slot was cancelled; CHWs spaced out visits to pregnant women; and the basic community hospital of AAC stopped attending deliveries to prevent pregnant women from getting COVID-19. The birthing centre was the only public facility attending deliveries in the entire AAC municipality, which led to the care of some patients in a labour room set-up in the adjacent waiting home to avoid overcrowding at the birthing centre.
The major disruption in maternity service use coincided with a local burden of COVID-19 cases in June 2020, with a significant decline in the number of deliveries at public AAC facilities. Another significant decline was observed in December 2020 (figures 3B, 4B). Overall, the number of FBDs was significantly lower than expected by 16% from March to December 2020 (table 1). Although mobility restrictions at the national and state levels were moderate, some rural communities prohibited people from leaving and entering, making it difficult for women to access the birthing centre to give birth. In addition, fear and uncertainty may have led women to seek other options for delivery care. This is consistent with some reports indicating an increase in home births supported by traditional midwives during the pandemic in Chiapas.26 However, after the first months of the pandemic, fear began to dissipate as women who had experienced a safe delivery at the birthing centre shared their positive experiences with other women, potentially resulting in a gradual increase of pregnant women coming to the facility for delivery.
Sierra Leone
Since PIH began working in Sierra Leone, after the organisation was invited by the Ministry of Health and Sanitation (MoHS) to join forces against the Ebola outbreak, the organisation has expanded across three districts, offering maternal health services including antenatal, delivery and postpartum care, which are reinforced by CHW-led work at the community level.
The strong preparedness and response measures to the COVID-19 pandemic implemented by the government of Sierra Leone could have had an impact on the country’s figures: 6347 confirmed cases and 121 deaths as of 20 August 2021 (table 1).27 However, the restrictions in the early stages of the pandemic also affected care use. From March to December 2020, the number of first ANC visits was significantly lower than expected by 32%, while the number of FBDs was significantly lower than expected by 16% (table 1). Looking at the data at the monthly level, we found that significant declines in first ANC visits were from June to October 2020, inclusive, and were experienced again in December 2020. As for FBDs, significant declines began in April and continued through August 2020, inclusive, and occurred again in November 2020 (figures 3C, 4C).
To mitigate the impact of the pandemic on maternal health use, PIH–Sierra Leone, in collaboration with the MoHS, developed strategies that focused primarily on on-site preparedness to prevent local outbreaks, ensuring continuity of health services. Health workers were trained to align their practices with the latest recommendations on maternal healthcare delivery issued by international bodies and the national government. Following these recommendations, patient flows were optimised and bed arrangements in hospital wards were improved to limit patient-to-patient contact. To ensure safe use of health facilities, CHWs raised community awareness of the importance of keeping safe distance and good hand hygiene. In addition, a communication plan was put in place to counteract misinformation campaigns, dispelling women’s fear of becoming infected at health facilities.
Conclusion
Despite differences in context among PIH-supported sites, all countries shared the need to adapt to the new challenges brought on by the COVID-19 pandemic. Creativity in designing context-specific responses has been especially important in resource-constrained settings whose fragile health systems, with medical infrastructure, material supply, and human resources shortages have been challenged by the additional demands resulting from the health emergency.28
We found some commonalities among the strategies followed by PIH-supported sites (table 1). Communication campaigns have been used as a means to maintain the use of health services. This strategy has been specially relevant in Malawi, Liberia and Sierra Leone, which have been particularly affected by the COVID-19 infodemic, as have other countries in the African continent.22 29 In all sites, CHWs, who have maintained their routine activities, helped dispel fear among the women by communicating the preventive measures taken by the health facilities to ensure safe ANC visits and delivery care.
On the supply side, building the capacity of healthcare providers to deliver maternal healthcare during the pandemic has been essential to ensure patient and provider safety and to gain women’s trust. Most facilities began applying guidelines from global reference health agencies, such as the WHO and the Centers for Disease Control and Prevention, and implemented national recommendations when available.30 31 In addition, PIH created cross-site expert working groups that established updated recommendations for front-line workers with the latest evidence. To conform to the recommendations, sites adapted spaces to ensure safe distancing between patients and ensured sufficient stock of PPE and sanitation kits in all facilities. In some countries with good telecommunications infrastructure, such as the USA, remote ANC has been widely implemented as a solution to reduce potential exposure to COVID-19 by providers and patients.32 33 Nevertheless, telephone and internet connectivity issues in most of the communities served by PIH have made the implementation of this intervention infeasible in our settings.
All of these strategies, along with years of collaborative capacity building between PIH and local MoHs, likely contributed to buffering the effects of the COVID-19 pandemic on maternal health service use on both the supply and demand sides. Looking at monthly data, declines in maternal health service use were either not significant or mitigated and returned to expected values by August 2020 in half of the countries in the study.
Our findings complement previous studies of maternal health service use during the pandemic conducted in LMICs. In Asia, studies in Bangladesh, China, India and Nepal reported a decline in the number of women delivering in facilities and disruptions in ANC attributable to the pandemic.8 34–36 In Africa, research conducted in Cameroon, Ethiopia, Liberia, Mali, Malawi, Nigeria, Rwanda, Sierra Leone, Somalia, South Africa and Uganda reported decreases in ANC visits and/or FBDs during the pandemic,8 10 37–41 whereas research conducted in the Democratic Republic of the Congo showed no declines in ANC visits nor FBDs during the first wave of COVID-19.42 The reductions in first ANC visits and FBDs in Sierra Leone and Liberia reported in other studies are consistent with our findings. However, contrary to our results, Saphira and colleagues found decreases for these two indicators in Malawi at the national level.10 As mentioned previously, this may be related to the additional resources that the facilities included in our study have, in the form of training and supplies received from PIH, which may have helped mitigate the effects of the pandemic on maternal health service use locally and may have led to different outcomes from those of other public health facilities or private for-profit facilities in the country. Thus, it is imperative to investigate changes at both the national and local levels during emergencies, such as the COVID-19 pandemic, as these can often tell different stories.
Our analysis sheds light on the impacts of the COVID-19 pandemic on maternal health service use in LMICs and the mitigation strategies put in place to counteract these effects. We hope that the lessons learned from PIH project sites will assist other teams working in LMICs in developing local context-specific solutions to the challenges brought by the pandemic.
Data availability statement
The data underlying this article will be shared on reasonable request to the corresponding author. We have provided an example dataset with code on our GitHub repository: [https://github.com/isabelfulcher/global_covid19_response].
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @KarenGrepin, @myclaw, @jcmugunga, @BHedtGauthier
Collaborators The Cross-site COVID-19 Syndromic Surveillance Working Group is composed of the following—Partners In Health (PIH)/Boston: Jean-Claude Mugunga; PIH/Haiti: Peterson Abnis I Faure, Wesler Lambert, Jeune Marc Antoine; PIH/Liberia: Emma Jean Boley, Prince F Varney; PIH/Lesotho: Meba Msuya, Melino Ndayizigiye; PIH/Malawi: Moses Aron, Emilia Connolly; PIH/Mexico: Zeus Aranda, Daniel Bernal; PIH/Rwanda: Vincent K Cubaka, Nadine Karema, Fredrick Kateera; PIH/Sierra Leone: Thierry Binde, Chiyembekezo Kachimanga; Harvard Medical School: Dale A Barnhart, Isabel R Fulcher, Bethany Hedt-Gauthier, Megan Murray; Hong Kong University: Karen A Grépin; University of British Columbia: Michael Law.
Contributors ZA is the first author of the manuscript and has worked on the conceptualisation of the manuscript, literature search and all stages of writing. TB is the second author and has participated in the drafting of the original version of the manuscript. KT has performed data cleaning and analysis. AT has participated in writing the original draft and editing the final version of the text. BM, DM, EJB, IM, ID, MM, MC, MGM, MN, MCJ-B, PFV, SA, KAG, MRL, JCM and BH-G have reviewed the original text and edited the final version of the manuscript. IRF actively participated in the conceptualisation of the manuscript, led statistical methods development and oversaw the development of the manuscript. All authors, including the Cross-site COVID-19 Syndromic Surveillance Working Group, discussed the results and provided comments on the manuscript.
Funding This work was supported by a grant from the Canadian Institutes of Health Research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.