Article Text

Abstract
Background With growing numbers of older people worldwide, improving and maintaining quality of life during the extended years of life are a major focus for healthcare providers and policymakers. Some studies have suggested frailty may be associated with worse quality of life.
Objectives To review the associations between frailty and quality of life among community-dwelling older people.
Methods A systematic literature search was performed using five databases for cross-sectional and longitudinal studies examining associations between frailty and quality of life among community-dwelling older people published in 2000 or later. Reference lists of relevant studies were also manually searched. Authors were requested for data for a meta-analysis if necessary. Meta-analysis was attempted for studies using the same frailty criteria and quality-of-life instrument. Methodological quality, heterogeneity and publication bias were assessed.
Results The systematic review identified 5145 studies, among which 11 cross-sectional studies and two longitudinal studies were included in this review. Meta-analysis including four cross-sectional studies using the Fried Phenotype and 36-Item Short Form Health Survey showed that those classified as frail and prefrail had significantly lower mental and physical quality-of-life scores than those classified as non-frail. High heterogeneity and possible publication bias were noted.
Conclusions This systematic review and meta-analysis has demonstrated the evidence of a consistent inverse association between frailty/prefrailty and quality of life among community-dwelling older people. Interventions targeted at reducing frailty may have the additional benefit of improving corresponding quality of life. More longitudinal analysis is required to determine this effect.
- QUALITY OF LIFE
- GERIATRICS
- AGEING
Statistics from Altmetric.com
Introduction
There are growing numbers of older people worldwide, as life expectancy has markedly increased over the past century, largely due to public health improvements.1 The numbers of older people are projected to keep increasing, as is the proportion in the population.1 In the UK, the proportion of people aged 65 years and over is expected to increase from 17% in 2010 to 23% in 2035, with similar increases in other EU member states.2 Increased longevity does not mean a happy old age. Quality of life among older people tends to decline as they age, partially due to having poorer health than younger people.3 As people age, they are at increased risk of developing more chronic medical conditions and physical disabilities, which may impair their quality of life. Although it is important to prevent or treat these medical conditions, the absence of these conditions is not necessarily the only determinant of quality of life. Besides chronic diseases and physical impairment, psychological and social problems, such as depressive symptoms, isolation and loneliness, are also common among older people, especially the oldest old and lower socioecomonic groups.3–6 All these may potentially have detrimental and negative impacts on quality of life, and should also be addressed for successful ageing. Low quality of life among older people has been shown to be associated with various negative health outcomes, including falls, nursing home placement and mortality.7–9 In these circumstances, improving and maintaining quality of life during the extended years of life and facilitating successful ageing have been a major focus for healthcare providers and policymakers.10 ,11
Quality of life is a broad-ranging concept, affected in a complex way by a person's physical health, psychological state, personal beliefs, social relationships and their relationship to salient features of their environment.12 It is defined by WHO as ‘an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns’.12 In this context, older people's quality of life can be increased and maintained at a high level, even with poor physical health, as long as they are satisfied with other dimensions of quality of life, such as mental health, social and environmental relationships, and socioeconomic status.13
A possible link has recently been reported between quality of life and frailty.14 Frailty is a clinical syndrome of decreased physiological reserve, due to an age-related accumulation of multidimensional deficits.15 ,16 Prevalence of frailty has been reported to vary substantially ranging from 4.0% to 59.1% and the overall weighted prevalence was 10.7% according to a systematic review paper.17 Frailty can exhibit various signs and symptoms including weight loss, fatigue, weakness, impaired walking performance, low levels of physical activity, a depressed mood, and cognitive impairment.15 ,16 ,18 Furthermore, frail older people are highly susceptible to adverse health outcomes, such as falls, disabilities, institutionalisation, hospitalisation and death.15 ,16 ,18 ,19 All these factors may negatively affect quality of life. Compared with these well-studied outcomes, associations between frailty and quality of life have only recently started to be investigated and evidence is still scarce. Although a number of (mainly cross-sectional) studies have shown that frailty is associated with a lower quality of life among community-dwelling older people, there has been no systematic review study published in the literature. Therefore, how consistent the associations are across the studies, or how much degree of differences in quality of life exists according to frailty are still largely unknown.
The objectives of this study were to systematically review the literature for cross-sectional and prospective studies on associations between frailty and quality of life among community-dwelling older people, and to conduct meta-analysis and combine available evidence to synthesise pooled estimates.
Methods
This systematic review study was conducted according to a protocol developed based on the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement.20
Data sources and search strategy
A systematic literature search was performed in July 2015 using EMBASE, MEDLINE, CINAHL Plus, PsychINFO and the Cochrane Library for studies published from 2000 through current without language restriction by one investigator (GK), according to the predefined review protocol. The search terms used included (Quality of Life (Medical Subject Heading (MeSH)) OR (Health Status (MeSH)) OR (Health Survey (MeSH)) OR (Health Status Indicator (MeSH)) OR (Questionnaires (MeSH)) OR (General Health Questionnaire (MeSH)) OR (General Health Status Assessment (MeSH)) OR (Health Assessment Questionnaire (MeSH)) OR (Health Perceptions Questionnaire (MeSH)) OR (Mental Health (MeSH)) OR (Patient Health Questionnaire (MeSH)) OR (Well-being (MeSH)) OR (Spiritual Well-being (MeSH)) OR (Psychological Well-being (MeSH)) OR (quality of life) OR (QOL) OR (HRQOL) OR (HRQL) OR (well being*) OR (wellbeing*) OR (health status) OR (health status indicator*) OR (health survey*) OR (questionnaire*) AND (frailty) with an explosion function if applicable. Reference lists of relevant and included studies were also manually searched. Authors were contacted for data necessary for a meta-analysis.
Study selection
Cross-sectional or prospective cohort studies examining the associations between frailty and quality of life among community-dwelling older people aged 60 years and older, or with a mean age of 70 years and older, were eligible. Frailty should be defined by validated criteria or modified versions. Studies were excluded if they were review articles, randomised controlled trials, dissertations, or conference abstracts, or used only components or subdomains of frailty criteria (eg, gait speed) instead of multidimensional frailty. If the same cohort was used by multiple articles with the same study design (cross-sectional or prospective), the one with the largest number of participants was included.
Data extraction
The data collected from each of the included articles were the study type (cross-sectional study or prospective cohort study), first author, the name of the study or cohort if any, publication year, location, sample size, proportion of female participants, age (mean and range), frailty criteria, quality of life tool and the relevant findings.
Methodological quality assessment
The cross-sectional studies considered as eligible for meta-analysis were further assessed for methodological quality using six criteria from guidelines developed by Loney et al21 for critically appraising studies of prevalence or incidence of a health problem. The methodology of each study was considered to be adequate to be included in the meta-analysis if the study met three or more criteria out of the six.
Statistical analysis
Meta-analysis was attempted for the studies which used the same frailty criteria and quality of life instrument, and presented mean quality of life scores according to frailty categories. Heterogeneity across the studies was examined using χ2 test. The degree of the heterogeneity was assessed using I2 statistic. I2 values of 25%, 50% and 75% were considered as low, moderate and high heterogeneity, respectively.22 Pooled mean quality of life differences between frail and robust participants, and between prefrail and robust participants, were calculated using random-effects models when heterogeneity was high and fixed-effects models when heterogeneity was moderate or low. Publication bias was examined using Begg-Mazumdar's and Egger's tests, and by visual inspection of funnel plots. Statistical analyses were conducted using Review Manager 5 (V.5.2., Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration) and StatsDirect (Cheshire, UK). All analyses were two sided, and p<0.05 was considered as statistically significant.
Results
Selection processes
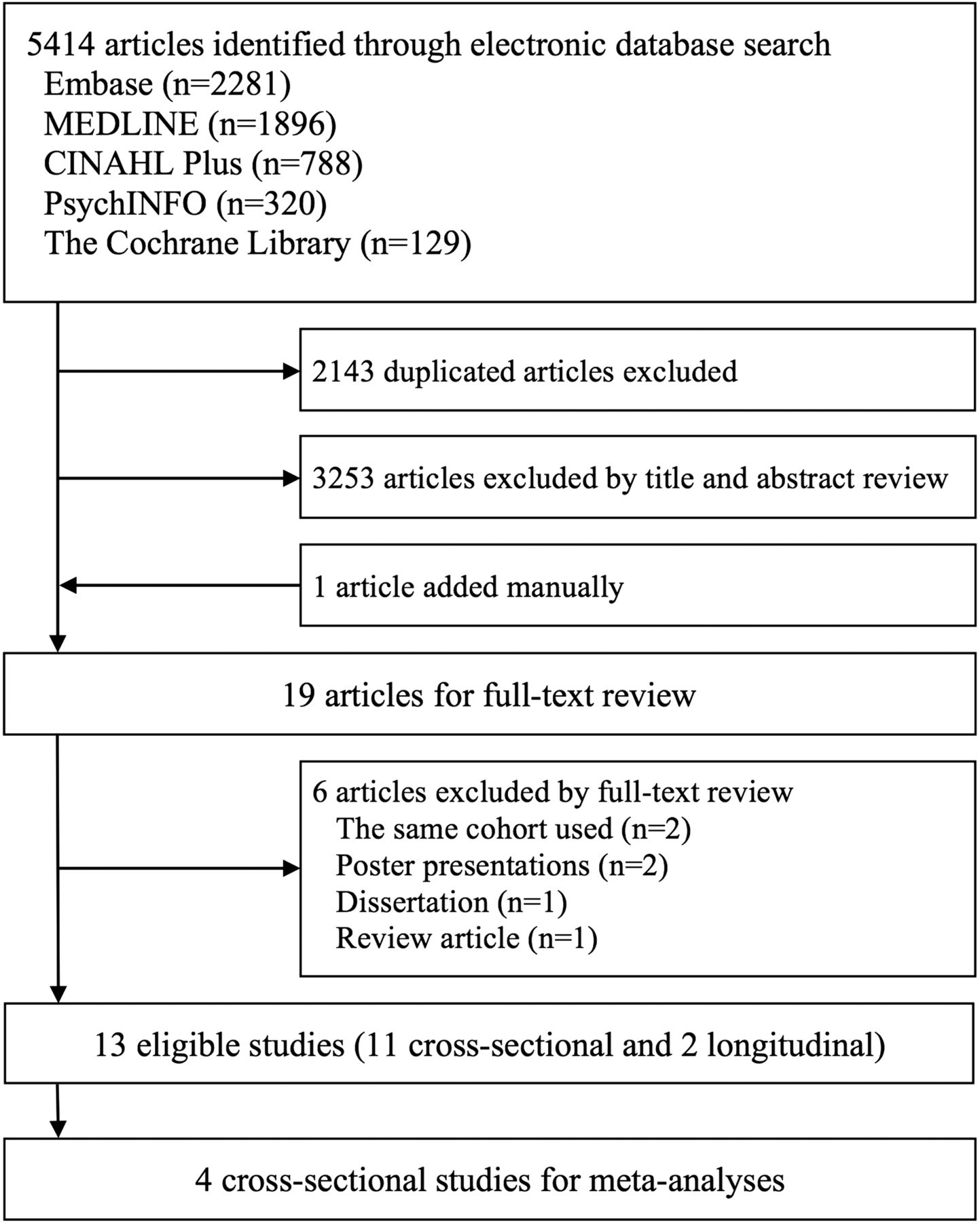
The electronic literature search used five databases: EMBASE, MEDLINE, CINAHL Plus, PsychINFO and the Cochrane Library. It yielded a total of 5414 studies. From these, 2143 duplicate studies and 3253 studies not considered eligible for this systematic review through the title and abstract review were excluded, and one study was added from the manual search, leaving 19 articles for the full-text review. Of these, six studies were considered ineligible for using the same cohort (n=2), being poster presentations (n=2), a review article (n=1) and a dissertation (n=1). One study examined associations between quality of life and five components of the Fried frailty criteria separately, instead of categorised frailty status (frail, prefrail and robust), and was therefore initially considered to be ineligible for this review.23 However, additional data were provided by the authors on request, and this study was included.23 A total of 13 articles (11 cross-sectional studies14 ,23–32 and 2 prospective studies33 ,34) were included in this systematic review, among which four cross-sectional studies compared quality of life measured by 36-Item Short Form Health Survey (SF-36) across three frailty categories: frail, prefrail and robust, as defined by the Fried criteria14 ,23 ,28 ,31 were included for the meta-analysis. A PRISMA flowchart of the study selection is presented in figure 1.

Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow chart of study selection.
Study characteristics and findings
Characteristics and findings of the included 11 cross-sectional14 ,23–32 and 2 prospective studies33 ,34 are summarised in online supplementary table S1. Three articles are from Taiwan,27 ,28 ,31 two each from Canada,29 ,30 the UK,25 ,33 Italy23 ,32 and the Netherlands,26 ,34 and one each from Germany24 and the USA.14 Sample sizes ranged from 8329 to 5703.30 The English Longitudinal Study of Ageing cohort was analysed by two studies, one cross-sectionally25 and one prospectively.33 Gobbens et al26 ,34 likewise published two papers (cross-sectional and longitudinal) from the same cohort in the Netherlands.
The proportion of female subjects ranged from 33.2% to 78.3%. Mean age was in the 70s in most studies, though up to the early 80s in some. Frailty was defined variously, including the Fried criteria,14 ,23 ,28 ,29 ,31 ,33 Frailty Index (FI),25 ,29 ,30 the Tilburg Frailty Indicator,26 ,34 the Study of Osteoporotic Fractures frailty index,32 and the Canadian Study of Health and Aging Clinical Frailty Scale.27 One study defined frailty based on a combination of three different criteria.29 The instruments used to measure quality of life also varied across the studies, including SF-36, 12-Item Short Form Health Survey (SF-12), CASP-19, EUROHIS-8, WHOQOL-BREF, Quality of Life Systemic Inventory questionnaire, Older People's Quality of Life questionnaire, and Ryff Psychological Well-being scale. Different methodologies were used to examine the associations between frailty and quality of life. Frailty was either divided into subgroups or described as a continuous variable. Quality of life was described as a continuous variable, often along with subdomains, such as physical health or mental health, etc. Despite a wide range of frailty definitions and quality of life instruments with different statistical analytic methodologies across all 11 cross-sectional studies, worse frailty status was consistently shown to be associated with lower levels of quality-of-life measures. Two prospective studies were identified in the present systematic review.33 ,34 Gobbens et al34 demonstrated significant correlations between frailty, as defined by the Tilburg Frailty Indicator, and future quality of life, based on WHOQOL-BREF 1 and 2 years later in 479 older people in the Netherlands. The other study,33 involving 2557 British older men and women in the community, showed better quality of life, measured using CASP-19, was associated with a lower risk of being frail (relative risk ratio=0.46, 95% CI 0.40 to 0.54) and prefrail (relative risk ratio=0.69, 95% CI 0.63 to 0.77), defined by the Fried criteria over 4 years.
Meta-analysis
Four cross-sectional studies14 ,23 ,28 ,31 using the Fried criteria and SF-36 were included in the meta-analysis. These studies were assessed for methodological quality,21 and all the studies met at least three criteria out of six, and were included in the meta-analysis. No other studies used the same combination of frailty assessment and quality-of-life measure, and were suitable for inclusion in a meta-analysis.
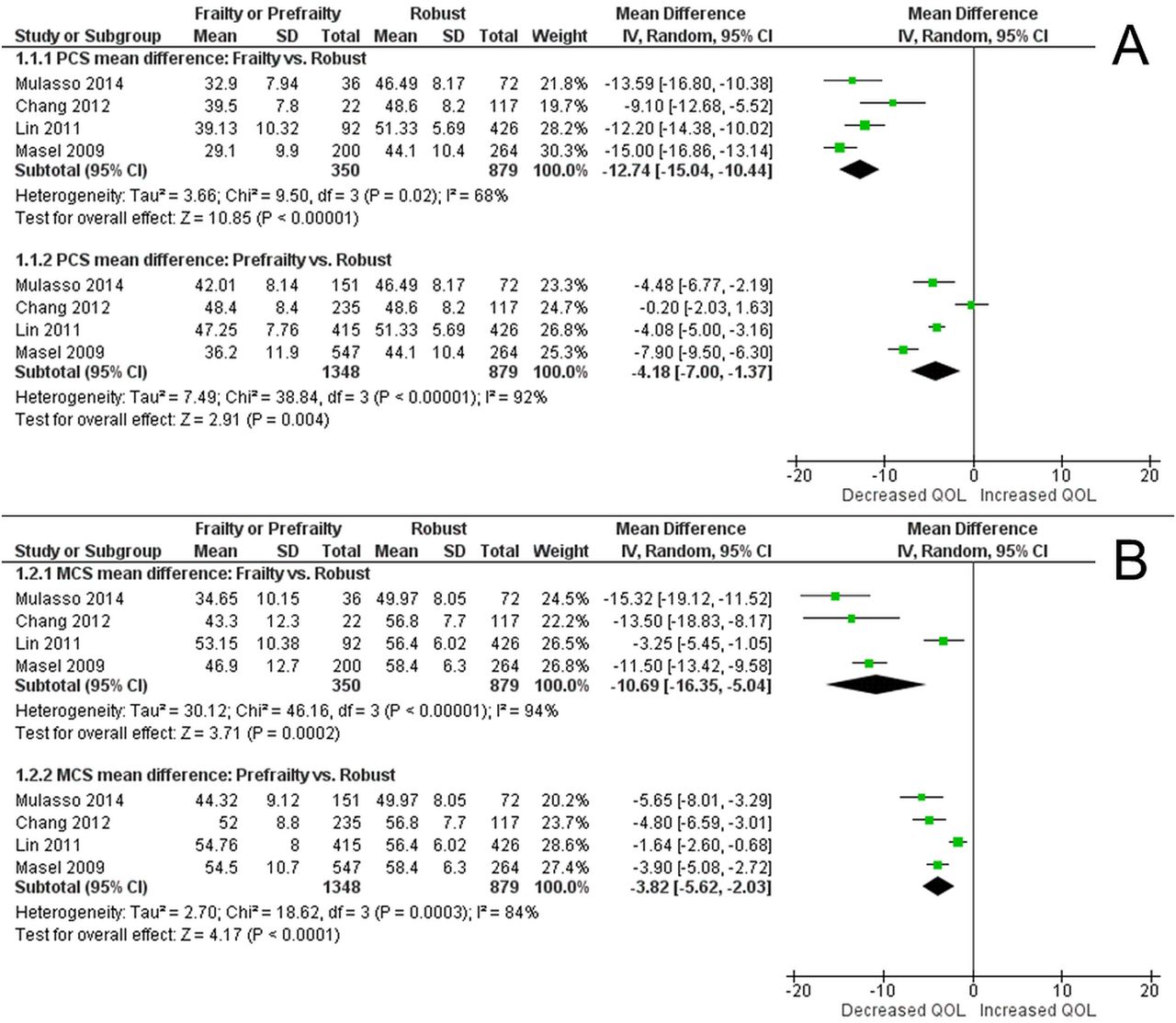
Mean scores of physical component summary (PCS) and mental component summary (MCS) with SDs and the number of participants for each of three frailty categories: frail, prefrail and robust, were extracted from these studies14 ,28 or obtained from the authors on request,23 and used to synthesise pooled mean differences. One study only reported adjusted mean scores.31 Unadjusted mean scores were obtained from the authors and used for the meta-analyses. Random-effects models were used for all meta-analyses due to high heterogeneity (all p values <0.05, I2=68–94%). Forest plots are shown in figure 2A, B. For PCS, pooled mean differences were −12.74 (95% CI −15.04 to −10.44, p<0.00001) for frail subjects, and −4.18 (95% CI −7.00 to −1.37, p=0.004) for prefrail participants, compared with robust participants, respectively. Likewise for MCS, pooled mean differences were −10.69 (95% CI −16.35 to −5.04, p=0.0002) and −3.82 (95% CI −5.62 to −2.03, p<0.0001) compared with robust participants, respectively. We could not conduct sensitivity or subgroup analyses due to a small number of the studies included.
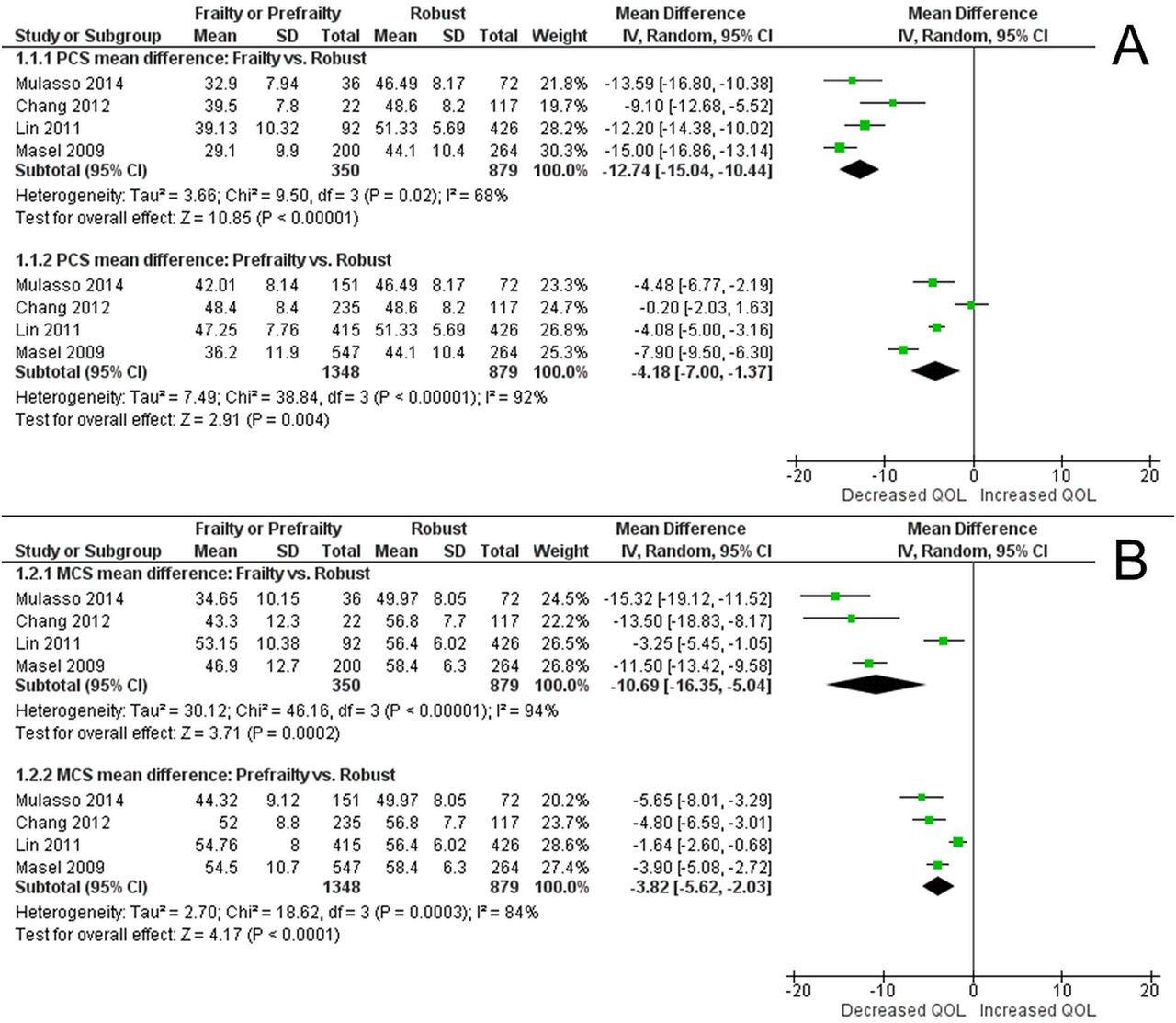
Forest plots of 36-Item Short Form Health Survey (SF-36) physical component and mental component summaries mean differences between frail/prefrail and robust older people. (A) SF-36 Physical Component Summary mean difference, (B) SF-36 Mental Component Summary mean difference.
Publication bias assessment
No evidence of publication bias was noted in three (PCS frailty vs robust, PCS prefrailty vs robust, and MCS frailty vs robust) of four meta-analysis models using Begg-Mazumdar's and Egger's tests (all p values >0.05). Publication bias was suggested in the meta-analysis of MCS mean difference between prefrailty versus robust (p<0.0001 by Begg-Mazumdar's test, p=0.0476 by Egger's test). Funnel plots for four meta-analyses are illustrated in figure 3A–D. Although it was difficult to interpret precisely since only four studies were included, visual inspection of the funnel plots of C (MCS between frailty vs robust) and D (MCS between prefrailty vs robust) suggests asymmetry with more studies plotted on more negative effect measure side.

{kind=link}
{kind=link}
{kind=link}
Funnel plots for quality of life mean difference between frail/prefrail and robust older people. (A) Physical component summary (PCS) frailty versus robust, (B) PCS prefrailty versus robust, (C) mental component summary (MCS) frailty versus robust, (D) MCS prefrailty versus robust.
Discussion
This systematic review identified 11 cross-sectional and 2 prospective studies examining associations between frailty and quality of life in community-dwelling older people. The meta-analysis including four cross-sectional studies demonstrated that both frail and prefrail older people defined using the Fried Phenotype14 ,23 ,28 ,31 had significantly worse quality of life compared with robust older people.
All the 11 cross-sectional studies identified in this systematic review consistently showed an association between frailty and worse quality of life, regardless of the different frailty criteria and quality-of-life tools used. The most commonly used frailty criteria was the Fried Phenotype, which mainly focuses on physical components associated with frailty: unintentional weight loss, self-reported exhaustion, weakness, slow walking speed and low physical activity.18 Therefore, it may seem natural that the physical component quality-of-life summary of frail participants would be worse than those classified as robust, based on the Fried criteria. The mental component quality-of-life summary was also much worse, almost to the same degree, among the frail than the robust participants. It can be speculated that frailty, even if defined mainly physically, can have significant effects on the mental components of quality of life, and that incorporating psychological and mental factors may improve the validity of frailty criteria.35 Furthermore, there appeared to be a ‘dose–response’ relationship: those with frailty had a substantially lower quality of life in both physical (−12.7) and mental (−10.7) domains in our meta-analysis, and those with prefrailty had important but smaller reductions in both physical (−4.2) and mental (−3.8) domains of quality of life.
Causal relationships between frailty and quality of life cannot be inferred based on the findings of the cross-sectional studies. The present systematic review identified only two prospective studies. One study showed significant inverse correlations between frailty and subsequent quality of life 1 and 2 years later.34 The correlation coefficients between frailty and four quality-of-life domains ranged from −0.34 to −0.75. It should be noted that they failed to adjust these associations for important covariates, such as age, gender, education, or socioeconomic status, and that the findings may have been confounded. Another prospective study demonstrated that a higher baseline quality of life was protective against being prefrail (relative risk ratio (RR)=0.79, 95% CI 0.71 to 0.89) and being frail (RR=0.62, 95% CI 0.52 to 0.74) at 4-year follow-up, controlling for important covariates and baseline frailty status.33 Although more prospective studies are needed to enhance our understanding, the association between frailty and quality of life may possibly be bidirectional, based on these two prospective studies and the aforementioned cross-sectional studies, consistently showing inverse associations between frailty and worse quality of life. Those who are frail, or become frail, may experience a decline in their quality of life, which in turn is likely to worsen rather than improve their physical and mental health. Given that both frailty and quality of life are multidimensional concepts, future research should also investigate how components or subdomains of these two entities are associated.
A variety of quality-of-life instruments were used in the included studies. SF-36 was used by the four studies in our meta-analysis. Although SF-36 is one of the most widely used quality-of-life instruments in various populations and settings in the literature, it and most of the other generic instruments have not been developed or validated specifically for the elderly population, whose health, physical status and perspectives are likely to be different from the younger population. Physical functions are often especially impaired among older people, and their quality of life measured by non-old-age-specific instruments may be compromised by overemphasising the physical function domain.36 Quality-of-life measures specifically for older people have recently been developed.37 These measures include CASP-19,38 WHOQOL-OLD,39 and the Older People's Quality of Life questionnaire,40 and these were used by some of the included studies.25 ,27 ,32 ,33
Our results should be interpreted with caution. Although a total of 11 cross-sectional studies were identified through the systematic review of the literature, only four studies could be incorporated in the meta-analysis because of the wide array of tools used to measure quality of life across the studies. Furthermore, sensitivity or subgroup analyses could not be performed due to the small number of the included studies.
One of this study's strengths is that this is, to the best of our knowledge, the first systematic review and meta-analysis study reporting the associations between frailty, prefrailty and quality of life among community-dwelling older people. Another strength is the extensive and reproducible systematic literature search, using comprehensive search terms in the five electronic databases, plus a manual search of the relevant articles’ reference lists. We also contacted authors to identify further potentially eligible studies for the meta-analysis, and were eventually able to add one study,23 with additional data provided by the authors on request. Regarding the four studies included in the meta-analysis, methodological quality was assessed and secured, and possible publication bias was suggested.
Conclusion
This systematic review and meta-analysis has demonstrated the first evidence of a consistent inverse association between frailty, prefrailty and quality of life among community-dwelling older people. Frailty and prefrailty defined by the physical phenotype were significantly associated with both worse physical components and mental components of quality of life, compared with those defined as robust. Interventions targeted at reducing frailty may have the additional benefit of improving corresponding quality of life.
What is already known on this subject
With growing numbers of older people worldwide, improving and maintaining quality of life during the extended years of life are a major focus for healthcare providers and policymakers.
Although some studies have suggested that frailty may be associated with worse quality of life, their findings were mixed and inconsistent.
The objectives of this study were to systematically review the literature for the associations between frailty and quality of life among community-dwelling older people, and to conduct meta-analyses to combine available evidence to synthesise pooled estimates.
What this study adds
This systematic review and meta-analysis has demonstrated the first evidence of a consistent inverse association between frailty, prefrailty and quality of life among community-dwelling older people.
Interventions targeted at reducing frailty may have the additional benefit of improving corresponding quality of life.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors GK designed the study and performed systematic review and meta-analysis. GK, SI, SJ and KW interpreted the data. GK drafted the manuscript. All authors revised the manuscript critically for important intellectual content, read and approved the final manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.