Article Text

Abstract
Background: Socioeconomic differences in perinatal health decreased in Finland in the late 1990s. Whether the decreasing socioeconomic differences in perinatal health observed in Finland in the late 1990s have continued in 2000–6 was studied.
Methods: The data were based on 965 443 births and 931 285 singletons recorded between 1991 and 2006 in the Finnish Medical Birth Register. Information on socioeconomic position was based on maternal occupation. Perinatal health was measured with six different indicators.
Results: The proportions of preterm, low birthweight and SGA (small-for-gestational-age) births remained stable during the study period, but decreased for LGA (large-for-gestational-age) births and perinatal death. After adjustment for maternal background variables, the socioeconomic differences in preterm and low-birthweight births decreased in the late 1990s and remained low thereafter. In 2003–6, blue-collar workers had a 14% (95% CI 7% to 22%) higher risk for preterm birth and a 25% (95% CI 16% to 34%) higher risk for low birthweight than upper white-collar workers. For SGA, the socioeconomic differences remained unchanged, and the excess risk for blue-collar workers was 44% (95% CI 31% to 58%) in 2003–6. For LGA, the socioeconomic differences increased, and the highest excess risks were obtained among lower white-collar (23%, 95% CI 15% to 33%) and blue-collar workers (24%, 95% CI 14% to 36%). The differences in perinatal mortality decreased until the late 1990s, but increased thereafter. In 2003–6, lower white-collar and blue-collar workers had the highest excess risks: 46% (95% CI 20% to 77%) and 44% (95% CI 13% to 83%), respectively.
Conclusions: The trends in social inequality in perinatal health outcomes were diverging by indicator. The positive trend on diminishing socioeconomic differences found in the 1990s seems to have come to an end.
Statistics from Altmetric.com
Despite the long-term aim to diminish health inequalities, socioeconomic differences in morbidity, mortality and the utilisation of healthcare services have been reported for all Nordic countries.1 2 We have previously reported that the socioeconomic differences in perinatal health decreased in Finland in the late 1990s.3 Nordic comparative studies came to the same conclusion on preterm birth,4 small-for-gestational-age (SGA) births5 and infant mortality.6
Finland experienced a boom economy that after a long levelling period in the late 1970s and 1980s substantially increased differences in income distribution in the late 1990s and early 2000s. Currently, the income differences have increased back to the similar level than in the early 1970s,7 even though they remain smaller than the European Union average.8
The socioeconomic differences in adult mortality have grown since the 1990s, mainly because of elevated mortality in cardiovascular diseases, suicides and increased use of alcohol in the lowest socioeconomic groups.9–11 The trends in perinatal health in Finland have not been studied after the late 1990s. The aim of this study was to examine whether the socioeconomic differences in perinatal health in Finland decreased, were stable or increased in the period 2000–6.
MATERIAL AND METHODS
The Finnish Medical Birth Register (MBR) was initiated in 1987, and is maintained by the National Research and Development Centre for Welfare and Health (STAKES). The register includes information on maternal background, care and interventions during pregnancy and delivery, and on newborns’ outcome until the age of 7 days. The data are collected at all delivery hospitals, and, in the case of home births, by the assisting healthcare personnel.12 All live births and stillbirths with a gestational age of 22 weeks or more, or with a birth weight of 500 g or more, are included in the register. According to a 1991 data quality study, the majority of MBR content corresponded well or satisfactorily with the hospital record data.12 13
Since October 1990, the MBR has included information on the mother’s occupation at the time of birth. This is automatically coded to occupational code and socioeconomic position, as described earlier.3 The socioeconomic positions were aggregated into four groups:
upper white-collar workers (group I), such as teachers, physicians and journalists;
lower white collar workers (group II), such as secretaries, nurses and shop assistants/cashiers;
blue-collar workers (group III), such as dressmakers, cookers and cleaners;
“others” (group O), including entrepreneurs, farmers, students, housewives, pensioners and unemployed people.
We used the following indicators to monitor perinatal outcome: (1) the number of preterm births (<37 gestation weeks based on the best estimate at delivery) per 100 deliveries; (2) mean birth weight; (3) the number of low birthweight children (<2500 g) per 100 newborns; (4) the number of SGA and (5) large-for-gestational-age (LGA) children (according to the national standards for birth weight and gestational age14) per 100 newborns; (6) perinatal deaths (stillbirths and neonatal deaths up to 7 days of life with gestational age of 22 weeks or more or birth weight of 500 g or more) per 1000 newborns.
To study trends in socioeconomic differences, the study period was divided into five periods: 1991–3, 1994–6, 1997–9, 2000–2 and 2003–6. We used t tests, the test for relative proportions and χ2 tests to study differences in background variables and perinatal outcomes by socioeconomic group.
To adjust for differences in maternal background characteristics, adjusted ORs with 95% CIs for differences by socioeconomic group were calculated using logistic regression analyses. For outcome measures, only data for singletons (N = 931 285) were used. Maternal age (continuous), parity defined as the number of previous deliveries (continuous) and mother’s county of residence (six) were included as confounders. Separate analyses were made for calendar time by adding time periods (five) in all logistic regression analyses. For perinatal mortality, additional analyses were made by adjusting for prematurity and low birth weight.
As additional background variables, we investigated the proportion of smokers who quit smoking during the first trimester by socioeconomic group, and the age-adjusted proportion of overweight and obese parturients (pre-pregnancy body mass index (BMI) greater than or equal to 25 and 30, respectively) by socioeconomic group. The information on BMI was available in the MBR from 2004 onwards only.
STAKES, the owner of MBR, gave its permission to use its register data for scientific research, as required by the national data protection legislation.
RESULTS
Since the late 1990s, the proportion of upper white-collar women increased from 16% to 19%, while lower white-collar and blue-collar women decreased from 41% to 35% and from 17% to 13%, respectively (table 1). The proportion of women in the group Others increased from 26% to 33%, mainly because of increasing proportions of women with no reported occupation (from 7% to 14%) and students (from 8% to 10%). The proportion of housewives slightly decreased (table 1).
The substantial differences in the maternal background characteristics by socioeconomic position were similar during the whole study period. Upper white-collar workers were the oldest parturients, had fewer previous pregnancies and deliveries, were less often single and smoked less often during pregnancy than women in other socioeconomic groups (table 2). The differences between other socioeconomic groups were smaller, even though blue-collar workers constituted the highest percentage of single mothers and smokers.
Over time, the mean age of parturient, the proportion of single mothers, and the multiple birth rate increased in all socioeconomic groups. The mean number of previous pregnancies and deliveries increased in all groups excluding the group Others. The mean number of previous pregnancies not ending in a birth increased in all socioeconomic groups, but significantly less among upper white-collar women (4%) than other socioeconomic groups (12–15%).
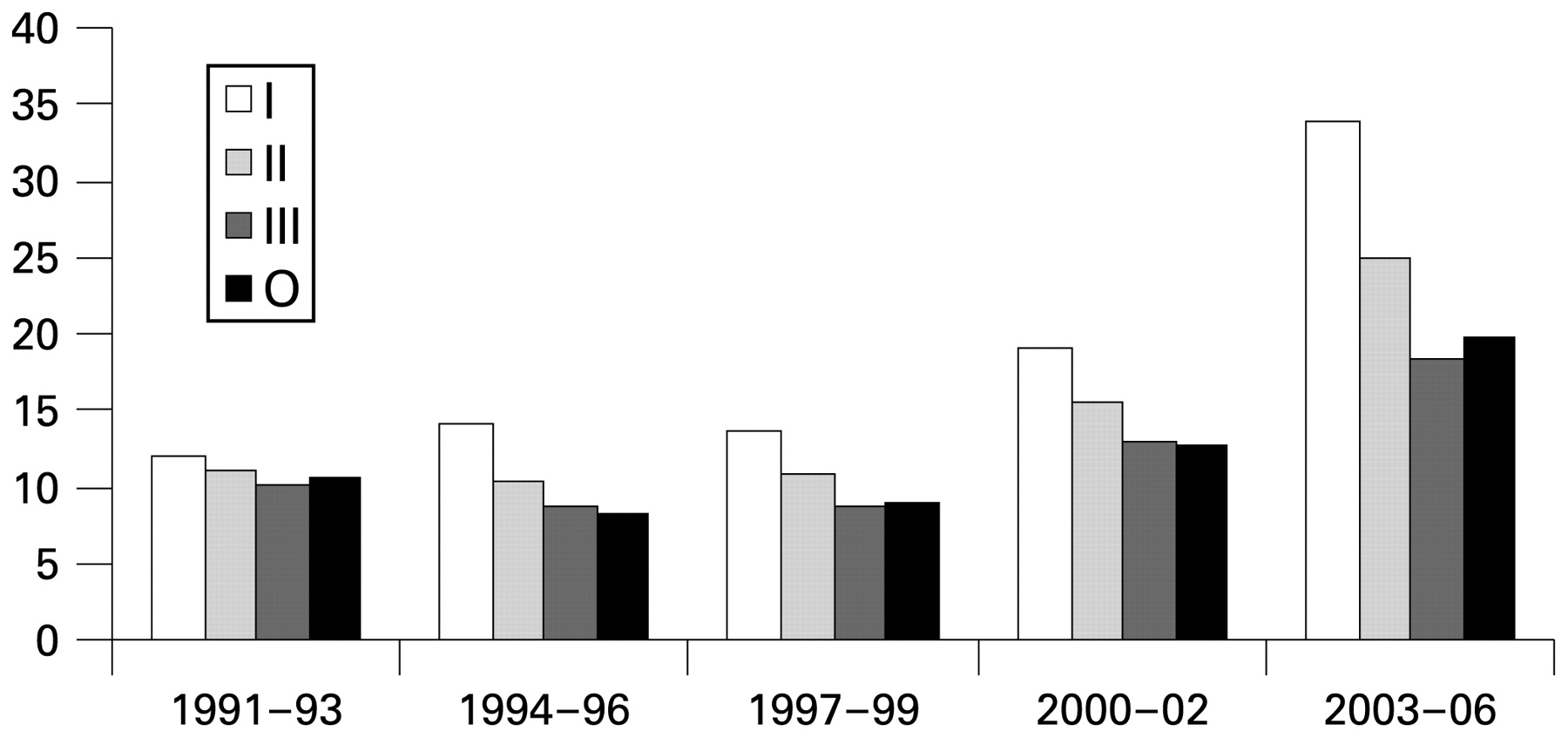
Smoking was most common among blue-collar workers and least common among the upper white-collar workers in all time periods. The proportion of women who stopped smoking in early pregnancy (“quitters”) increased in all socioeconomic groups over time, but the increase was larger in the higher social groups (figure 1). No socioeconomic gradient in rate of quitting smoking was observed in the early 1990s. However, in 2003–6, one out of three upper white-collar workers and one out of four lower white-collar workers quit smoking, while less than a fifth of smokers in blue-collar workers and in the group ‘Others’ quit smoking during pregnancy (figure 1).
{kind=link}
The proportion of smokers, who quit smoking during the first trimester by socioeconomic position, Finland 1991–2006.
Upper white-collar workers were the tallest in 2004–6 (mean height 166.6 cm), had lower mean pre-pregnancy weight (64.9 kg) and BMI (23.4 kg/m2) than other socioeconomic groups (for which corresponding mean values ranged from 165.1 to 165.6 cm, 65.6 to 68.0 kg and 24.0 to 24.9 kg/m2, respectively). The proportion of overweight (BMI 25.0 kg/m2 or more) parturients was 24% in upper white-collar women, 35% in lower white-collar women (age-adjusted OR 1.80, 95% CI 1.74% to 1.86% compared with upper white-collar women), 40% in blue-collar women (OR 2.29, 95% CI 2.19% to 2.38%) and 31% in group Others (OR 1.67, 95% CI 1.61% to 1.72%). The corresponding risks were even higher for obesity (BMI 30.0 kg/m2 or more): 7% in upper white-collar women and 12% in lower white-collar women (age-adjusted OR 1.98, 95% CI 1.88% to 2.10%), 15% in blue-collar women (OR 2.78, 95% CI 2.62% to 2.96%) and 11% in group Others (OR 1.98, 95% CI 1.87% to 2.09%).
Over time the different perinatal outcomes showed different development (table 3). The rates remained similar for preterm birth, low-birth weight and SGA. Mean birth weight decreased by 34 g. Perinatal mortality decreased by 30%: from 6.5 to 4.6 per 1000 newborns, most among blue-collar and upper white-collar women (43% and 37%, respectively). The proportion of LGA children decreased by 18% from 3.5 to 2.9 per 100 newborns. The decline was larger for upper white-collar workers (22%) than for other groups (10–13%).
A clear socioeconomic gradient was found for unadjusted results: the lower the socioeconomic position the poorer the infant outcome. The mixed group Others had similar or sometimes even higher risks than blue-collar women. Adjustment for maternal background characteristics (age, parity and region) increased the socioeconomic gradient in all outcomes when comparing other socioeconomic groups to upper white-collar women. After adjusting for the background characteristics, the socioeconomic differences between upper and lower white-collar women with respect to preterm birth, low birth weight and SGA remained at the same level during the study period. For perinatal mortality, the differences were statistically significant only in the first and the last time period. For LGA, the differences increased during the study period. After including period variable in the model, all socioeconomic differences remained statistically significant.
The differences in the risks of preterm birth and low birth-weight between blue-collar and upper white-collar women were halved during the 1990s, but thereafter these differences remained at the same level. The excess risk of SGA births remained at the same level during the entire study period, but the excess risk of LGA births increased.
The difference between upper white-collar women and the group Others remained statistically significant and at a similar level for other outcome variables but perinatal mortality, for which an increase in the difference was observed from the late 1990s onwards (table 3). We also investigated perinatal mortality trends within subgroups of the group Others. Among housewives and the parturients without occupational information, the adjusted perinatal mortality trends were similar to that of the whole group ‘Others’. In contrast, among students, the perinatal mortality trend did not differ from that of upper white-collar workers (data not shown).
Prematurity explained one-third on the excess risk for perinatal mortality, and the higher incidence of low-birth weight among the women with lower socioeconomic status explained round half of the excess risk. All socioeconomic differences, however, remained statistically significant.
DISCUSSION
Socioeconomic differences were observed for all perinatal outcome variables in Finland, but the most recent trends have been divergent for different outcomes. The socioeconomic differences in preterm birth and low birth-weight have remained relatively small and at the same level since the late 1990s. In SGA the socioeconomic differences remained relatively large, and at the same level during the whole study period. The socioeconomic differences in perinatal mortality and LGA increased.
A strength of this study was that we used population-based register data with complete coverage and high quality, and most of the variables used in this study were collected similarly during the whole study period. The major weakness of our study was the limited number of possible confounders in the routinely collected register data. The Finnish MBR does not contain any information on the father, but this information can be linked to information on highest level of education, socioeconomic position and taxable income, as shown previously.4–6 The data linkages are, however, expensive and cannot be performed on a routine basis. In addition, Statistics Finland can only return a sample instead of a complete population-based data set, due to their strict data protection policy. This may cause problems when studying, for example, rare cases, such as perinatal deaths.
Possible explanations for the changes in the socioeconomic differences over time include changes in the composition of occupations, being outside the labour force, occupational exposures and avoidance of harmful work exposure, increased knowledge about preventive and health-promoting behaviour, and in prenatal and delivery care.3 The percentage of women in the highest socioeconomic group increased, and the proportion of women in the two lower socioeconomic groups declined as a consequence of the increased educational level among Finnish women and the change in occupational structure from industrial work to services. Our data showed that the proportion of women outside the labour force (students, unemployed people, retired people and housewives) increased from 12% in the early 1990s to 17% in 2003–6. However, excluding students with good perinatal outcomes, the increase was only moderate, from 7% to 8%, as shown in table 1. We do not, however, suggest that these changes could explain our findings, because the relative changes in the sizes of the groups were quite small.
Some parturient characteristics are not included in the MBR, and some were introduced in the MBR in 2004, such as detailed information on women’s medical conditions and their pre-pregnancy BMI. We were not able to use these variables in our trend analysis. Examples of the other missing data include migrant background and substance abuse. Recent studies show that the percentages of women of migrant origin as well as women with alcohol or drug-related problems have increased in Finland.15 16 Some migrant groups have increased risks for poor perinatal outcomes. For example, women of African origin have higher perinatal mortality rates than other migrant groups or women of Finnish origin.15 Also, parturients with a substance abuse problem during pregnancy have increased risks for poorer perinatal outcomes than parturients in general.16 Most of the women in these two groups are classified in the group Others in the MBR, since they are often out of the labour market. However, their small proportion of the total number of parturients or even among women in the group Others cannot explain the total unfavourable development in perinatal outcomes.
Our results show that socioeconomic differences have increased in some background characteristics, for example smoking and previous pregnancy history. The women in the group with higher socioeconomic position quit smoking much more often than women in other socioeconomic groups.17 Also the mean number of previous pregnancies not ending in a birth has increased more among other socioeconomic groups than upper white-collar workers. The contribution of these factors to the observed socioeconomic differences in perinatal health should be investigated in more detail.
Socioeconomic differences in SGA did not diminish and the differences in LGA and perinatal mortality even increased. We cannot exclude the explanation that this is caused by the deteriorating MBR information. Our results, however, were based on total population-based data with almost a million births, and we were able to define a socioeconomic position for three out of four mothers. An emerging tendency was that the number of mothers with missing information on maternal occupation has grown rapidly. Continued efforts are needed to maintain the good register quality both for background variables and outcome variables to ensure reliable routine health monitoring by means of existing register data.
Our data showed that perinatal outcomes in Finland are good, but remained at the same level since the early 1990s.18 There are two exceptions: perinatal mortality rate and the proportion of LGA births have decreased in all socioeconomic groups. These are the same indicators for which increased socioeconomic differences were observed. Thus, from the public health perspective, widening of socioeconomic differences is not necessarily bad, if at the same time all groups do better. Improved care of preterm born infants is likely to be the main reason for the diminished perinatal mortality rate.19 Outcomes of diabetic pregnancies have been improved after a nationwide recommendation to standardise their care was given in 1993,20 which may explain the decline in the proportion of LGA births.
Internationally the Finnish perinatal health outcomes are among the best in Europe,21 but there are still possibilities for further improvement. Among upper white-collar workers, the postponement of childbearing has led to the mean age of mothers being 2.5 years higher than on average in Finland. Decreasing the average age at first birth and the percentage of women aged 35 years of more could further improve the situation.22 For other socioeconomic groups, public health actions aiming at reducing smoking prevalence, overweight and obesity, substance use and occupational hazards during pregnancy, should not only reduce the socioeconomic differences in perinatal health, but also improve the perinatal health outcomes in the total population.
What is already known on this subject
Socioeconomic differences in perinatal health decreased in Finland during the late 1990s.
Diminishing socioeconomic differences in perinatal health may improve perinatal health outcomes in general.
What this study adds
Socioeconomic differences in perinatal health vary by the health indicator.
The excess relative risks for preterm birth and being of low-birth weight among blue-collar workers have remained low since the late 1990s.
The socioeconomic difference in risk for SGA births has remained unchanged since the early 1990s, but increased for LGA births.
The excess risk for perinatal mortality among blue-collar workers has increased since the late 1990s.
REFERENCES
Footnotes
Competing interests: None declared.
Funding: This study is a part of NorCHASE collaboration (Nordic Collaborative project on health and social inequality in early life), which was funded by the Research Programme in Longitudinal Epidemiology, supported by the Nordic Council of Ministers and administered by NordForsk (The Nordic Research Board).