Article Text

Abstract
Background This randomized trial compared ultrasound-guided pericapsular nerve group block and suprainguinal fascia iliaca block in patients undergoing primary total hip arthroplasty. We selected the postoperative incidence of quadriceps motor block (defined as paresis or paralysis of knee extension) at 6 hours as the primary outcome. We hypothesized that, compared with suprainguinal fascia iliaca block, pericapsular nerve group block would decrease its occurrence from 70% to 20%.
Methods Forty patients undergoing primary total hip arthroplasty under spinal anesthesia were randomly allocated to receive a pericapsular nerve group block (n=20) using 20 mL of adrenalized levobupivacaine 0.50%, or a suprainguinal fascia iliaca block (n=20) using 40 mL of adrenalized levobupivacaine 0.25%. After the performance of the block, a blinded observer recorded pain scores at 3, 6, 12, 18, 24, 36, and 48 hours; cumulative breakthrough morphine consumption at 24 and 48 hours; opioid-related side effects; ability to perform physiotherapy at 24 and 48 hours; as well as length of stay. Furthermore, the blinded observer also carried out sensory assessment (of the anterior, lateral, and medial aspects of the mid-thigh) and motor assessment (knee extension and hip adduction) at 3, 6, and 24 hours.
Results Compared with suprainguinal fascia iliaca block, pericapsular nerve group block resulted in a lower incidence of quadriceps motor block at 3 hours (45% vs 90%; p<0.001) and 6 hours (25% vs 85%; p<0.001). Furthermore, pericapsular nerve group block also provided better preservation of hip adduction at 3 hours (p=0.023) as well as decreased sensory block of the anterior, lateral, and medial thighs at all measurement intervals (all p≤0.014). No clinically significant intergroup differences were found in terms of postoperative pain scores, cumulative opioid consumption at 24 and 48 hours, ability to perform physiotherapy, opioid-related side effects, and length of hospital stay.
Conclusion For primary total hip arthroplasty, pericapsular nerve group block results in better preservation of motor function than suprainguinal fascia iliaca block. Additional investigation is required to elucidate the optimal local anesthetic volume for motor-sparing pericapsular nerve group block and to compare the latter with alternate motor-sparing strategies such as periarticular local anesthetic infiltration.
Trial registration number NCT04402450.
- nerve block
- pain
- postoperative
- pain management
- lower extremity
- acute pain
Data availability statement
Data are available on reasonable request. The deidentified data are available on reasonable request to the corresponding author.
Statistics from Altmetric.com
Introduction
In recent years, ultrasound (US)-guided suprainguinal fascia iliaca block (SIFIB) has emerged as a reliable analgesic option for total hip arthroplasty (THA)1 that rivals lumbar plexus block in terms of pain control and breakthrough opioid consumption.2 However, SIFIB may lead to decreased motor strength of the surgical limb2 thereby hindering postoperative mobilization3 and delaying discharge after outpatient THA.4 In 2018, Girón-Arango et al 5 described a new block, termed pericapsular nerve group (PENG) block, which selectively targets the articular branches of the femoral and accessory obturator nerves while sparing their motor components.
In this randomized trial, we compared US-guided SIFIB and PENG block in patients undergoing primary THA. Since an important benefit associated with PENG block stems from its motor-sparing effect, we selected the incidence of quadriceps motor block (at 6 hours) as our primary outcome. We hypothesized that, compared with SIFIB, PENG block would decrease its occurrence from 70% to 20%.
Material and methods
The current trial (online supplemental file 1) was registered at ClinicalTrials.gov (Study ID: NCT04402450) on 5/26/2020 prior to patient recruitment. Ethics committee approval (Hospital Clínico Universidad de Chile) was secured on 4/1/2020. All study data were collected and managed using the REDCap electronic data capture tool hosted at the University of Chile.6 The 40 subjects were recruited over a period of 9 months (8/31/2020 to 5/25/2021) (figure 1).
Supplemental material
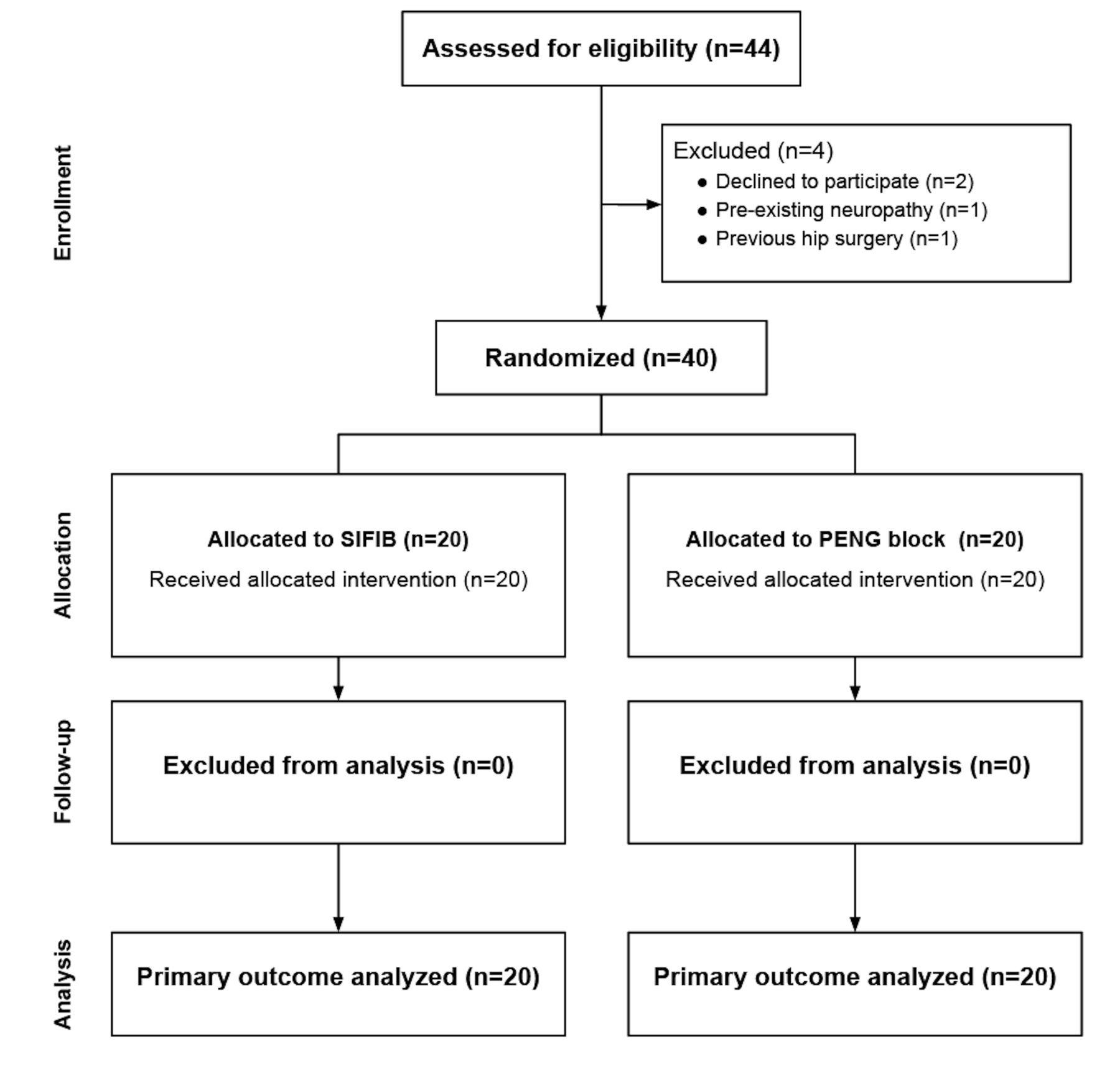
CONSORT diagram. PENG, pericapsular nerve group block; SIFIB, suprainguinal fascia iliaca block.
After obtaining written informed consent, we enrolled 40 patients undergoing primary THA. Inclusion criteria were: age between 18 and 80 years, American Society of Anesthesiologists (ASA) physical status I to III, and body mass index between 18 and 35 kg/m2. Exclusion criteria were: inability to consent to the study, coagulopathy, sepsis, hepatic or renal failure, allergy to local anesthetic (LA), prior surgery of the inguinal or suprainguinal area, pregnancy, and opioid intake at home
All patients received spinal anesthesia with 10 mg of isobaric bupivacaine (ie, 2 mL of bupivacaine 0.5%) and 20 µg of fentanyl. All surgical interventions were performed by the same team of surgeons (CB, RW, JB) using a posterior approach and a lateral decubitus position. During the case, propofol sedation through a target-controlled infusion (site effect concentration=0.5–1 ug/mL) was provided at the discretion of the treating anesthesiologist, provided patient response to verbal stimulus was maintained. At the end of the case, all patients received intravenous ketoprofen (100 mg) and paracetamol (1 g).
On arrival in the postanesthesia care unit (PACU), using a computer-generated sequence of random numbers and a sealed, opaque envelope technique, patients were randomly allocated to receive US-guided PENG block (n=20) or SIFIB (n=20). The randomization list and opaque envelopes were created by a research assistant who was not otherwise involved in patient care. All blocks were performed by trainees (Fellows or residents) and supervised by one of three coauthors (DB, SL, JA). The US machine (GE Logiq e, GE Healthcare, Wauwatosa, Wisconsin, USA), 4–13 MHz linear US transducer, 100 mm, 20-gauge, short-beveled block needles (Stimuplex Ultra 360, B Braun Medical, Melsungen, Germany), and block adjuvants (4 mg of intravenous dexamethasone) were identical for all subjects. Furthermore, the total dose of levobupivacaine (100 mg) was also similar for both groups; however, for PENG blocks, a concentration of 0.5% was used in order to respect the 20 mL-injectate advocated by Girón-Arango et al.5 In contrast, for SIFIB, a 0.25%-concentration and a 40 mL-volume2 were administered.
Performance of nerve blocks
For PENG blocks, patients were placed in the supine position. The US transducer was placed in a transverse orientation, medial, and caudal to the anterosuperior iliac spine in order to identify the anteroinferior iliac spine, the iliopubic eminence, and the psoas tendon.5 Using an in-plane technique and a lateral-to-medial direction, the block needle was advanced until its tip was positioned between the periosteum and psoas tendon (figure 2). The LA (20 mL of levobupivacaine 0.5% with epinephrine 5 µg/ mL) was injected following negative aspiration.

Sonoanatomy of PENG block. AIIS, anterior inferior iliac spine; Asterisk (white), target for local anesthetic injection; FA, femoral artery; IM, iliac muscle; IPE, iliopubic eminence; PT, psoas muscle tendon.
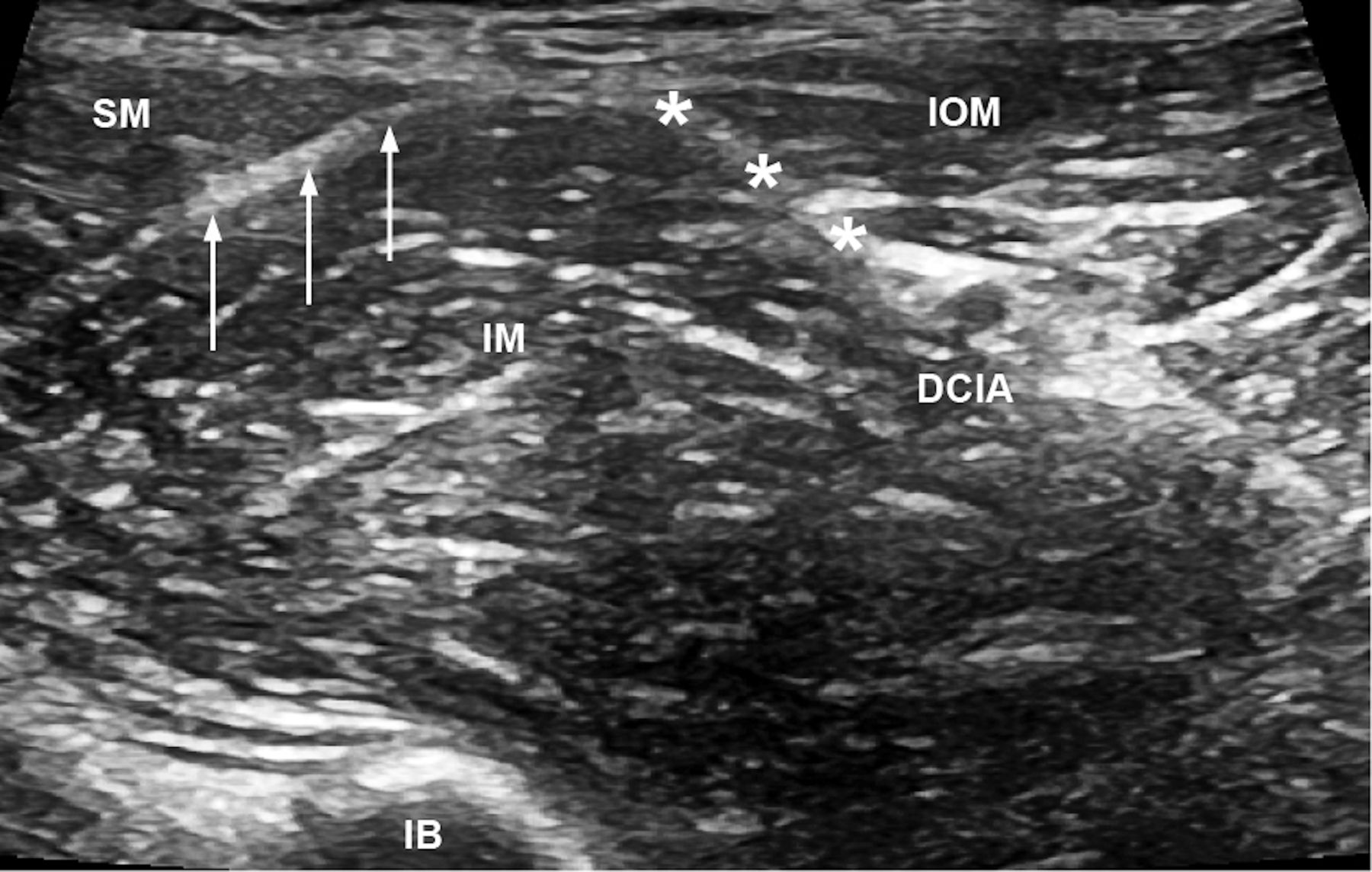
For SIFIBs, patients were placed in the supine position. The US transducer was placed in a parasagittal orientation, medial to the anterosuperior iliac spine in order to obtain the “bow-tie” sign.1 The sartorius, iliacus, and internal oblique muscles were identified.2 Using an in-plane technique and a caudad-to-cephalad direction, the block needle was advanced until its tip was positioned between the internal oblique and iliacus muscles underneath the fascia iliaca (figure 3). Following negative aspiration, the LA (40 mL of levobupivacaine 0.25% with epinephrine 5 µg/ mL) was injected as the needle was slowly advanced cephalad inside the fascia iliaca compartment.

{kind=link}
{kind=link}
{kind=link}
Sonoanatomy of suprainguinal fascia iliaca block. Asterisks (white), target for local anesthetic injection; arrows (white), fascia iliaca; DCIA, deep circumflex iliac artery; IB, iliac bone; IM, iliac muscle; IOM, internal oblique muscle; SM, sartorius muscle.
During the performance of PENG blocks and SIFIBs, the screen of the US machine was systematically turned away from the patient’s field of vision.
Postoperative analgesic regimen
In the PACU, after the performance of the PENG block or SIFIB, all patients received patient-controlled analgesia (morphine bolus=1 mg; lockout interval=8 min). On the surgical ward, in addition to patient-controlled morphine analgesia, they also received regular acetaminophen (1 g per os every 6 hours) and ketoprofen (100 mg per os every 8 hours) during 48 hours.
Primary outcome
Our primary outcome was the incidence of quadriceps motor block (defined as paresis or paralysis of knee extension) at 6 hours postoperatively. Knee extension was evaluated in a supine position with the patient’s hip and knee flexed at 45° and 90°, respectively. The patient was asked to extend the knee first against gravity and then against resistance. Knee extension was graded according to a 3-point scale: 0=normal strength (extension against gravity and against resistance); 1=paresis (extension against gravity but not against resistance); 2=paralysis (no extension possible).2
Secondary outcomes
During the performance of the blocks, recorded secondary outcomes included performance time (defined as the temporal interval between the start of skin disinfection and the end of LA injection through the block needle) as well as the incidence of block-related adverse events (ie, vascular puncture, paresthesia, LA toxicity).
Postoperatively, secondary outcomes included static (at rest) and dynamic (with hip adduction) pain scores at 3, 6, 12, 18, 24, 36, and 48 hours; cumulative morphine consumption at 24 and 48 hours; opioid-related side effects (ie, postoperative nausea/vomiting, pruritus, urinary retention, respiratory depression); inability to perform physiotherapy at 24 and 48 hours due to motor block or pain; as well as length of stay.
Postoperative sensory block was assessed in the anterior, lateral and medial aspects of the mid-thigh at 3, 6, and 24 hours. For each territory, blockade was evaluated using a 3-point scale: 0=no block, 1=analgesia (patient can feel touch, not cold), 2=anesthesia (patient cannot feel touch).2
Postoperative motor block was assessed using knee extension and hip adduction. In addition to 6 hours, knee extension was also evaluated at 3 and 24 hours according to the same 3-point scale described for the primary outcome (vide supra). Since hip adduction originates from the lumbar and sacral plexi, it was evaluated by comparing postblock to baseline strength. Preoperatively, a blood pressure cuff, inflated at 40 mm Hg, was inserted between the knees of the patient: the latter was then instructed to squeeze the cuff with the operative limb as hard as possible and to sustain the effort. Postoperatively, hip adduction was assessed at 3, 6, and 24 hours. We defined hip adduction scores of 0, 1, and 2 points as decreases in strength of 0%–20%, 21%–70%, and 71%–90% compared with baseline measurement, respectively.2 7
Except for performance time and the incidences of vascular puncture, paresthesia and LA toxicity (which were recorded by the coauthor supervising the block), all other outcomes were evaluated by a blinded investigator. The latter also recorded demographic data (ie, sex, age, weight, height, and ASA class) and surgical duration.
Sample size calculation and statistical analysis
Our experience with SIFIB suggests that the incidence of quadriceps motor block (paralysis or paresis) at 6 hours hovers around 70%.2 We hypothesized that PENG block would decrease its incidence to 20%. Thus, a calculated sample size of 16 patients per group was required for a statistical power of 0.80 and a two-tailed type I error of 0.05. A total of 40 subjects was recruited to account for possible dropouts.
Statistical analysis was performed using SPSS V.21 statistical software (IBM, Armonk, New York). For continuous data, normality was first assessed and then analyzed with the Student t-test. Data that did not have a normal distribution, as well as ordinal data, were analyzed with the Mann-Whitney U test. For categorical data, the χ² test was used. The Fisher’s exact test was used when any cell for the aforementioned categorical data had an expected count of less than five. All p values presented were two-sided and values inferior to 0.05 were considered significant.
Results
Demographic characteristics and surgical duration are presented in table 1.
Patient characteristics
Compared with SIFIB, PENG block resulted in a lower incidence of quadriceps motor block at 3 hours (45% vs 90%; p<0.001) and 6 hours (25% vs 85%; p<0.001) as evidenced by improved knee extension (table 2). Furthermore, PENG block also resulted in decreased paresis/paralysis of hip adduction at 3 hours (50% vs 90%; p=0.023) (table 2). Compared with SIFIB, PENG was associated with decreased sensory block of the anterior, lateral, and medial thighs at all measurement intervals (all p≤0.014) (table 2).
Sensory and motor block assessment
No intergroup differences were found in terms of block performance time, static pain scores, cumulative opioid consumption at 24 and 48 hours, time, ability to perform physiotherapy at 24 and 48 hours, block-related adverse events, opioid-related side effects, and length of hospital stay (table 3). Dynamic pain scores were lower with SIFIB at 3 and 36 hours (both p=0.021) but no intergroup differences were observed at other time intervals (table 4).
Block performance data and postoperative outcomes
Postoperative pain scores
Discussion
In this randomized trial, we compared US-guided PENG block and SIFIB in patients undergoing primary THA. Our findings suggest that PENG block results in improved preservation of knee extension (at 3 and 6 hours) and hip adduction (at 3 hours) without significantly sacrificing postoperative pain control or increasing breakthrough opioid consumption. Although our findings validate the motor-sparing benefits provided by PENG blocks, we must highlight the fact that the latter do not seem to circumvent motor block altogether. For instance, at 3 hours, 45%–50% of subjects randomized to PENG blocks experienced some paresis or paralysis of knee extension or hip adduction. However, the impairment in quadriceps function appears short-lived: in our study, at 6 hours, only 25% of subjects still experienced decreased knee extension. In contrast, at 6 hours, residual impairment in hip adduction persisted in 50% of patients. We speculate that the decrease in knee extension may stem from LA spread to the femoral nerve.8 9 In contrast, decreased hip adduction could originate from postsurgical hip pain. Alternately, some authors have reported possible obturator motor blockade in the setting of PENG block if the needle tip is positioned medially along the iliopubic eminence10 or if large injectates are employed.11 Consequently, future dose-finding trials are required to elucidate the maximal effective volume of LA in 90% of subjects (MEV90) for motor-sparing PENG block. Furthermore, future investigation is needed to compare PENG blocks with alternate motor-sparing strategies such as periarticular LA infiltration.
The lack of intergroup differences in terms of ability to perform physiotherapy deserves special mention. Since PENG blocks result in improved motor strength of the surgical limb, one would also expect an inherent improvement in physiotherapy performance. We attribute the lack of intergroup differences to two factors. First, the ability to perform physiotherapy constituted a secondary variable: thus, our trial may have been underpowered to detect significant differences in this outcome. More importantly, our current postoperative pathway for THA (eg, first session of physiotherapy only at 24 hours) may have been inadequate to fully reap the motor-sparing benefits of PENG blocks.
Our control group (SIFIB) requires discussion, as one could argue for the inclusion of a third (placebo) group. We elected to forego such a true control group for two reasons. First, Desmet et al 1 have already demonstrated that, compared with no block, SIFIB results in lower pain scores and decreased opioid consumption (at 24 and 48 hours). Second, in our center, the analgesic criterion standard for THA includes the provision of peripheral nerve blocks.2 In hindsight, the lack of a placebo group is unlikely to hinder clinical interpretation of our results, as Pascarella et al 12 have recently demonstrated that, compared with no block, PENG block yields lower maximal pain scores and opioid consumption during the first 48 hours after THA. Thus, the combined findings of Desmet et al 1 and Pascarella et al 12 obviate the need for sham injections or placebo.
Our protocol contains some limitations. First, despite our best effort, our subjects may not have been blinded. Although the screen of the US machine was purposefully turned away from their field of vision during the performance of the blocks, patients could have nonetheless guessed group allocation based on more pronounced sensorimotor block (SIFIB group). Second, our results are specific to single-injection blocks. Additional studies are required to confirm our findings for continuous PENG block and SIFIB.
In conclusion, for primary THA, PENG block results in better preservation of motor function than SIFIB. Additional investigation is required to elucidate the MEV90 for motor-sparing PENG block and to compare the latter with alternate motor-sparing strategies such as periarticular LA infiltration.
Data availability statement
Data are available on reasonable request. The deidentified data are available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Dr Estela Maulén, Dr María Mercedes Aguirre, Ada Tapia (physiotherapist) and Dana Rothfeld (physiotherapist) for their assistance with patient recruitment.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AlisteJulian, @s_layera, @danibrava, @jaroncio
Contributors SL, JA, DB, AJ, GM, CB, RW and JB participated in the planning, conception, design, conduct, reporting, acquisition of data, data analysis, and interpretation of data. RJF and DQT participated in the planning, conception, design, data analysis, and interpretation of data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.