Article Text

Abstract
Background It is unknown whether the risk of preterm birth (PTB) is elevated for forced (refugee) international migrants and whether prolonged displacement amplifies risk. While voluntary migrants who arrive from a country other than their country of birth (ie, secondary migrants) have favourable birth outcomes compared with those who migrated directly from their country of birth (ie, primary migrants), secondary migration may be detrimental for refugees who experience distinct challenges in transition countries. Our objectives were (1) to determine whether refugee status was associated with PTB and (2) whether the relation between refugee status and PTB differed between secondary and primary migrants.
Methods We conducted a retrospective population-based cohort study. Ontario immigration (2002–2010) and hospitalisation data (2002–2010) were linked to estimate adjusted cumulative odds ratios (ACOR) of PTB (22–31, 32–36, 37–41 weeks of gestation), with 95% CIs (95% CI) comparing refugees with non-refugees. We further included a product term between refugee status and secondary migration.
Results Overall, refugees (N=12 913) had 17% greater cumulative odds of short gestation (ACOR=1.17, 95% CI 1.07 to 1.28) compared with non-refugees (N=110 640). Secondary migration modified the association between refugee status and PTB (p=0.007). Secondary refugees had 58% greater cumulative odds of short gestation (ACOR=1.58, 95% CI 1.25 to 2.00) than secondary non-refugees, while primary refugees had 12% greater cumulative odds of short gestation (ACOR=1.12, 95% CI 1.02 to 1.23) than primary non-refugee immigrants.
Conclusions Refugee status, jointly with secondary migration, influences PTB among migrants.
- MIGRATION
- PREGNANCY
- PERINATAL EPIDEMIOLOGY
- SOCIAL EPIDEMIOLOGY
Statistics from Altmetric.com
Migration is a key social determinant of health.1 Migrant health is associated with a spectrum of experiences ranging from ‘voluntary’ to ‘forced’ migration.2 Yet migration is often a multistep process. Previous research has found that women who voluntarily migrate to a transition country before migrating to Canada (ie, secondary migrants) have a lower risk of preterm birth (PTB) compared to women who voluntarily migrate directly from their country of birth (ie, primary migrants), and further suggested that lower risk may be related to the upwardly mobile socioeconomic profiles of the former group.3 However, in the case of refugees, departure from their country of birth is most often forced because of persecution, war or violence.4 In 2013, refugees numbered 16.7 million globally.4 Refugees’ migration experiences may be arduous and prolonged, including residence in one or more transition countries in the hopes of finding safe haven along the way. It is estimated that refugees are spending an average of 17 years awaiting a resolution to exile.5 Such journeys may compound stress experienced by refugees in their home countries through further marginalisation in transition countries since they are often denied the right to work and live in security.6 We hypothesise that refugee status (ie, refugee immigrants vs non-refugee immigrants, henceforth referred to as ‘refugees’ and ‘non-refugees’, respectively) is associated with negative health impacts and that secondary migration further exacerbates risk.
PTB is a leading predictor of perinatal morbidity and mortality, and increases risk for a number of adverse health outcomes over the life course.7 ,8 PTB is also particularly sensitive to social disadvantage. Studies have identified persistent disparities in PTB based on race9 ,10 as well as steep gradients based on income, education and occupation in the USA11 and other industrialised countries.12 ,13 Studies examining disparities by refugee status are mixed.14–16 The mechanism by which social disadvantage increases risk of PTB is not well understood, but there has been increasing interest in the role of psychosocial stressors.17 Our objectives were to determine if (1) the risk of PTB differed between refugees and non-refugees and (2) the relation between refugee status and PTB differed depending on whether women experienced secondary or primary migration.
Methods
Study design and participants
This was a population-based retrospective cohort study. We used the Citizenship and Immigration Canada Permanent Resident Database (CICPRD) (described below) to identify the refugee status of women who immigrated to the province of Ontario, Canada, and received permanent residency between 1 April 2002 and 31 December 2010. Women who were <15 years old at the time of arrival were excluded. All women included in this study were eligible for provincially funded healthcare insurance. All singleton infants born in an Ontario hospital to immigrant women between 1 April 2002 and 31 March 2011 were included. Multiple deliveries were excluded given different reasons for PTB among multiples,7 as were births 18–21 weeks of gestation, or with birth weights <500 g.
Data sources
Two administrative databases were linked to conduct this study. The CICPRD, administered by the Canadian Government, contains information on refugee status, date of permanent residency, country of birth (COB), country of last permanent residence, education level and knowledge of Canadian official languages (English and French) upon arrival to Canada. The Discharge Abstract Database (DAD) contains paired maternal and infant hospital admission records. Gestational age (GA) at the time of birth contained in the DAD was used to identify newborns born preterm. This dataset also contains information on maternal age at the time of delivery and number of previous live births.
Variables
The main exposure examined was refugee status, whereby refugees were compared with non-refugees. Refugee status was objectively determined in the CICPRD based on the immigration category following evaluation of the applicants’ legal documentation. The definition of refugees in the CICPRD was consistent with the United Nations Convention Relating to the Status of Refugees (1951), which stated that refugees are persons who cannot return to their home country due to a well-founded fear of persecution based on race, religion, political opinion, nationality or membership in a particular social group. Non-refugees were immigrants who did not have refugee migration histories.
The outcome measure, PTB, was defined as any birth <37 weeks GA. However, since infant health outcomes and survival differ across the range of preterm GA and diverse causal mechanisms are implicated, the investigation of PTB subtypes based on GA has been recommended.10 In recognition of this, PTB was operationalised as a three-category outcome: very preterm (22–31 weeks), moderate preterm (32–36 weeks) and full term (37–41 weeks). GA (in completed weeks) incorporates the best clinical estimate in the medical chart, based mostly on early ultrasound measurements.18 Canadian guidelines suggest that pregnant women should be offered prenatal dating ultrasound in the first (preferred) or second trimester.18 In Ontario, approximately 95% of pregnant women had their first prenatal ultrasound before 20 weeks of gestation.19
The effect modifier of interest was secondary migration.20 Secondary migrants resided in a country (regardless of their legal status) other than their COB for ≥ 6 months in the 5 years prior to immigration to Canada. This country is referred to as a transition country, or the country of last permanent residence. Secondary migrants satisfied the above criteria while primary migrants resided in their COB in the 5 years prior to immigration to Canada. See online supplementary figure S1 for an illustration.
The covariates in this study included maternal COB (a contextual variable,21 incorporated as a random intercept) and world regions of birth (used to investigate a potential three-way interaction analysed in further subgroup analyses). The United Nations country classification system was used to categorise the COB into world regions.22 Maternal age at delivery, number of previous live births, education at the time of arrival, knowledge of official languages, and duration of residence were considered potential confounders identified a priori.
Analytic methods
Descriptive analyses were conducted to examine the distribution of categorical covariates and means and SDs for continuous covariates by refugee status, and further stratified by secondary migration status.
Risks (per 100 singleton live births) were estimated for very and moderate PTB according to refugee status, and further stratified by secondary migration status. Results were graphed to visualise differences in risk according to secondary migration.
Generalised linear mixed models with maximum-likelihood estimation techniques,23 were used to estimate the unadjusted and adjusted cumulative OR24 (ACOR) and 95% CI for very and moderate PTB, among refugees compared with non-refugees. An ordinal model more effectively models the severity of health outcomes which increase with earlier GA.10 ,24 A second model containing a product term between refugee status and secondary migration further assessed effect modification of the main association by secondary migration. Models were adjusted for maternal age, number of previous live births, education level, language ability, and duration of residence in Canada.
COB has been identified as an essential indicator of the perinatal health of migrants,25 suggesting similarity (non-independence) in the perinatal health of women from the same country. As such, we accounted for non-independence by testing the significance of a random intercept for COB in an intercept-only model. If significant non-independence was found, we kept the random intercepts to obtain more accurate SEs. Further, the intraclass correlation coefficient was calculated to estimate the proportion of total variation in PTB that is explained by variation at the group level (COB).21 The intraclass correlation coefficient was interpreted as the average correlation in risk of PTB among women from the same COB.21
The proportional odds assumption for cumulative probability models was examined using the Score Test, where not rejecting the null hypothesis (p≥0.05) suggests that the proportionality assumption was met and that the single estimate from the cumulative probability model fits the data better than two logits.24
This study received research ethics approval from (1) Sunnybrook Health Sciences Centre (2) St Michael's Hospital and (3) The University of Toronto.
Results
This study included 100 894 singleton births to primary non-refugees, 11 618 births to primary refugees, 9746 births to secondary non-refugees, and 1295 births to secondary refugees. Additional descriptive characteristics of the study population are summarised in table 1. Figure 1 indicates that the risk of very and moderate PTB (per 100 singleton live births) were similar for all refugees and non-refugees as well as all primary refugees and primary non-refugees. However, there was a substantial difference between secondary refugees and secondary non-refugees, for both very PTB (1.2 vs 0.6, respectively) and moderate PTB (5.9 vs 4.4).
Characteristics for singleton live births (Ontario, Canada, 2002–2010) to primary non-refugee, primary refugee, secondary non-refugee and secondary refugee women who became permanent residents in Ontario between 2002 and 2010
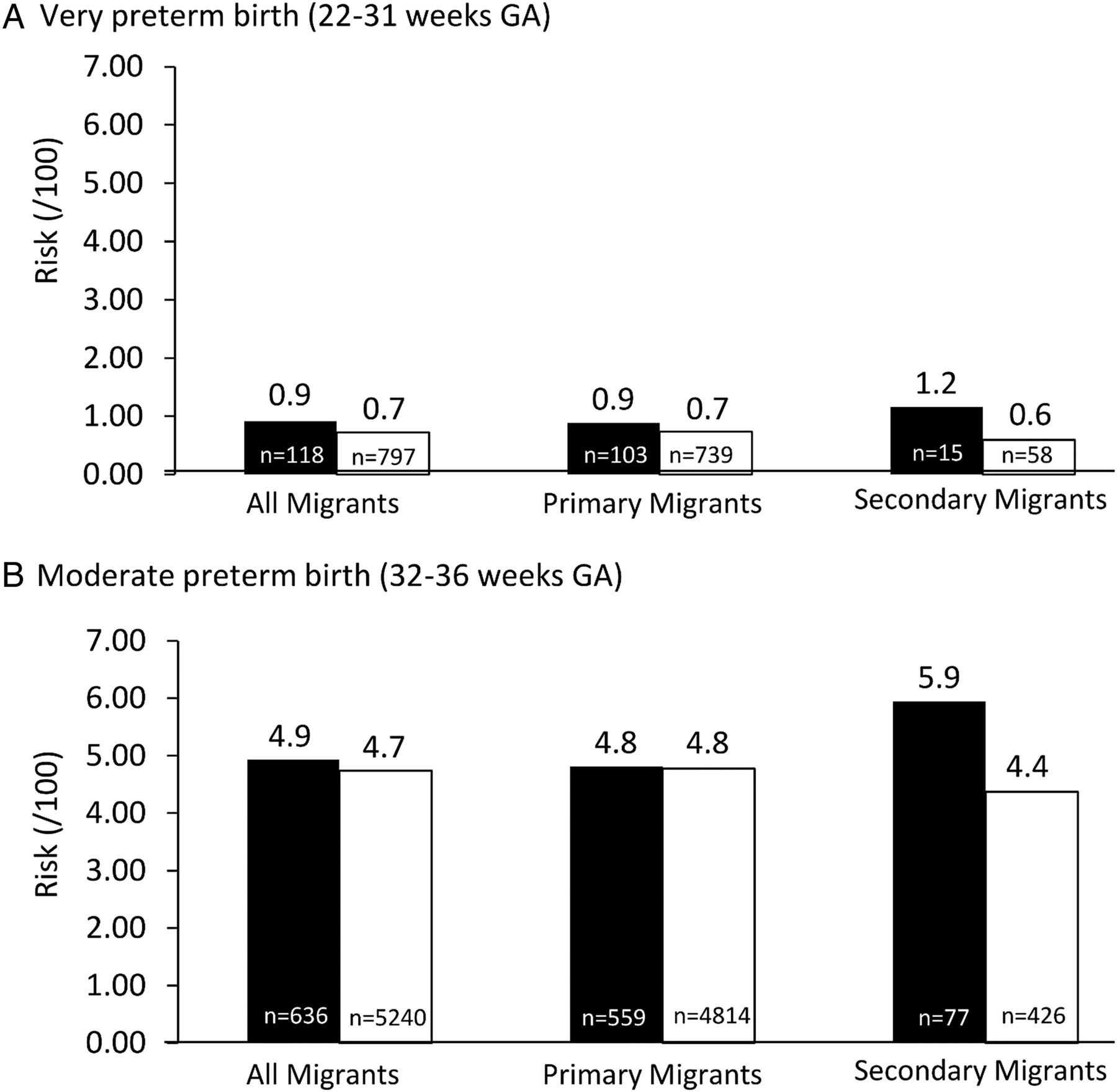
Number (n) and risk (per 100 singleton live births) of very and moderate preterm birth (2002 to 2010) to refugees (black squares), and non-refugees (white squares)—all migrants (N=123 524), primary migrants (N=112 484) and secondary migrants (N=11 040) who became permanent residents in Ontario, Canada, between 2002 and 2010. GA, gestational age.
For cumulative odds models, the random intercept coefficient for COB was statistically significant (covariance parameter estimate =0.050, SE =0.013) resulting in an intraclass correlation coefficient of 1.51%, suggesting minimal similarity in the cumulative odds of PTB among women born in the same country. In addition, the proportionality assumption was satisfied (p=0.10).
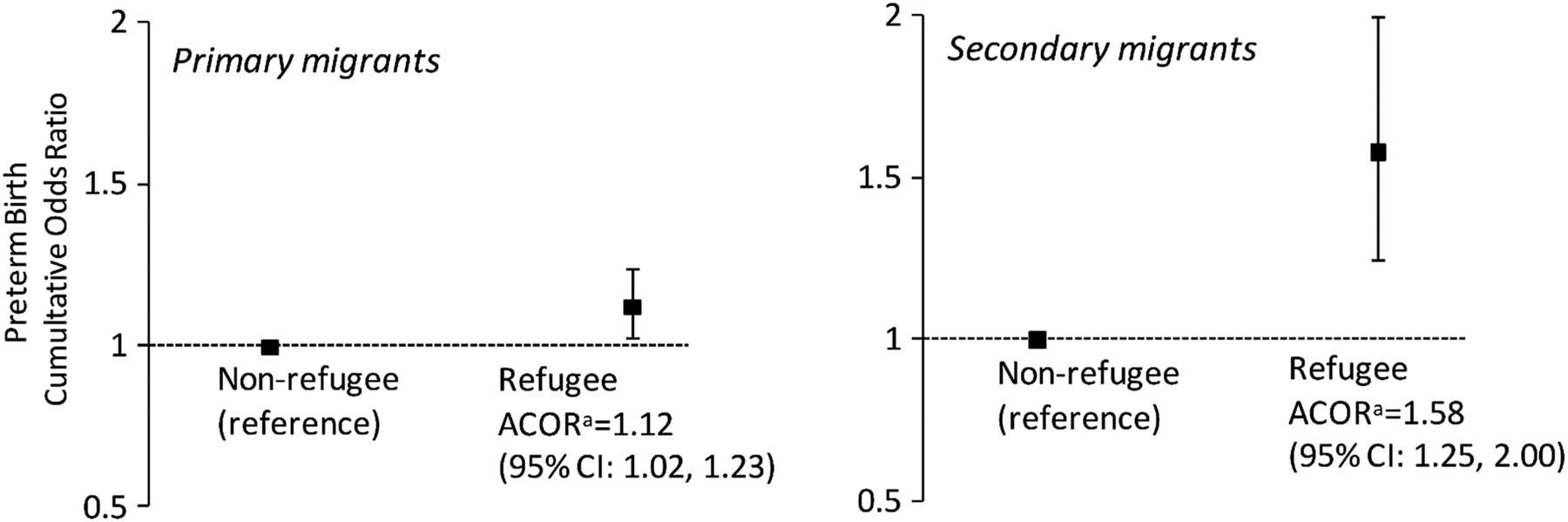
Overall, refugees had 17% greater cumulative odds of PTB compared with non-refugees, after adjustment (ACOR=1.17, 95% CI 1.07 to 1.28). Furthermore, there was a significant interaction between refugee status and secondary migration (p=0.0073). Figure 2 depicts a 12% increase in the cumulative odds of short gestation for primary refugees compared with non-refugees (ACOR=1.12, 95% CI 1.02 to 1.23), and a much larger 58% increase in the cumulative odds of PTB for secondary refugees compared with secondary non-refugees (ACOR=1.58, 95% CI 1.25 to 2.00).

{kind=link}
{kind=link}
Adjusted cumulative ORs and 95% CI for preterm birth in Ontario, Canada (2002–2010), according to refugee status (refugee vs non-refugee migrants, consisting of those who became permanent residents in Ontario, Canada, between 2002 and 2010), stratified by secondary migration (significant effect modification (p=0.0073)). Random intercept for maternal country of birth included, adjusted for maternal age, number of previous live births, education at arrival, knowledge of official languages at arrival and duration of residence. ACOR, adjusted cumulative OR.
In secondary analyses, including a three-way product term with maternal regions of birth did not further modify the relationship (p=0.22).
Discussion
Refugees experienced greater odds of PTB compared with non-refugees, with secondary refugees experiencing much larger excess odds than primary refugees. The 58% increased odds of PTB experienced by secondary refugees is of a magnitude comparable to known strong risk factors for PTB such as smoking and bacterial vaginosis (RR≈1.5–2.0).26
The impact of secondary migration among refugees has been largely unexplored. One qualitative study included Burundian and Liberian refugee families who undertook secondary migration within the USA.27 Families cited numerous impacts of secondary migration including loss of support of local agencies and ethnic and religious communities but also increased family solidarity and neighbourhood safety. These experiences, particularly in terms of opportunities contrasting with supports that are lost, may be generally similar for international secondary refugee migrants. However, these findings may not be generalisable to our study population in that most secondary refugees’ transition countries were not industrialised (see table 1) and were, therefore, unlikely to have resources to promote refugee integration. In fact, many host populations are reportedly hostile to refugee populations28 and actively prevent integration.
This study makes three contributions. First, to our knowledge, this is the first study with sufficient statistical power to identify refugee status as a significant risk factor for PTB. Second, this is the only study to demonstrate the strongly modifying effect of secondary migration on the relationship between refugee status and PTB. Finally, our findings suggest that the healthy migrant effect is experienced by primary but not secondary refugees, since the PTB rate among primary refugees compares favourably to Canadian-born women (5.0% and 6.4%,29 respectively), while that of secondary refugees does not (7.1%).
A large population-based immigration dataset was used, with objectively ascertained information on legal refugee status and sociodemographic characteristics. The population-based hospital admission data included nearly all immigrant births taking place in the province of Ontario during the study period. There was a very low proportion (<1%) of missing values for most variables in both databases. Last, healthcare is universally available to all permanent residents and Canadians citizens in Ontario, ensuring that cost is not a prohibitive factor for hospital birth.
Sensitivity analyses were conducted to assess potential modelling limitations. First, we replaced the maternal COB random intercept with regions of birth (as a categorical fixed effect) to assess the potential for non-normally distributed random effects. Both effect estimates and SEs were somewhat reduced using regions, suggesting that even if the random intercept was inappropriately included, the study conclusions remain the same. We also determined that the findings were not driven by over-representation of mothers from a specific COB. Studies of Somali immigrant women in several industrialised countries suggest a higher risk of some perinatal outcomes compared with native-born women.30 Online supplementary table S1 indicates that Somali women comprise ∼5% of both secondary and primary refugees with much smaller proportions among non-refugees. If Somali women in our study were at a substantially increased risk for PTB, this may explain some of the excess risk seen among refugees. However, results excluding Somali women were virtually identical to those reported. Possible heterogeneity among exposure groups was further assessed by restricting to countries represented in all four exposure groups (n=88). Contrasted with results from all countries (n=203), we found slightly increased risks among secondary refugees compared with both secondary non-refugees and primary refugees (68% and 34%, respectively). These analyses suggest that possible exposure group heterogeneity does not explain the increased PTB risk among secondary refugees.
This study has limitations. For the majority of births in this study, GA was measured by ultrasound in the first or second trimester. However, variation in GA by dating ultrasound increases from 3 to 5 days between 7 and 13 weeks to 1 week between 14 and 20 weeks.10 As such, there may be some misclassification of GA. However, differential misclassification of GA by refugee or secondary migration status is unlikely. Second, some control variables may be mediators, yet, considering minimal differences between unadjusted and adjusted estimates, any overadjustment appears negligible. Some secondary migrants may have lived in more than one other country in the 5 years prior to immigrating to Canada, but reported the most recent country during immigration. Additionally, primary migrants may have also lived in another country other than their COB in the distant past (≥5 years prior to immigration to Canada). Regardless, the secondary migration indicator captures those who experienced at least one migration event that lasted ≥6 months in the previous 5 years. Although we controlled for several sociodemographic factors, residual confounding may be present as we could not account for potential differences in social capital and wealth between primary and secondary refugees, where greater resources may contribute to a refugee's ability to flee to Canada (primary migration) directly rather than to a neighbouring country first (secondary migration). Also, we could not identify members of the same family, which may help reduce possible exposure misclassification by identifying a minority of women with refugee exposure who migrated as economic or family class immigrants. We did not have information on duration of residence in transition countries, which may highlight potential cumulative exposures in transition countries. Behavioural risk factor data was not available as well as various measures of psychosocial stress that may be important to clarify potential pathways as described in the next section. Finally, the results of this study are not generalisable to unsuccessful refugee claimants and other migrants without permanent residency. Lack of permanent residency status prohibits access to provincially funded healthcare insurance which has important implications for stress experienced by pregnant women.31 Stress resulting from lack of status may affect PTB differently than that described in this study.
Possible explanations for increased risk
Despite extensive research, the causes of PTB are not well understood,12 and few risk factors have been established.26 Many behavioural or biological risk factors (often related to material deprivation) are implicated in the risk of PTB among socially disadvantaged populations.26 Descriptive studies have shown that some of these risk factors, such as infections and malnutrition, are prevalent among refugees in Canada and the USA.32 ,33 However, it has also been suggested that these risk factors do not entirely explain increased risk of PTB among socially disadvantaged populations.27 ,34 It seems unlikely that the excess risk seen in our study can be completely attributed to these factors considering the often cited healthy behavioural profiles (ie, lower rates of smoking) of immigrant women in Canada.35 ,36 These factors may also be partially adjusted for in our study by maternal education, or considered through COB.
In light of the limited ability of behavioural risk factors to explain increases in PTB among socially disadvantaged populations, there has been increasing interest in psychosocial stress.7 ,10 ,17 ,26 Stress is defined as ‘demands that tax or exceed the adaptive capacity of an organism that result in psychological and biological changes’.26 The most consistent evidence is for major life events (eg, death in the family), exposure to chronic stress (eg, accumulation of stressors over the life course), maternal anxiety, racism, domestic or personal violence and unintended pregnancy.26 All these psychosocial risk factors may be disproportionately present among refugees,37–39 and may, in turn, be responsible for the generally increased risk of PTB among refugees we observed. A subtle difference between secondary and primary refugees is the time elapsed between departure from their COB and arrival in Canada, and how this may interact with psychosocial stress. Specifically, primary refugees’ experience of psychosocial stress may be attenuated by faster arrival in Canada while, for secondary refugees, psychosocial stress may be prolonged by a lengthier migration journey producing chronic stress. Chronic stress and a possibly weakened adaptive response12 ,40 (ie, coping skills) might help explain the substantially increased risk of PTB among secondary refugees. A large body of evidence suggests that maternal chronic stress contributes to increased risk of PTB through early initiation of hormonally induced events required for birth.40
Conclusion
Our results suggest that secondary migration may affect the health of voluntary and forced migrants in opposite ways. While migrants who voluntarily transition through intermediate countries have favourable birth outcomes, exposure to unplanned stay in a transition country seems to increase the risk of PTB among refugees.
Considering the magnitude of the elevated risk identified in this study, and the global population at risk (ie, approximately 3.15 million female refugees living in protracted situations at the end of 2013),4 more detailed data are needed to clarify the mechanisms behind our observed associations, including the influence of psychosocial stressors and other potentially mediating factors. Future studies may help inform the implementation of policies that reduce wait times in transition countries, and enhance healthcare and social services for pregnant women during displacement.
What is already known on this subject
International secondary migration is associated with good health among voluntary migrants.
Refugee experiences in transition countries (eg, refugee camps) may not be conducive to good health.
It is unknown what the risk of preterm birth (PTB) among refugees is, and whether it differs according to secondary migration status.
What this study adds
Overall, refugees have a slightly excess risk of PTB compared with non-refugee immigrants.
However, the gap is considerably amplified among secondary migrants.
Unlike among voluntary migrants, secondary migration exacerbates the risk of PTB among refugees.
Acknowledgments
The study was possible thanks to the Institute for Clinical Evaluative Sciences (ICES), which is supported by an annual grant from the Ontario Ministry of Health and Long-Term Care. The opinions, results and conclusions reported in this article are those of the authors, and are independent from the funding sources. No endorsement by ICES or the Ontario Ministry of Health and Long-Term Care is intended or should be inferred. Parts of this material are based on data and information compiled and provided by CIHI. However, the analyses, conclusions, opinions and statements expressed herein are those of the author, and not necessarily those of CIHI. MU holds a CIHR New Investigator Award.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors SW conceived the study, analysed the data and drafted the first version of the manuscript. MLU acquired funding and access to the data. All authors contributed to the interpretation of results, revised the manuscript, and approved the final version.
Funding The study was funded by a grant of the Canadian Institutes of Health Research.
Competing interests None declared.
Ethics approval (1) Sunnybrook Health Sciences Centre; (2) St Michael's Hospital; (3) The University of Toronto.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.