Article Text

Abstract
Introduction Preterm birth is the major cause of under-five mortality. Population-based data on determinants and proportions of children born preterm are limited, especially from low-income countries. This study aimed at assessing time trends and social, reproductive and environmental determinants of preterm births based on a population-based pregnancy cohort over 25 years in rural Bangladesh.
Methods In this cohort study in Matlab, a rural area in Bangladesh, we used data from the Health and Demographic Surveillance System from 1990 to 2014. Gestational age at birth was based on the reported last menstrual period and verified by ultrasound assessments. Preterm birth proportions were assessed within strata of social and reproductive characteristics, and time series analysis was performed with decomposition for trend and seasonality. We also determined the prevented fractions of preterm birth reduction associated with social and demographic changes during the follow-up period.
Results Analyses were based on 63 063 live births. Preterm birth decreased from 29% (95% CI 28.6 to 30.1) in 1990–1994 to 11% (95% CI 10.5 to 11.6) in 2010–2014. Low education, older age and multi-parity were associated with higher proportions of preterm births across the study period. Preterm births had a marked seasonal variation. A rapid increase in women’s educational level and decrease in parity were associated with the decline in preterm births, and 27% of the reduction observed from 1990 to 2014 could be attributed to these educational and reproductive changes.
Conclusion The reduction in preterm birth was to a large extent associated with the sociodemographic transition, especially changes in maternal education and parity. The persistent seasonal variation in the proportion of preterm birth may reflect the environmental stressors for pregnant women across the study period. Continued investments in girls’ education and family planning programmes may contribute to further reduction of preterm births in Bangladesh.
- preterm birth
- time trend
- education
- parity
- prevented fraction
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Globally, the prevalence of preterm birth is reported at 11% with 80% of these births occurring in South Asia and sub-Saharan Africa.
Studies in different countries have shown strong associations between a range of maternal sociodemographic factors and preterm birth.
What are the new findings?
This study provides unique information about the downward trend in preterm births in a rural Bangladeshi setting, revealing a reduction from 29% in 1990–1994 to 11% in 2010–2014.
One-quarter of the reduction in the proportion of preterm births could be attributed to the decrease in parity and the rapid expansion of girls’ education across this time period.
What do the new findings imply?
This study suggests that family planning and education programmes may substantially contribute to the reduction of preterm births in a low-income setting with basic maternal health services.
Introduction
Preterm birth, defined as the birth of an infant before 37 completed weeks of gestation, is the leading cause of death in children before the age of 5 years globally and accounts for one-third of the neonatal deaths.1 In the short term, preterm birth is associated with respiratory distress syndrome, bronchopulmonary dysplasia, necrotising enterocolitis, neurodevelopmental impairment including intraventricular haemorrhage, and cerebral palsy.2–4 There are also associations between preterm birth and long-term health consequences, such as chronic lung disease, hypertension and glucose intolerance.5–8
The worldwide average proportion of preterm births was estimated at 11% in 2014, corresponding to 15 million children born too soon annually.9 Over 80% of these preterm births occur in South Asia and sub-Saharan Africa. In a global comparison, Bangladesh has the highest proportion of preterm births with 19% of births occurring before gestational age week 37.9 Data from low-income and middle-income countries are generally scarce; accurate estimates regarding population-based preterm birth levels and trends over time are not available.9 10
The proportion of preterm births varies with socioeconomic conditions, ethnicity, level of women’s education, age and parity.11 12 An intervention study in Bangladesh, where a postpartum family planning intervention was integrated with maternal and neonatal health services, demonstrated increased inter-pregnancy intervals and decreased frequency of preterm birth.13 Knowledge is relatively limited regarding the mechanisms by which these social and reproductive characteristics are linked to biological mediators such as infection, inflammation, nutrition and stressors causing preterm birth.14 Some researchers argue that primary prevention will only be possible with an expanded knowledge of these socially related biological mechanisms.15 Our understanding is limited on whether reductions in the proportion of spontaneous preterm births also could be attributed to social transitions in society, for example, through increased levels of education of girls and successful family planning activities with reduced total fertility rates. Bangladesh has demonstrated strong equity-oriented policies and women-focused programmes including widespread education of girls that have contributed to impressive reductions of maternal and child mortality.16 It is not known, whether these policies and programmes influence the prevalence of preterm births.
The Global Strategy for Women’s, Children’s, and Adolescents’ Health under the Sustainable Development Goal 3 has emphasised the end to all preventable deaths and set targets to reduce the neonatal mortality to 12 per 1000 live births or lower by 2030 in every country.17 The recognition and prioritisation of reducing preterm births is a prerequisite for achieving this development goal.9 10
Studies investigating the prevalence of preterm births in low-income countries are scarce and available studies have been cross-sectional and based on data from hospitals or other non-representative data.9 To the best of our knowledge, there are no or very few longitudinal studies from low-resource settings that have monitored preterm birth trends over time.
The present study was based on prospectively collected pregnancy data in the time period of 1990–2014 from the Health and Demographic Surveillance System (HDSS) in rural Matlab, Bangladesh. The aims were to assess the proportion of preterm births based on last menstrual period (LMP) recall validated by ultrasound assessment during 2 years, and to analyse the association with maternal education levels, parity and season of birth in population-based pregnancy cohorts over these 25 years.
Methods
Study design, setting and sample
This cohort study was conducted in Matlab, a rural subdistrict of Bangladesh, where the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) has been running a HDSS in a population of about 220 000 since 1966 (STROBE checklist: online supplementary table SI). The population within the HDSS belongs to two distinct areas; the icddr,b and the government-serviced areas. In the icddr,b service area women of reproductive age and their children less than 5 years of age receive health services from icddr,b health facilities. In the government service area, the population receives care from the public health facilities similar to other parts of the country. While the demographic information has been collected since the inception of the HDSS in both areas, the reproductive and the child health information was not collected before 2002 in the government service areas. Therefore, our analyses are limited to the information from the icddr,b service area.
Supplemental material
The icddr,b service area has four administrative blocks; each block with a health subcentre, where midwives provide 24 hours maternal and child health services. The hospital located in Matlab town supports the subcentres in the management of patients referred from the lower levels.
In the study area, a Maternal Child Health and Family Planning programme started in 1978 with the distribution of family planning methods to women of reproductive age and provision of prevention and treatment services to women and children. Over the years, different functions have been added to improve maternal and child health. In 1987, a safe motherhood programme was introduced by icddr,b to increase the attendance by midwives from the subcentres at home deliveries. This strategy continued until 1996, after which facility-based delivery care was promoted. From 1996 to 2001, all four subcentres were upgraded and equipped to provide essential obstetric care, and midwives’ support to home births was no longer offered. In 2007, a new Maternal, Neonatal, and Child Health (MNCH) programme was initiated to strengthen the ongoing maternal and child health services in line with the continuum of pregnancy, delivery and postpartum care. Efforts were made to integrate community and facility levels of care. The details of these interventions and the process of implementation of the programme have been described elsewhere.18
The study sample included women in the icddr,b service area, who were identified as pregnant at routine household visits by Community Health Research Workers (CHRWs) and delivered live born babies during the study period. We took advantage of the MNCH study conducted in 2007–2010 in the study area, and used the information from that study on ultrasound assessment of gestational age at the first antenatal care visit to validate the gestational age at birth based on the reported LMP recorded by the HDSS.
Data collection
The present study used the information available from HDSS databases. In the study area, the frequency of routine home visits by the CHRWs varied over the study period: fortnightly until 2001, monthly from 2002 to 2006, and bi-monthly from 2007. The CHRWs identified pregnant women by their histories of missing menstruations. Pregnancy was after that confirmed at subsequent visits and followed up for type and date of pregnancy outcomes. The LMP date was determined by recall during the pregnancy identification interviews. The gestational age at birth was calculated by subtracting the LMP date from the date of pregnancy outcome. Live births were categorised into preterm birth (birth before 37 weeks of gestation) or term birth (gestational age at birth ≥37 weeks). Preterm births were further divided into very preterm (<32 weeks of gestation) or moderate preterm (32–33 weeks of gestation) or late preterm (34–36 weeks of gestation) births.
Information on women’s age, parity, education and household wealth was obtained from the HDSS databases. Parity was defined as the number of live births and stillbirths born before the current pregnancy. Educational level was determined as the number of years completed at school. Household wealth was assessed by generating scores through principal component analysis based on ownership of household assets during a certain time period such as consumer items (radio, watch, etc), but also dwelling characteristics (wall and roof material), and type of drinking water and toilet facilities. These scores were indexed into quintiles, where one represented the poorest and five the wealthiest or least poor households. Bangladesh has three distinct seasons; the hot premonsoon season from March through May, the rainy monsoon season from June through October and the cool and dry winter from November through February.
Analyses
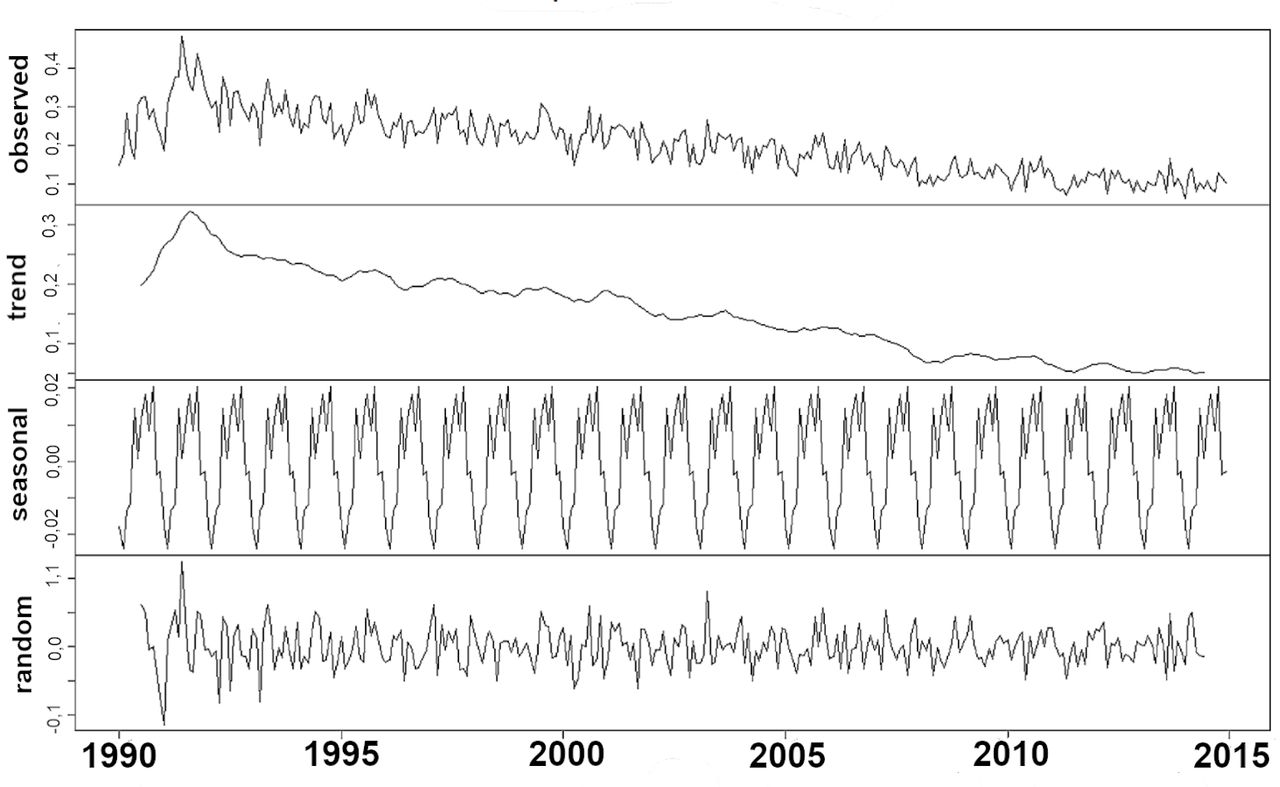
The characteristics of the study sample in the period of 1990–2014 in total and in intervals of each 5-calendar year periods were presented in frequencies, proportions or by means (SD). The original monthly time series of the proportion of preterm births were decomposed into the components trend, seasonality and random noise, assuming seasonal additive components.19 The trend was statistically analysed by Mann-Kendall test20 and the seasonal variation by fitting a general linear model to the data with the function ‘monthglm’ in the time series package in R21 called ‘season’.22
We graphically displayed preterm birth prevalence by year. The proportions of preterm births were analysed by background characteristics and also the distribution of background characteristics were presented graphically in 5-calendar year periods. The associations between covariates and preterm births were assessed by χ2 tests.
The risk of preterm birth by available covariates was analysed with logistic regression and presented as ORs with their 95% CIs. To analyse the prevented fraction, we estimated the risk of preterm birth in different parity (<3, ≥3) and education groups (<6 years, ≥6 years) in each 5-year interval, adjusting for potential confounding factors. Thereafter we calculated the prevented fractions of preterm birth that could be attributed to belonging to the more favourable groups in parity and maternal education. The prevented fraction was calculated as P(1-OR), where P was the change in prevalence of lower parity and higher education level, respectively, from one calendar period to the next.
The LMP-based assessments of gestational age at birth were compared with the ultrasound measurement in early pregnancy from 2009 to 2010 by computing Cronbach’s alpha to assess the reliability of the reported LMP. We also calculated the proportions of preterm birth by the two methods and tested the difference in proportions by χ2 test.
Patient and public involvement
Community residents or patients were not included in the elaboration of the research questions and study design. The results of this study will be distributed to stakeholders such as the Ministry of Health and Family Welfare of the Government of Bangladesh, and the local Non-Government Organisations, after publication in a scientific journal.
Results
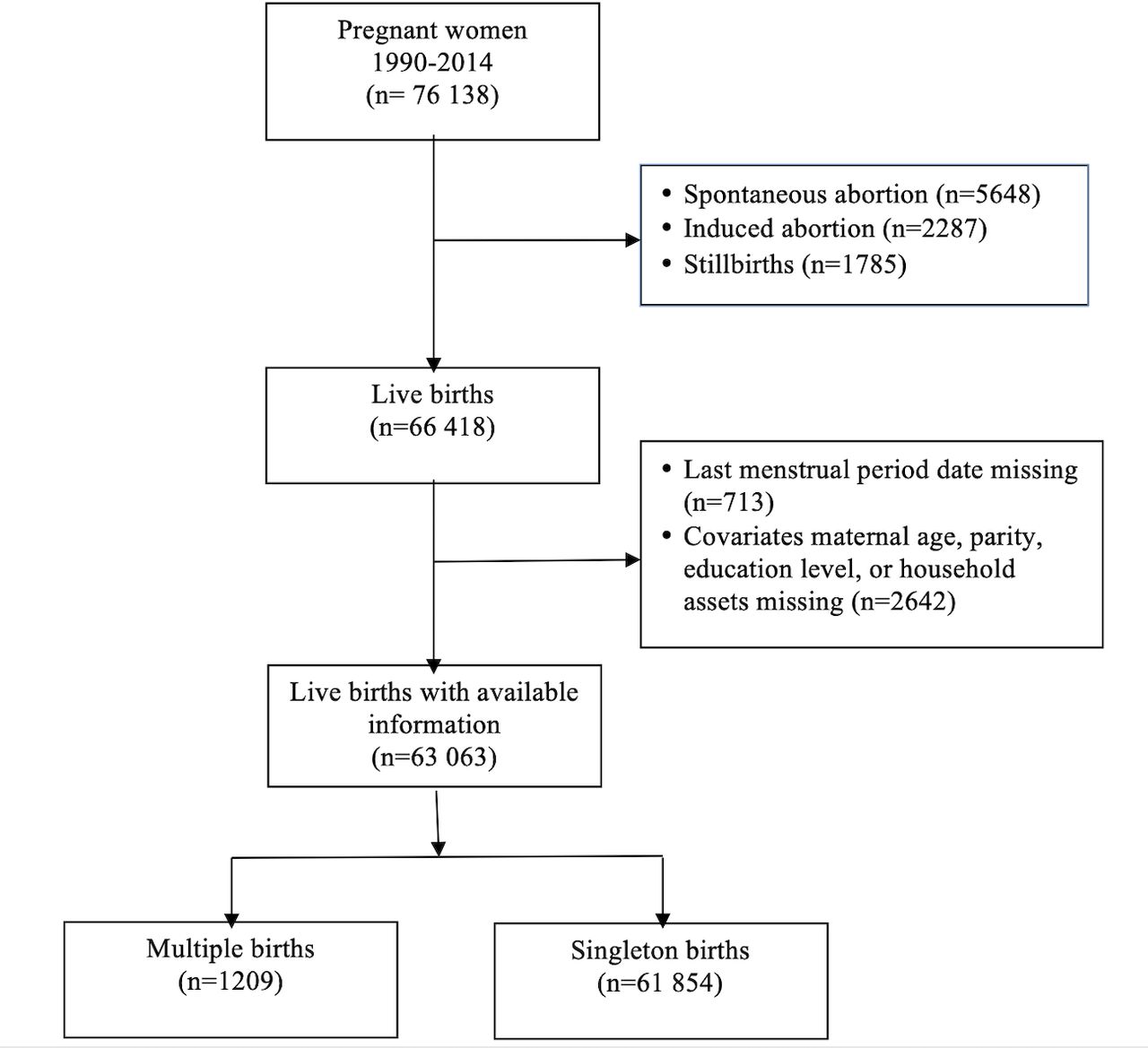
There were 76 138 pregnancies recorded in the databases in the period of 1990–2014, of which 66 418 resulted in live births and 1790 in stillbirths. In the present study, analyses were based on 63 063 live births. The reasons for exclusion of 3355 live births from the study were due to missing LMP information or pregnancy outcome dates (n=713) or missing covariate information such as maternal age or education levels or asset scores (n=2642) (figure 1). Out of the total number of live births included in the analysis, 61 854 (98%) were singletons, and multiple pregnancies contributed 1209 live births. The mean gestational ages at delivery were 38.6 (SD 2.5) and 35.7 (SD 3.3) weeks, respectively, for singleton and multiple births. The proportions of preterm births were 19.7% and 59.7% for singletons and multiple births, respectively.

Study profile.
In total, 2700 ultrasound assessments were available for participants in the MNCH project during the period 2009–2010.18 Gestational age measured by ultrasound-based LMP and reported LMP had a Cronbach’s alpha of 0.89. The proportions of preterm birth were 8.2% and 7.9% by ultrasound and LMP-based assessments, respectively (p=0.92).
The distribution of background characteristics indicated an ongoing social and demographic transition (table 1). Across the study period, the age-at-birth distribution was relatively constant. The women in the birth cohort 2010–2014 had lower parity and were more educated in comparison with the birth cohort 1990–1994. Parity of three or more decreased from 31% to 9%, and women without education decreased from 46% to 5%.
Characteristics of the study women and frequencies of term and preterm live births in 5-calendar year periods from 1990 to 2014 in Matlab, Bangladesh
We observed a pronounced reduction in the prevalence of preterm birth across the 25 years of the study. In the interval 1990–1994 more than 29% (95% CI 28.6 to 30.1) of the live births were preterm compared with 11% (95% CI 10.5 to 11.6) in 2010–2014 (table 1 and figure 2). All categories of preterm births decreased from 1990 to 2014 (table 1). The annual reduction of preterm birth rate was 2.8%, 3.3% and 2.3% from the estimated rates of 23.3%, 6.1% and 2.8% for late, moderate and very preterm births, respectively (figure 2). There was a monotonic downward trend in preterm births over time (test for trend p<0.001) (figure 3). Across the study period there was a seasonal variation in preterm births with the lowest proportion at the beginning of the calendar year and peaks in February (cool and dry winter), June, September (rainy monsoon season) and November (cool and dry winter) (online supplementary table S2).
Supplemental material

Preterm birth proportions (gestational age at birth <37 weeks, <32 weeks, 32–33 weeks and 34–36 weeks, respectively) by year in the study area in Matlab, Bangladesh. The linear trend equation indicated 2.3% (y=−0.0629x+2.78), 3.3% (y=−0.2037x+6.14) and 2.8% (y=−0.6605x+23.3) annual reduction of very preterm, moderate preterm and late preterm births, respectively.

Decomposition of additive time series analysis of occurrence of preterm births in Matlab, Bangladesh. The observed data, the time trend (p<0.001), the seasonal variation and the remaining random variation are displayed.
Preterm births decreased over calendar time in all maternal age groups, parity groups and maternal education groups (figure 4). Preterm births occurred most frequently in the highest parity group (≥3) and oldest age group (≥35), which both decreased over time. Mothers with 6 years of education or more had the lowest prevalence of preterm births, and this educational level steadily increased over the observed 25 years.

Proportion of preterm births (graphs to the left) stratified by age, parity and educational levels in 5-year calendar period from 1990 to 2014, in Matlab, Bangladesh. The distributions (per cent) of these stratifying characteristics are given for the same intervals of calendar periods (graphs to the right).
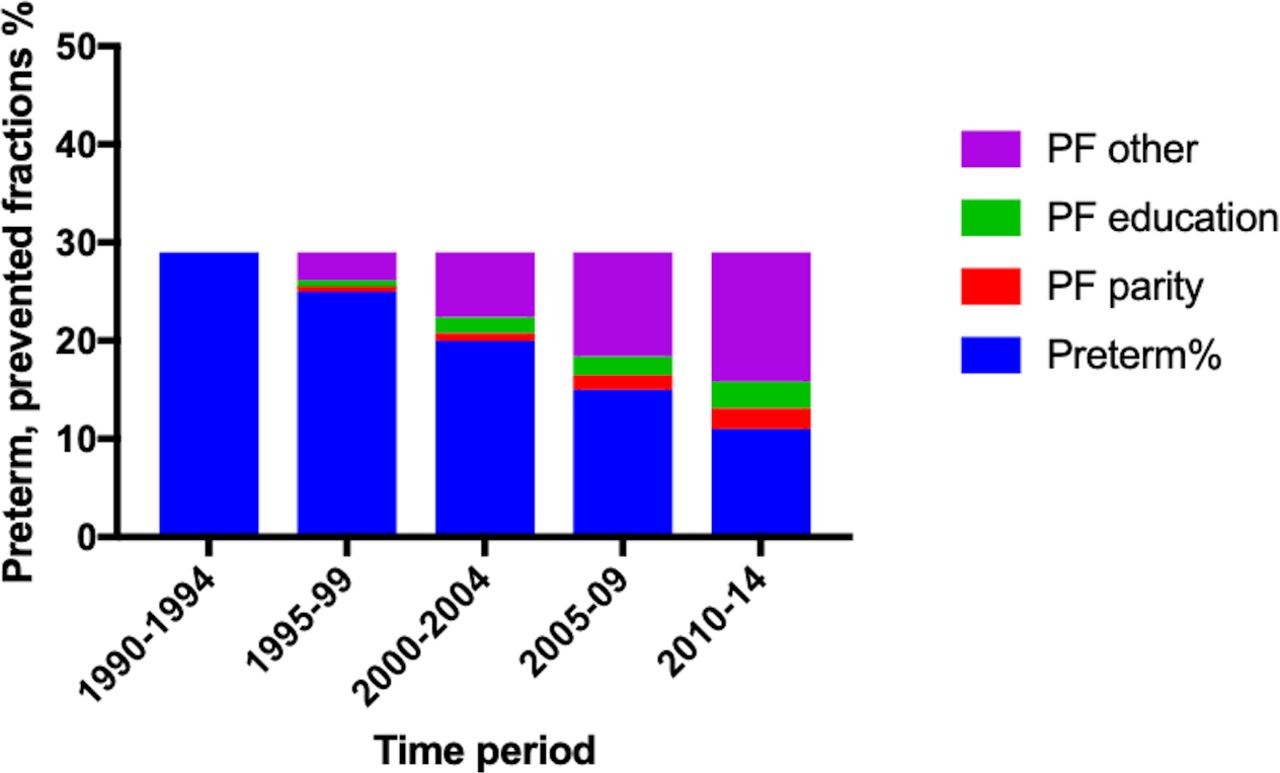
All the available covariates were associated with preterm birth (online supplementary table S3). The risk of preterm birth by parity groups and educational levels adjusted for potential confounding factors are displayed in table 2. The adjusted OR for parity less than three compared with three or more varied from 0.57 (95% CI 0.50 to 0.64) to 0.80 (95% CI 0.73 to 0.87), and the adjusted OR for 6 years of education or more compared with less than 6 years varied between 0.73 (95% CI 0.66 to 0.80) and 0.84 (95% CI 0.77 to 0.92). The proportions of births having those desirable characteristics increased considerably between 1990–1994 and 2010–2014. These figures are reflected in the estimated prevented fractions of preterm births across the study period (figure 5). From the first to the last interval, more than a quarter (27%) of the preterm birth reduction could be attributed to the combination of change in parity (12%) and educational levels (15%) of the mothers. However, 73% of the reduction of preterm birth rate in the same period was contributed by other factors (figure 5).
Supplemental material
The risk of preterm birth in different sociodemographic groups and the prevalence of these characteristics in the study periods 1990–1994, 1995–1999, 2000–2004, 2005–2009 and 2010–2014

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion preterm births in 5-year calendar periods from1990 to 2014 and the prevented fractions (PF) related to changes in parity and educational levels across these periods. Figures based on the ORs for parity <3 and education ≥6 years and the change in the prevalence of these characteristics.
Discussion
The burden of preterm birth remains a public health issue all over the world. To date, limited information is available about the role of sociodemographic transition in preterm birth trends. In this cohort study we have demonstrated that the proportion of preterm births decreased from 29% in 1990–1994 to 11% in 2010–2014 in Matlab, a rural area in Bangladesh. We also observed that all categories of preterm birth decreased throughout the 25 years of the study period. There was a marked seasonal variation in the proportions of preterm birth. More than a quarter of the reduction in preterm births could be attributed to decreased parity and increased levels of maternal education. The study findings highlight the importance of continued investments in girls’ education and family planning programmes to reduce the preterm birth rates in a low-income setting with basic maternal health services.
Data are scarce about trends in preterm birth rates in low-income settings.9 The observed preterm birth proportion of 11% in Matlab in 2010–2014 differs substantially from the reported frequency of 19.1% (95% CI 13.2 t0 26.2) in Bangladesh in a global review paper.9 The latter figure might have been influenced by a study in 2002–2006 in northern Bangladesh showing 19.4% preterm births.23 The preterm birth rate of 20% observed in our study in the corresponding calendar period in Matlab indicates a similar level of preterm birth burden at that time. In an umbilical cord cleansing trial in northern Bangladesh the proportion preterm birth was 22% in 2007–2009,24 and in a secondary analysis of data from a maternal infection screening trial, also in northern Bangladesh from 2012 to 2016, preterm births were 23%.25 There was a peak observed in the present study in the proportions of preterm births in 1991—a year with the devastating cyclone Gorky that hit the country during the pre-monsoon season, a pronounced flooding during the monsoon and a major cholera outbreak. Such environmental stressors may substantially contribute to the high preterm birth rate that year.
In a majority of countries with high-quality data, preterm birth rates have reportedly increased since 2000.9 This increase, which mainly consists of late preterm births, has been related to the increase in obstetric interventions including caesarean sections performed before gestational week 37.26 The Demographic Health Surveys reported that the national caesarean section rate increased from 4% in 2002 to 23% in 2014 in Bangladesh.27 A high caesarean section rate has also been observed in a cross-sectional study in the Matlab area.28 This increased rate probably did not influence the observed preterm birth rates, since most caesarean sections are performed at gestational age ≥37 weeks.
The seasonality analysis revealed a lower frequency of preterm birth in the cooler season at the beginning of the years and a tendency of higher proportions mainly in the pre-monsoon and monsoon seasons. Even in high-income countries, it is reported that high temperatures may trigger preterm birth29 or earlier birth of term pregnancies.30 The findings of a persistent seasonal variation in preterm birth rates in the present study add to other evidence of environmental influences on pregnancy, fetal development and the young child. Studies in the Matlab area have shown seasonal variation in the effect of food supplementation on birth weight,31 an association between season of conception and linear growth from birth to pre-adolescence and stunting at ten years,32 and seasonal variation of infant anaemia.33 Such health and nutrition effects on pregnant women, fetuses and young children might increase with climate change, increasing climate variability and other increasing environmental influences in countries like Bangladesh.34
The family planning programme in Matlab, which was experimentally initiated in 1977, was a success in fertility reduction, increased birth spacing, improved child survival,35 and resulted in positive effects on maternal and child nutrition and economic growth.36 The present study suggests that the reduced frequency of preterm birth might be added to the list. Such a conclusion is also supported by an intervention study in Bangladesh, that documented a reduced preterm birth rate when integrating a postpartum family planning programme into maternal and newborn health services.13 A systematic review and a cohort study have suggested some plausible mechanisms for the link between birth spacing and preterm births that include factors such as maternal nutrition, infections, cervical insufficiency37 and premature rupture of membranes.38
The differentials in preterm births between maternal educational groups were relatively constant over the observed 25 years, while the maternal educational level rapidly increased. Education level is one of the social determinants of preterm birth found across different continents and contexts.12 An educational gradient in preterm births has been relatively constant even in the Nordic countries.39 In the USA, education level of the mother has explained a substantial part of the excess proportion of preterm births among black women.40 The more proximate factors beyond education include infections, nutrition and toxic exposure. These factors differ between contexts; in western societies, smoking may be an important factor,12 while almost no mother smokes in this Bangladeshi setting. It is beyond the scope of this study to disentangle which factors have been important in mediating the education effect on spontaneous preterm birth in the Matlab setting.
It should be noted, that family planning and basic antenatal and delivery services were available throughout the observed period. In 2005–2006, before the MNCH project, 38% of the pregnant women made three or more antenatal care visits and 55% delivered at health facilities, while 3 years later, after the completion of that project, the corresponding figures were 78% and 72%.18 The improved coverage and quality of the antenatal and delivery services over time may have contributed to the reduction in preterm births.
The present study is unique in reporting prospectively collected population-based data from a low-income setting covering all women who gave birth over 25 years. There were few omissions due to missing information on gestational age at birth (1%) or missing covariate information (4%). It is highly unlikely that these omissions influenced the results. Obtaining accurate gestational age-at-birth data is a challenge in low-income countries.10 Here, the LMP information was collected at home as part of a high-quality surveillance system with very frequent visits. Further, the information was validated during 2 years with early pregnancy ultrasound assessments of gestational age showing high agreement. The information on household wealth index, maternal education levels and parity was retrieved from the HDSS databases that maintained a high accuracy. The gradual reduction in preterm births took place in a context where basic maternal health services were provided and these services were gradually improved over time. However, the inter-pregnancy interval and service utilisation information for the cohort was not available. Thus, an analysis was not possible whether these factors mediated the association between change in parity and education level and preterm births.
The dramatic decrease in the preterm birth burden over 25 years in Matlab illustrates that improvement is possible from extremely high to a moderate level of preterm births in a context with fertility reduction, expansion of girls’ education, and essential reproductive, maternal, and child health services. This study illustrates that actions on social determinants may render significant reductions in the rate of babies born too soon—even if the biological enigma of spontaneous preterm birth persists.15 The knowledge gaps regarding biological or social mediators of the social determinants should not preclude action also on distant factors, when possible. In a US study, upward social mobility was associated with a decreased risk of preterm birth and the authors suggested that efforts to improve socioeconomic conditions could lower these rates.41
In conclusion, the present study provides unique information about the downward trend in preterm births in a rural Bangladeshi setting. The observed reduction in preterm births was, to a large extent, associated with the sociodemographic transition, especially changes in maternal education and parity. The persistent seasonal variation in the proportion of preterm births may reflect the environmental stressors for pregnant women across the study period. The present results indicate that reduction of preterm births might be added to the exceptional health achievements in Bangladesh that have resulted from women-focused efforts, including education of girls and provision of equitable and essential maternal and child health services.16
Acknowledgments
This research study was funded by icddr,b core donors, which provide unrestricted support to icddr,b for its operations and research. Current donors providing unrestricted support include the Government of the People’s Republic of Bangladesh; Global Affairs Canada (GAC); Swedish International Development Cooperation Agency (Sida) and the Department for International Development (UK Aid). We gratefully acknowledge these donors for their support and commitment to icddr,b's research efforts.
References
Footnotes
Handling editor Seye Abimbola
Contributors AR and LÅP designed the study. AR, MR, JP, AR, SA and JUA prepared the dataset and were involved in the preliminary analysis. AR and LÅP prepared the first draft of the manuscript. All authors participated in editing the manuscript and approved the final version for submission. The corresponding author had full access to all data and had the final responsibility for the decision to submit for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.