Article Text

Abstract
Alcohol-related harm has gained increased attention in high-income countries (HICs) in recent years which, alongside government regulation, has effected a reduction in alcohol consumption. The alcohol industry has turned its attention to low-income and middle-income country (LMIC) markets as a new source of growth and profit, prompting increased consumption in LMICS. Alcohol use in LMICs is also increasing. There is a need to understand particularly in LMICs the impact of industry strategy in shaping local contexts of alcohol use. We draw on conceptualisations from food systems research, and research on the commercial determinants of health, to develop a new approach for framing alcohol research and discuss implications for alcohol research, particularly in LMICs, focusing on South Africa as an illustrative example. We propose a conceptualisation of the ‘alcohol environment’ as the system of alcohol provision, acquisition and consumption—including, critically, industry advertising and marketing—along with the political, economic and regulatory context of the alcohol industry that mediates people’s alcohol drinking patterns and behaviours. While each country and region is different in terms of its context of alcohol use, we contrast several broadly distinct features of alcohol environments in LMICs and HICs. Improving understanding of the full spectrum of influences on drinking behaviour, particularly in LMICs, is vital to inform the design of interventions and policies to facilitate healthier environments and reduce the harms associated with alcohol consumption. Our framework for undertaking alcohol research may be used to structure mixed methods empirical research examining the role of the alcohol environment particularly in LMICs.
- health policy
- health systems
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
In recent years, alcohol consumption has reduced in high-income countries.
The alcohol industry has turned its attention to low-income and middle-income countries.
Critical need to understand how the alcohol industry shapes local alcohol use.
We propose a conceptualisation of the ‘alcohol environment’ to help do this.
Our conceptualisation includes alcohol provision, acquisition and consumption.
This, critically, includes advertising and marketing activities.
The conceptualisation also includes political, economic and regulatory context of alcohol industry.
This new conceptualisation provides an approach for framing alcohol research.
Research of alcohol environments is vital to inform effective regulation.
Introduction
Hazardous alcohol use is a major public health concern worldwide, increasing risk of many non-communicable diseases, infectious diseases, mental health problems and harm from external causes such as injuries and violence.1 This alcohol-related harm has gained increased attention in recent years, evidenced by a focus on addressing alcohol consumption in the Sustainable Development Goals.2 The increasing recognition and associated government regulation of the alcohol industry has been accompanied by reductions in alcohol consumption in high-income countries (HICs).1 The industry has responded by developing new sources of growth and profit, particularly in low-income and middle-income countries (LMICs),3 and expansion into Africa is an explicit part of the industry’s growth strategy.4 Relatedly, alcohol use has been shown to be on the rise in many LMICs.1
South Africa is a particular target of alcohol industry efforts to develop new markets in Africa. Its large population, low rates of drinking among some population groups and connectedness globally and regionally makes it an attractive base from which to expand into other parts of Africa.5 Overall consumption of alcohol in South Africa is high, despite current drinkers being in the minority. This is due to drinkers’ propensity to engage in heavy episodic drinking, which increases sales and profitability. Industry marketing has focused on encouraging uptake of drinking among women, who generally have low drinking rates in Africa currently,6 and young adults, in the hope that they will adopt heavy drinking patterns. This targeting is done in various ways, for example, through development of flavoured products thought to be favoured by women, such as alcopops, and through marketing that promotes an association between alcohol and women’s independence.6
Evidence of alcohol’s health impact in LMICs is emerging, with alcohol consumption a leading health risk factor in Southern Africa, as demonstrated in the Global Burden of Disease Study.3 In South Africa, 7% of disability-adjusted life years are attributable to alcohol.7 However, South Africa’s harmful alcohol use has socioeconomic dimensions; high-income earners have the highest drinking prevalence, but low-income earners on average consume more alcohol, spend a greater proportion of household income on alcohol and experience a higher burden of alcohol-related harm.8 9
Higher rates of alcohol-related illness, injury and mortality among the poor in South Africa8 are compounded by the inequalities in the health and social systems—a legacy of the country’s history of colonial subjugation, apartheid dispossession and prevailing dysfunction of the postapartheid period.8 Related to this are the deep roots that harmful alcohol use has in political systems of control under apartheid. The ‘dop’ system was a practice which, despite being officially illegal, saw farm workers given alcohol as a benefit of employment.10 With the rise of the gold mining industry in Southern Africa, the availability of cheap alcohol to workers on the mines helped to facilitate retention and stability of a migrant work force. However, by the turn of the century, mining’s requirement for consistent worker productivity was threatened by uncontrolled alcohol distribution to and consumption by workers. As a result, mining interests sought to establish better control over merchant retailing of alcohol to workers or to support total prohibition of the supply of alcohol to African workers. In contrast, agricultural employers in Western Cape Province continued to use alcohol as a useful medium of renumeration of workers.10
The result is widespread alcohol-related harm. Alcohol is a key risk factor for South Africa’s exceptionally high levels of interpersonal violence and disease. Studies have also found that large proportions of pregnant women report drinking alcohol during pregnancy, corresponding with South Africa having the highest rates of fetal alcohol syndrome globally.11 Importantly, the health impacts of hazardous alcohol use may differ in LMICs from HICs, due to interaction with other risk factors; for example, alcohol use is associated with higher risk of infectious disease, including HIV infection and tuberculosis,12 of particular relevance in countries with a high burden of these diseases.
A substantial body of evidence has documented the environments in which people live with regard to the factors shaping alcohol acquisition and consumption. However, this work has often focused on alcohol outlet density13 or cost (eg, minimum unit pricing and taxation)14 and has mostly been conducted in HICs, despite the context of alcohol acquisition and consumption, including advertising and marketing strategies, differing significantly in LMICs. The alcohol industry is a key determinant of alcohol consumption and related harms in LMICs too and requires careful monitoring and effective regulation.15 However, there is also a need to understand the impact of industry strategy in shaping local contexts in which alcohol is used and interactions with broader relevant sociocultural factors. Analyses of industry strategy, as have also been advocated for and conducted in other areas of health including regarding tobacco and ultraprocessed food and beverages, can particularly assist with informing the development of effective public health advocacy and regulation.16–18 While the difficulty of attributing policy change to any particular analysis has long been noted,19 the evolution of tobacco control policy could be cited as policy change resulting to a significant extent from the large body of work analysing industry impact and strategy.20 21
In this paper, we draw on theories and conceptualisations from food systems research to propose a conceptualisation of what we term the ‘alcohol environment’. We then discuss the implications of the alcohol environment conceptualisation for alcohol research in LMICs, with a particular focus on South Africa as an illustrative example. We recognise the heterogeneity of contexts of LMICs, and thus while the themes emerging from South Africa are indicative, there is a need to replicate this analysis in other LMIC settings. Such research is critical to identify points of intervention and to inform the development of effective regulation.
Conceptualising the ‘alcohol environment’
Our conceptualisation of the ‘alcohol environment’ builds on research into the food environment, which is informed by socioecological theories of inter-related personal and environmental factors shaping health-related behaviours such as food (or alcohol) consumption.22 A recent conceptualisation by Turner et al22 describes the food environment as ‘the interface where people interact with the wider food system to acquire and consume foods’. The concept of an ‘interface’ and the focus on ‘interactions’ helps to relate the food environment construct to food systems more broadly, as well as to people’s daily lives and the activities that shape diets. However, our conceptualisation of ‘environment’ is different to that of the food environment: broader and encompassing a greater number of domains.
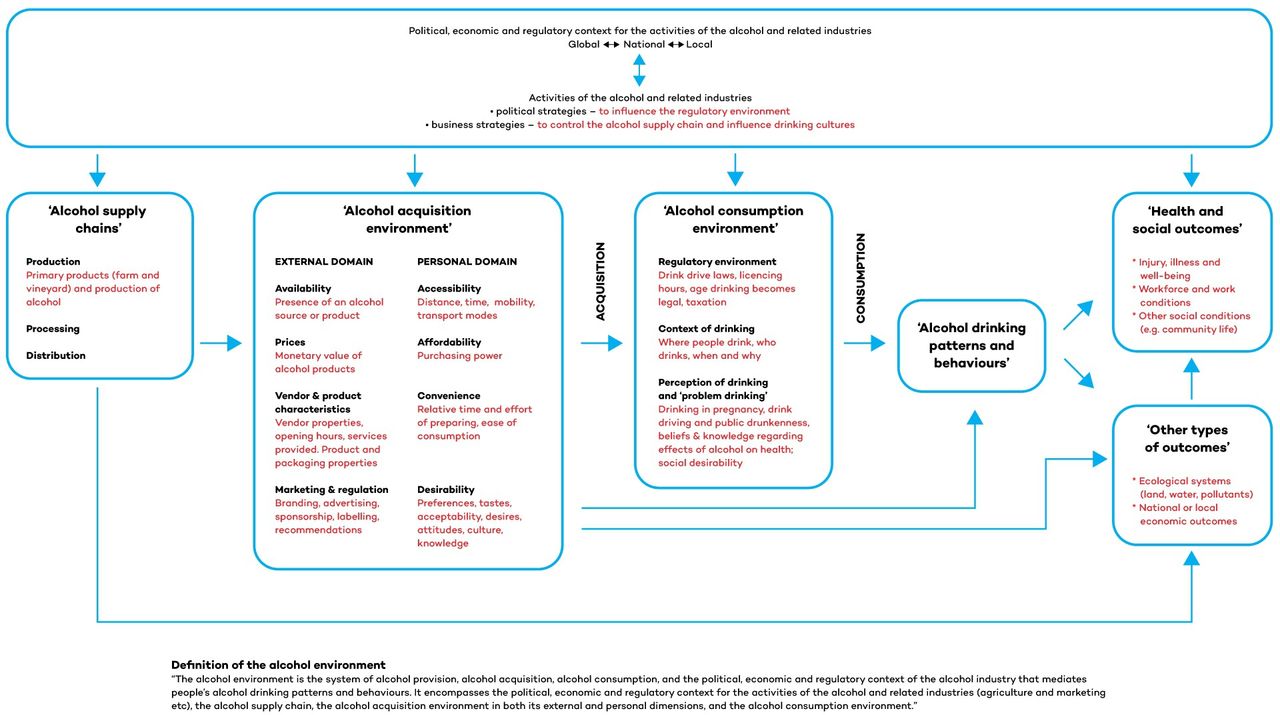
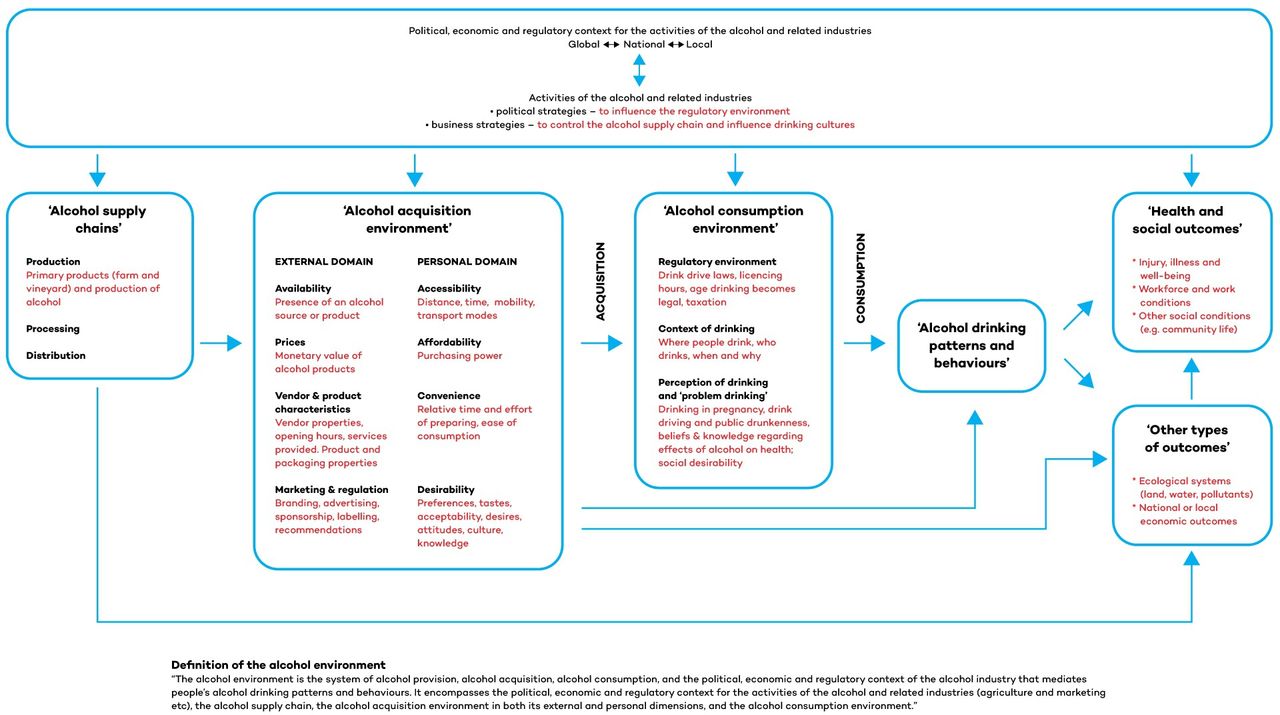
Alcohol, as a consumable marketable product, has similarities to food but also unique characteristics that require its consideration as a separate entity.23 In the framework we develop in this paper of alcohol environments, we describe key features that distinguish between the ‘alcohol acquisition’ and ‘alcohol consumption’ environments (drawing on the Turner et al conceptualisation). However, the alcohol industry includes some of the largest transnational corporations, whose actions strongly shape alcohol drinking patterns and behaviours and have clear detrimental health impacts. We therefore extend the food environment framework to examine the products and the structure and inter-related political and business practices of the industry, borrowing from the Corporate Health Impact Assessment framework.24 Additional contextual factors that may moderate these pathways include impacts on the workforce, working conditions and environment which, in turn, shape non-communicable disease, infectious disease and injury risks. By merging these two prior frameworks, we seek to describe the context for alcohol-related health harms and to characterise the pathways by which such impacts occur. Figure 1 describes our proposed framework and definition of the alcohol environment.
{kind=link}
Conceptual framework and definition of the alcohol environment and its wider influences.
The domain titled ‘political, economic and regulatory context for the activities of the alcohol and related industries’ covers global, national and regional levels and encompasses the political and business strategies of the alcohol industry and related industries. These industries use political strategies to influence decision makers so as to achieve favourable regulatory outcomes and develop business models to control supply chains and influence drinking cultures.21
We define the ‘alcohol acquisition environment’ as the interface where people interact to acquire alcohol, which fits between the broader system of alcohol provision (defined here as the ‘alcohol supply chain’ and comprising of production, processing and distribution), the political, economic and regulatory context of the alcohol industry and alcohol consumption. The external domain of the alcohol acquisition environment relates to the environmental opportunities and constraints related to dimensions such as alcohol availability, prices, vendor and product properties, and marketing and advertising of products, including as this relates to levels of illicit alcohol production. The personal domain of the alcohol acquisition environment includes individual-level dimensions: accessibility, affordability, convenience and desirability. The alcohol acquisition environment includes three sources: (1) market-based alcohol sources (both legal and illicitly produced); (2) own production; and (3) transfers (including payment in alcohol and gifts). Industrially produced alcohol available predominantly through market-based sources is the most significant alcohol source in most countries, including in LMICs, but non-market-based sources also contribute to alcohol environments, particularly in LMICs.
We define the ‘alcohol consumption environment’ as the interface where people interact to consume alcohol, located between the alcohol acquisition environment and alcohol drinking patterns and behaviours. It encompasses both regulations shaping alcohol consumption (eg, in regard to advertising and marketing, drink driving laws, licencing hours, minimum drinking age and the cost of alcohol relative to income, which is partly related to taxation) and the context in which people drink (who drinks, when, where and why). Some subgroups can be at greater risk of unhealthy alcohol consumption, for example, by gender, age, occupational group or geographical location. It also includes people’s attitudes to drinking and perceptions of ‘problem drinking’ (including in regard to drinking in pregnancy, drink driving and public drunkenness) and health beliefs and knowledge of alcohol’s health effects.
The complex and dynamic interactions between the alcohol environment domains shape people’s drinking patterns and behaviours, and ultimately, health and social outcomes, as well as related ecological and economic outcomes. This framework has the potential to support researchers, policymakers and practitioners to identify points for intervention to influence the alcohol environment. It can also help with identifying possible multiple effects of interventions. For example, community mobilisation on alcohol may change perceptions of drinking and may also change opening hours (vendor characteristics), independent of any regulatory change.
Key differences in alcohol environments of HICs and LMICs, with South Africa as an illustrative case
While recognising heterogeneity of the contexts of LMICs, in general, alcohol environments in LMICs are considerably more variable than in HICs, with alcohol also more likely to be informally produced and traded.25 The relationships between large industrial producers and smaller traders can be highly variable, with distribution of formally produced alcohol taking place alongside distribution of unrecorded alcohol through informal unregistered vendors. In fact, informal trade in alcohol has strategic value to formalised trade and the alcohol industry, through the role it plays in normalising a culture of drinking, creating addiction and entrenching barriers to entry.26 A report prepared for the South African Department of Trade and Industry comments that ‘whilst South African Breweries (SAB) indicates that over 70% of its beer is distributed to the licensed retail market, it is estimated that as much as 70% to 80% of SAB products are actually consumed in the informal and unlicensed market’.27 While the alcohol industry in some settings frames informally produced alcohol as highly problematic, particularly if the price of industrially produced alcohol through formal channels is increased, in reality alcohol prices are already very low in many settings through bypassing official retail channels. In some LMICs, with Russia a documented example here, non-beverage or surrogate alcohol consumption—from substances not sold for drinking such as perfumes or some medicines—is a substantial issue.28 These products are often cheaper and substantially stronger than legal beverages.
Alcohol is often relatively more affordable in LMICs than HICs. This is due to lower taxation rates applied and also in places such as South Africa with wholesalers offering volume-based discounts to incentivise purchase from informal traders, who then sell to consumers at just above wholesale prices. Payment for work in alcohol, rather than cash, has been documented in Russia29 and South Africa with the dop system.10 While this latter practice, now officially prohibited, has declined dramatically, its legacy lives on in the country’s high levels of alcohol dependence and a ‘culture’ of drinking.
The limited research undertaken in the area suggests that the contexts in which people drink—including who drinks, where, when and why—also differ markedly between HIC and LMICs,30 as do perceptions of drinking and ‘problem drinking’.31 In many HICs, the gender gap in alcohol consumption has lessened over time, while in many LMICs, women drink considerably less than men. These contexts in which people drink are also frequently themselves shaped by industry interests. Mager et al32 has described the way that the alcohol industry in South Africa has exploited masculinity and nationalism to develop a culture in which, for example, alcohol consumption is synonymous with what it means to be a man.
Alcohol production in both HICs and LMICs is dominated by transnational corporations, which in low-income contexts subsume local alcohol producers as they expand. Traditional and home-made alcohol production often operates alongside industrially produced alcohol in LMICs. In both HIC and LMIC settings, there are high levels of industry market concentration; however, in LMICS, there are many different distribution channels (fewer and more restricted in HICs), and industry also engages with informal vendors with selling their products. In South Africa, an estimated 14% of alcohol is illicit in some or another, typically either by evading excise duties or by being produced for sale by an unlicensed brewer.27 Truen et al describe how in South Africa, SAB has passed legal liability to a distribution network of licenced distributors and retailers to service the informal sector on their behalf. This distribution tier is not policed, and the brewery is not compelled to reduce or stop servicing this distribution tier.27
These figures from South Africa of alcohol consumption related to alcohol type are in fact not so different from the situation in many countries globally.33 However, it is worth noting that national figures, based on averages, can obscure considerable differences by region and population demographics. This is particularly so in countries with a high prevalence of abstinence from drinking but high levels of binge drinking among those who drink. Relatedly, in countries where drinking is very uncommon in women, the statistics based on averages thus underestimate drinking among men.
There are also stronger regulatory environments for alcohol in HICs than in LMICs—in terms of both presence and enforcement of regulation. Such regulation may cover, for example, taxation of alcohol products (generally higher in HICs, resulting in relatively high prices of alcohol), labelling in regard to alcohol units, age restrictions on drinking and laws regarding drinking and driving.34 However, particularly in low-income settings, and as observed in South Africa, regulatory environments can be applied and interpreted differently by different stakeholder agencies—for example, by industry, traders and enforcement agencies—and what happens on the ground may not reflect the regulatory environment intended by policymakers. Furthermore, policymakers are often (perhaps more so than in HICs) co-opted onto the board of major players in the alcohol sector. In South Africa, the intended effects of pricing interventions through tax and excise tax can be nullified if supply chains are circumvented, with unlicenced retail. Regulation can also be strongly influenced by the goal of maximising alcohol-industry contribution to the economy, rather than on the social, health and economic costs of alcohol use.35
Thus, while increased international trade, foreign direct investment and supermarketisation may be considered ‘homogenising’ influences of the alcohol environments of HICs and LMICs, there are fundamental differences as summarised in table 1. These differences illustrate the more complex, often informal and less regulated alcohol environments that often characterise LMICs compared with HICs.
Characterising the alcohol environments of HICs and LMICs: similarities and differences
Implications for alcohol research in LMICs
Alcohol environments in LMICs present various particular challenges to empirical research as described below.
Dynamic and complex nature of alcohol environments in LMICs compared with HICs
The dynamic and complex nature of alcohol environments in LMICs raise particular issues for research. Methods and metrics in alcohol research have largely been designed to capture the relatively stable, formalised and well-documented alcohol environments of HICs. Alcohol environment research in HICs has focused almost exclusively on market-based sources, but studies in LMICs must consider a more diverse range of alcohol sources and associated advertising and marketing strategies, including coexistence of formal and informal sources of alcohol, as well as non-market-based alcohol sources such as own production, and gifts, and payment in alcohol such as with South Africa’s dop system.
Governance arrangements, including the rules and processes that determine authority, accountability and community participation in decision making, can also differ in LMICs —with of course great heterogeneity within LMIC contexts too. As Rendall-Mkosi and Diederiks36 state in a report describing community-implemented actions to reduce alcohol harm, with examples from India and South Africa, alcohol control policies are usually introduced at a country or provincial level but can also be introduced at a local level, through municipalities or informal policies via community structures, for example, street committees. Assessing such governance arrangements, including at a community level, relates to areas of the framework that represent the political, economic and regulatory context for the activities of the alcohol and related industries at global, national as well as local levels and also to the ‘alcohol consumption environment’ domain including regulatory aspects.
Characteristics of the ‘personal’ domains of the alcohol acquisition environment also differ in LMICs than in HICs, with alcohol generally cheaper and more accessible in LMICs, for example. There are also markedly different alcohol consumption environments and contexts for drinking. While there is some research in this area on alcohol, particularly for HICs, given the parallels with food and tobacco research to understanding alcohol,37–39 investigation of the alcohol environment in LMICs can draw on qualitative research from tobacco and the burgeoning qualitative research of food environments and associated policy processes.40–42
Lack of data and poor policy transparency
LMICs are also more likely than HICs to lack quality data on the various dimensions of alcohol environments. Detailed datasets containing geotagged information about vendors are likely to be limited or non-existent. Similarly, policy information and documentation (eg, regulations regarding product labelling) may not be as readily available in LMICs, given differences in accessibility of government documentation and differences in multinational company operating practice between jurisdictions. Thus, while there is a need for more research on alcohol environments in LMICs, methods and metrics used to understand alcohol environments in HICs also need to be further developed and adapted to the complexity of alcohol environments in LMIC contexts.
As described above, there is also scope for specific analysis of policy processes in regard to alcohol environments in LMICs settings, including in regard to issues of policy transparency. Such political science analyses can investigate issues such as the role and power of interest groups supporting and opposing change, their interests and how they frame issues within policy debates and institutional processes (formal and informal) that support or constrain attention to alcohol policymaking at global, national and regional levels.43 44
The need for different survey tools and measurement
The qualitative research approaches described above are underused in regard to understanding the political economy dimensions of alcohol environments in LMICs. In terms of more quantitative approaches, alternative alcohol sources and differences in drinking cultures—and related differences in industry strategy—necessitate a more holistic approach to understanding alcohol environments in LMICs than has often been undertaken in HICs. Approaches should consider, for example, whether a high consumption of informally produced alcohol will lead to underestimates of real per-capita consumption levels if using national-level data from alcohol sales and taxation. While the under-reporting of alcohol consumption is not restricted to LMICs, the stigma associated with drinking and associated under-reporting in surveys may be particularly pronounced for some population groups, for example, differences in stigma associated with drinking between men and women, rural versus urban people and in some religious groups. The amount of ethanol consumed from non-market-based sources is difficult to quantify when production is not standardised, and such products are not included in sales and taxation data. Survey design in different settings also needs to be thoughtfully considered to reduce bias. Standardised survey tools for measuring alcohol consumption need to be fully validated and if necessary adapted for use in different drinking cultures, where for example the understanding or conceptualisation of a ‘drink’ may vary and definitions will require tools such as flashcards.
Conclusion
There is a critical need for better conceptualisation of what we describe here as the ‘alcohol environment’, including in regard to the methods and metrics for LMIC research application, to identify points of intervention and the development of effective regulation. Such conceptualisations of alcohol environments need to account for the socioecological interactions that influence alcohol production, distribution, acquisition, drinking contexts and the political economy influences on these including the role of the alcohol industry and its advertising and marketing—and the health and other impacts. Critically, a political economy approach, exploring associated policy processes, will help with understanding the political factors shaping the regulatory environment (or lack of) in LMICs and help with identifying key enabling or disabling factors and targets for possible policy intervention.
The framework that we present in figure 1 will, we hope, provide a structure from which many of these issues can be further examined to better characterise alcohol environments, and the political, commercial and sociocultural influences on alcohol use and associated harms in LMIC settings. This articulation of the alcohol environment and discussion of its implications may help to structure mixed methods empirical research examining alcohol environments including associated policy processes in LMICs. Improving understanding in LMIC contexts of alcohol acquisition and consumption, and associated advertising and marketing, as well as the political, economic and regulatory context in which the alcohol industry operates and associated policy processes, is vital to inform the design of interventions and policies to facilitate healthier alcohol environments, reduce the harms associated with alcohol consumption and contribute to addressing the significant burden of non-communicable disease globally as well as meeting the Sustainable Development Goals.
References
Footnotes
Handling editor Eduardo Gómez
Twitter @helenwalls
Collaborators We would like to acknowledge financial support for the publication of this article from the University of Cape Town and from the publication fund of UiT The Arctic University of Norway.
Contributors HW conceptualised this article and led the manuscript writing. All authors contributed critical content and contributed to manuscript writing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.