Article Text

Abstract
Background Taking antiobesity medication can be a cost effective way to lose weight. Uptake is determined in part by a General Practitioner's decision to prescribe weight loss medication and, in part, by patient preference. It is probable that the latter may indicate a patient's readiness to lose weight.
Methods Analysis of cross-sectional data (from February 2003 to March 2011) from a population based prescribing database (∼1.75 million people) using an adjusted Poisson regression.
Results The number of antiobesity medications increased from 23.4 per 1000 population in 2004 to 30.7 per 1000 population in 2010 and was three times higher in female than in male subjects. Against this background, a marked seasonal variation in the number of antiobesity medications dispensed was evident (p<0.001), peaking in June/July with a trough in December/January (±8.0% peak to trough). The seasonal component was stronger in female subjects, ±11.2% peak to trough, compared with ±3.5% for male subjects.
Conclusions Obese patients, particularly women, increase their uptake of weight loss medication in the months leading up to the summer holiday period. The period prior to the summer may represent a time that health professionals could promote increased participation of obese patients in weight loss programmes.
- obesity
- prescribing
- public health
Statistics from Altmetric.com
Introduction
Obesity is a major societal and public health problem.1 Recent data from the Health Survey for England have shown that the prevalence of obesity (defined as a body mass index (BMI) ≥30 kg/m2) exceeds 25% in both men and women.2 Current projections, based on data from 1993 to 2008, suggest that approximately 41% of UK men and 35% of UK women will be obese by 2030, representing an additional 11 million cases of obesity compared with 2010 levels.3 The healthcare costs associated with this are estimated at an additional £2 billion per year by 2030.3 Small reductions in average BMI across the population can produce large health gains; a 1% reduction in BMI across the UK population could avoid up to 202 000 incident cases of diabetes, up to 122 000 cardiovascular disease events and up to 33 000 incident cases of cancer.3 However, to achieve this, a multifaceted approach is required.4
In the UK, General Practitioners (GPs) are the main providers for obesity treatment,5 but the counselling required to achieve any long-term clinically meaningful weight loss is considerable.6 Advice from doctors is most effective when it coincides with a ‘teachable moment’,7 a concept which has been used in the acute setting by the National Health Service in Scotland so that ‘every healthcare contact is a health improvement opportunity’.8 Many such opportunities arise in primary care but they are often missed.9 In recent years, the consumption of antiobesity medication has increased, reflecting both its increased availability and to some extent patient preferences and a desire to lose weight.10 Therefore, an examination of variation in the number of prescriptions might indicate periods when patients are prepared to engage in weight reduction programmes. We hypothesised that the number of weight loss drug prescriptions might vary throughout the year, consistent with the recognised seasonal cycle in weight gain that often is not reversed during the spring and summer months and has a cumulative effect over time.11 ,12
The aim of this study was to investigate whether or not there was a seasonal trend in the number of prescriptions for antiobesity medication issued by GPs and dispensed by pharmacists.
Methods
Data on the monthly total number of antiobesity medications (orlistat (60 and 120 mg), rimonabant, sibutramine) prescribed and dispensed (new and repeat prescriptions) in Northern Ireland (NI) from February 2003 through to March 2011, for all age groups, were extracted from a centralised collection of GP prescriptions covering a population of approximately 1.75 million. Monthly counts were available by gender from 1 April 2008. The use of patient level data was approved by the Office for Research Ethics Committee NI (REC:10/NIR02/19).
Statistical analysis
A Poisson regression model was constructed for these monthly counts taking into account the population size (interpolated between mid-year population estimate; http://www.nisra.gov.uk/demography/default.asp17.htm) and the number of days in the month. The underlying long-term trend was captured using linear, quadratic and cubic terms in time. Seasonal variation was modelled by including sine and cosine terms which specified a sinusoidal pattern with one peak and one trough 6 months apart. The relative amplitude was estimated and expressed as peak to trough relative to the mean. The timing of the peak value was also identified. For the gender analysis, only linear and quadratic terms in time were included in the model. Data were analysed using SPSS V.17 (Chicago, Illinois, USA) and Stata release 11 (College Station, Texas, USA).
Results
The overall trend showed an increasing number of medications with an annual rate of 23.4 prescriptions per 1000 population in 2004 to 30.7 per 1000 population in 2010. The peak annual rate of prescribing occurred in 2007 with 43.0 prescriptions per 1000 population. In 2010, the annual rate of prescribing in male subjects was 14.2 per 1000 population compared with a rate of 41.6 per 1000 population in female subjects.
There was significant seasonal variation in the number of antiobesity medications dispensed (±8.0% with a late June/early July peak, p<0.0001; figure 1).

Monthly counts (adjusted for length of month) of antiobesity medication prescriptions (February 2003–March 2011) with fitted long-term trend and seasonal variation.
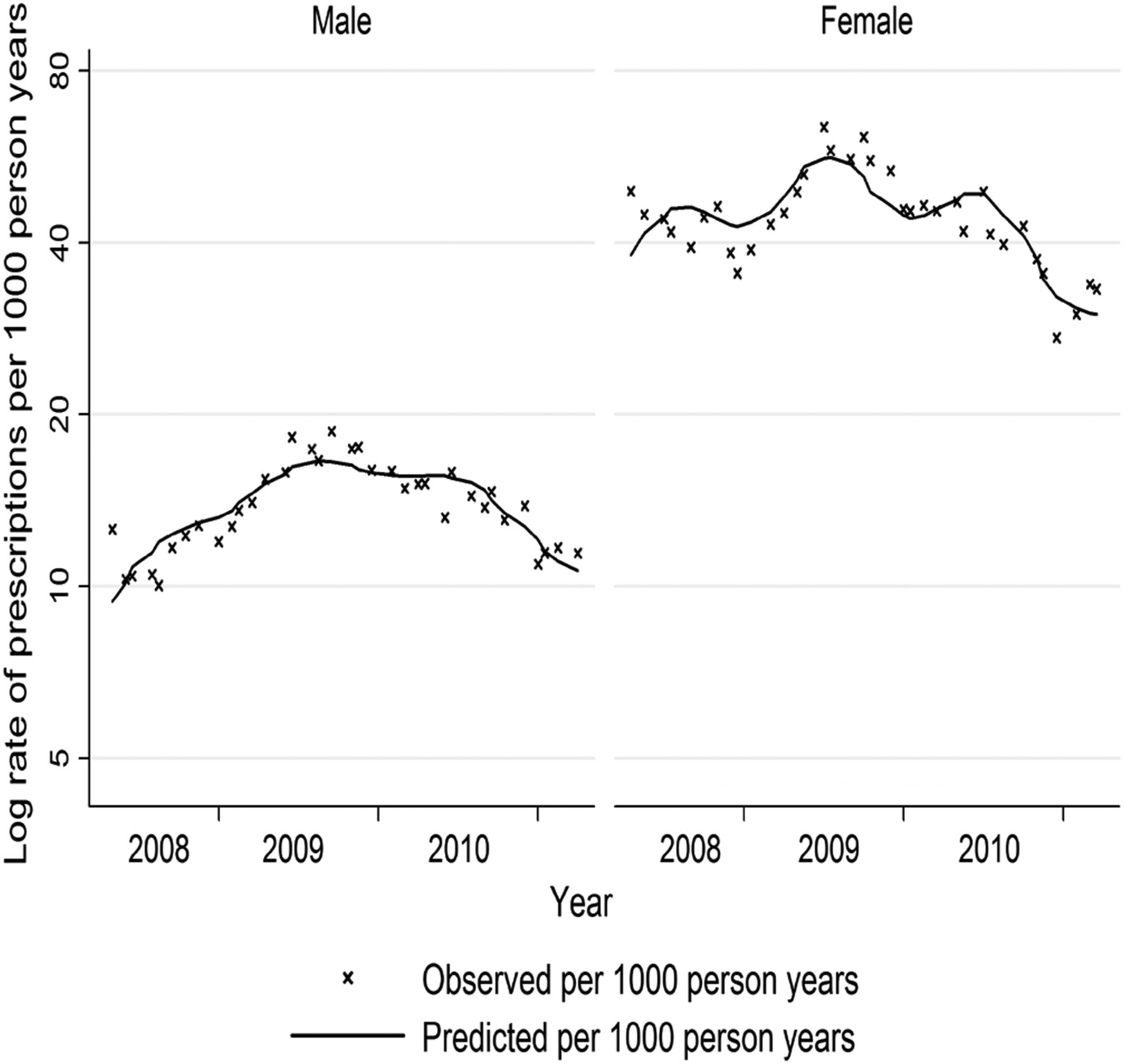
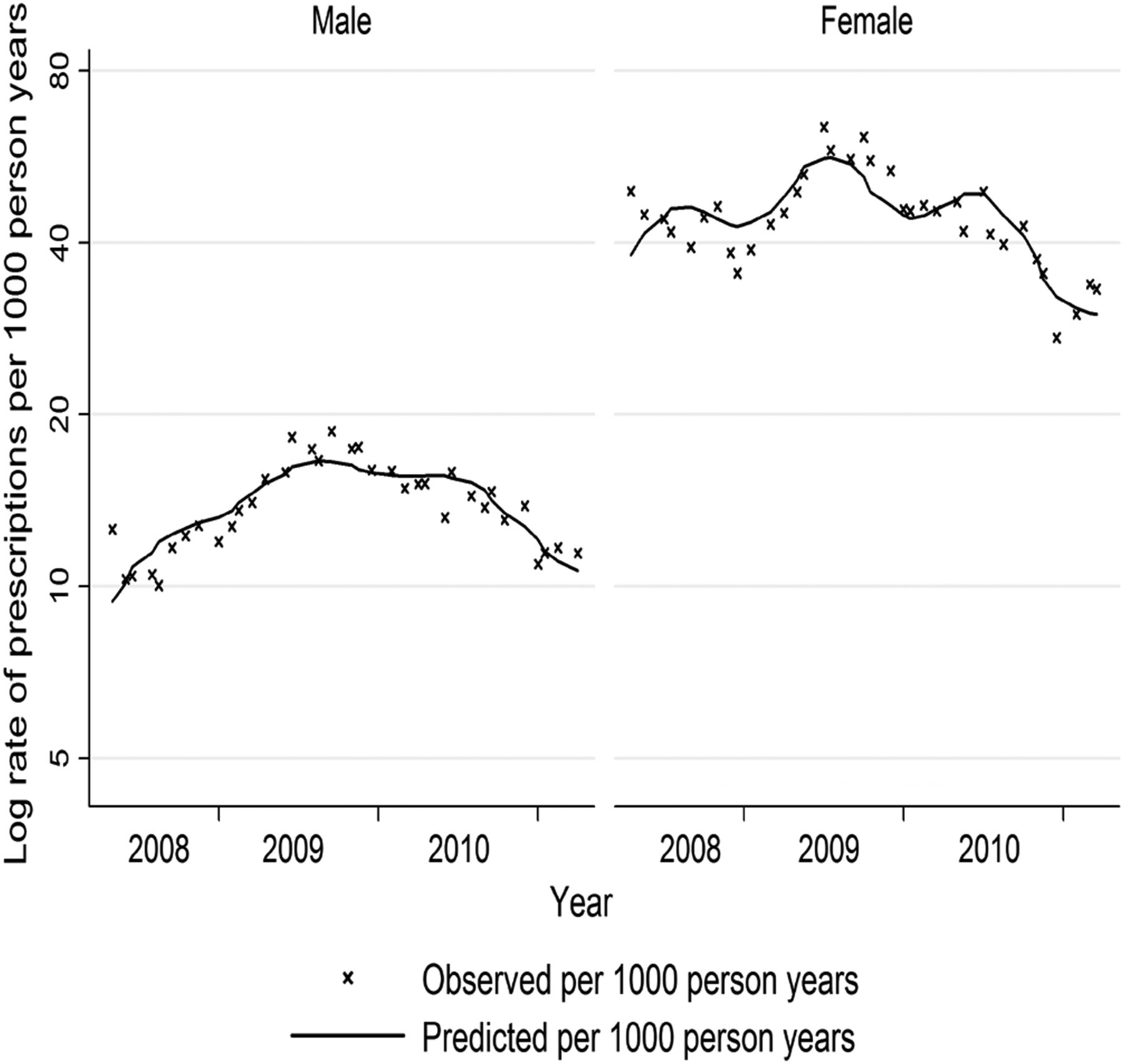
This seasonal variation differed by gender with a stronger significant difference between the peak and trough in female subjects (±11.0% peak to trough for female subjects compared with ±3.5% for male subjects; figure 2).
{kind=link}
{kind=link}
Monthly rates of antiobesity medication prescription by gender plotted on a logarithmic scale (April 2008–March 2011) with fitted long-term trend and seasonal variation.
Discussion
This country-wide study demonstrated a marked seasonal trend in the prescription of antiobesity medication, with a peak occurring in late June/early July and a trough in the winter season. This was particularly evident among female subjects.
Comparisons with other studies
Although this study has clearly demonstrated a seasonal pattern of antiobesity medications, it does not provide a ready explanation for why such cycles occur. All of these prescriptions have been issued by GPs and while they may exhibit different propensities or thresholds for prescribing, there is no obvious reason why this should vary systematically throughout the year. The other alternative, variation in patient preference, seems more plausible and the data suggest that users are keen to lose weight during the months leading up to the summer holiday period. In contrast, prescriptions decline during the winter, reaching a nadir in December perhaps reflecting the perceived futility of trying to lose weight in the run up to the festive season.12 It has been recognised for some time that women are more likely to attend doctors and seek treatment13 which might explain the stronger effect detected. A study of over-the-counter medications, the purchase of which is driven entirely by patient motivation, could shed light on this. The decline in the rate of prescribing since 2007 most likely reflects the withdrawal of sibutramine and rimonabant from the market following fears about their safety.
Strengths and limitations of the study
This was a country-wide study of prescriptions for all antiobesity medications, prescribed by GPs and dispensed to patients. However, the dataset was too small to explore seasonal variations by age, though we suspect these seasonal effects are more pronounced for younger female subjects where uptake is the highest. This could be explored in larger datasets as could the extent to which the seasonal trend is due to a subset of people restarting antiobesity medications each year or if it is a more generalised social phenomenon reflecting some aspect of social contagion.14 The true effect of demand-led variation is likely to be larger than reported here as data on over-the-counter weight loss medications were not available. The analysis included prescriptions for all weight loss drugs, including those that were removed because of safety fears. These account for a small proportion of the total number of antiobesity medications and there is no reason to assume that they would be any less susceptible to a seasonal variation. It is likely that the inclusion (and subsequent removal) of these drugs has introduced more noise into the models and made determination of a seasonal trend more difficult. Finally, there may be some residual confounding by unknown factors which were not available for this analysis.
Conclusions and policy implications
The salience of a health condition is not fixed and is influenced by its (changing) social, psychological and physical context. This would seem to be the case with obesity. The presence of annual cycles in antiobesity medication prescribing suggests that patients consulting in the spring and early summer could offer numerous teachable moments.9 The relationship between prescribing and referral to weight loss programmes was not examined in this study. However, policy makers may wish to consider linking prescribing with referrals to weight loss programmes to examine if similar variations in referrals exist. Further research to clarify if health professionals could capitalise on the increased readiness of obese patients to engage with weight loss programmes at this time is warranted.
What is already known on this topic
-
The use of antiobesity medication as a treatment option for obesity has been increasing.
-
Variation in the use of antiobesity medication may reflect General Practitioner prescribing habits and patient preference.
-
The effectiveness of interventions is improved when they coincide with a teachable moment.
What this study adds
-
Individuals increase their uptake of weight loss medication prior to the summer holiday period and less so during the winter months.
-
Links between prescribing and referrals to weight loss programmes may indicate a time that health professionals could capitalise on an increased readiness of obese patients to engage in weight loss programmes.
Acknowledgments
We would like to acknowledge the help and assistance of the Business Services Organisation who supplied the initial data.
Footnotes
-
Contributors LP, CP, DOR and FK contributed to the planning; all authors contributed to the drafting, revising and final approval of the manuscript; and LP, DOR and CP are responsible for the overall content as guarantors of the study.
-
Funding This work was supported by a grant from the Department of Education and Learning (DEL) of the Northern Ireland government. DEL had no role in the design and conduct of the study; in the collection, management, analysis and interpretation of the data; or in the preparation, review and approval of the manuscript. The researchers were independent from the funders.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.