Article Text

Abstract
Objective: To evaluate the strength of the evidence provided by epidemiological literature investigating drinking pattern as effect modifier of alcohol intake on the risk of coronary heart disease (CHD).
Design: Meta-analysis of observational studies.
Data sources: Medline, citation tracking, from 1966 to 2006.
Review methods: Original studies investigating the amount of alcohol intake, combined with the frequency of alcohol consumption and/or pattern of alcohol drinking affecting the risk of CHD were extracted. Among them, cohort and case–control studies reporting sufficient data to perform statistical analyses and using people who abstained from alcohol as the reference were included.
Results: Six (4 cohort and 2 case–control) out of 118 studies reviewed met the inclusion criteria. Compared with those who abstained from alcohol, regular heavy drinkers and heavy irregular or binge drinkers showed significantly different pooled relative risks of 0.75 (95% confidence interval 0.64 to 0.89) and 1.10 (1.03 to 1.17) respectively. The dose–response relation between the amount of alcohol intake and CHD risk was significantly different in regular and irregular drinkers. A J-shaped curve, with nadir around 28 grams of alcohol per week, and last protective dose of 131 grams per week, was obtained including drinkers who consumed alcohol for 2 days a week or less. Conversely, in people who consumed alcohol for more than 2 days a week a significant protective effect was seen even when drinking high amounts of alcohol.
Conclusion: This meta-analysis suggests that binge and heavy irregular drinking modify the favourable effect of alcohol intake on the CHD risk. However, this conclusion should be taken with caution because of the small number of studies considered.
Statistics from Altmetric.com
There is convincing evidence that moderate alcohol consumption protects against the risk of coronary heart disease (CHD).1 On the other hand, it has been consistently shown that heavy alcohol consumption and problem drinking are associated with an increased risk of cardiovascular diseases.1–3 The combination of protective and harmful effects influence results in a U-shaped or J-shaped dose–response relationship between alcohol and CHD.4
Most studies on this issue were conducted in north-west European countries and in North America. According to a meta-analysis of 51 studies, lower protective effects of alcohol were reported by investigations performed in countries outside the Mediterranean area than in Mediterranean populations.1 Recent evidence from eastern Europe is inconsistent with reference to alcohol and cardiovascular diseases.5 Finally, decreasing cardiovascular mortality rates were observed in Poland in 1981–2, when alcohol was rationed during martial law, and in Russia in 1985, after the anti-alcohol campaign.6 7
These findings could partly be explained by differences in the pattern of alcohol consumption. Daily and regular use of wine, mainly during meals, is the typical pattern of alcohol consumption of Mediterranean populations, whereas consumption of beer and spirits, mainly during weekends, is typical of northern European and northern American populations, and episodic binging intake of spirits is typical of eastern European populations.8
Most studies on the alcohol–disease association collected information on the total amount of alcohol consumed during a period that includes both drinking and non-drinking days. This does not allow the investigation of the role of drinking pattern, especially irregular heavy or binge drinking, in modifying the effect of the amount of alcohol consumed.9 Thus, only few data are available on this topic.
The main aim of this paper is to evaluate whether drinking pattern, defined by the frequency of drinking days as well as drinking intensity per drinking occasion, modifies the effect of alcohol intake on the risk of CHD. We have thus summarised the available data on this topic using a meta-analytic approach including published cohort and case–control studies.
METHODS
Literature search
We performed a Medline search of the literature from 1966 up to and including 2006, supplemented by attention to all references in the articles recovered through Medline and in several relevant reviews and meta-analyses published on this subject.1–5 10–25
The search process involved combining all the possible text word terms, and MESH headings, concerning disease (coronary heart disease, coronary death, myocardial infarction, ischaemic heart disease) and exposure, expressed as both quantity or dose of alcohol intake and pattern of alcohol drinking. Owing to the lack of a standard definition of pattern of alcohol drinking, the search focused on frequency of alcohol drinking (regular and irregular) and several terms considered as proxies of binge drinking or irregular heavy drinking (problem drinking, alcoholic intoxication, heavy episodic drinking, hangover).
The search was restricted to studies published in English-language journals.
Study selection
Each publication identified by this process was reviewed and included in the analysis if the following criteria were met. First, the study had to be published as an original article. This implied that only cohort and case–control studies were included and that abstracts, letters, editorials, reviews and meta-analyses were not eligible. Second, the study reported sufficient data to perform statistical analyses. Hence the reported findings (i) had to be expressed as relative risk (RR, odds ratio or hazard ratio), considering either different combinations of quantity and frequency of alcohol intake (eg, grams of alcohol per day, stratified according to number of days of consumption) or directly defining the drinking pattern (eg, binge drinking, heavy irregular drinking or heavy regular drinking) as exposure categories; (ii) had to report precision of RR (expressed as variance, standard error or confidence interval), or the absolute number of cases and non-cases for each exposure category; (iii) considered abstainers as reference category, or at least reported data allowing to recalculate RRs with respect to abstainers. Moreover, studies reporting intake only during the day preceding the onset of coronary heart events were excluded. In fact, although a high current consumption might be considered as a proxy of binge drinking, we did not consider this definition to be satisfactory.
The full texts of all potentially relevant articles were obtained and two reviewers independently checked the data. If more than one paper with the same data was identified, only the one containing the most comprehensive data was included. A third reviewer from the group was available to address any disagreements.
Study coding
Studies were coded on the basis of design (cohort or case–control) and outcome (incident case or death). Other characteristics of the studies such as first author, year of publication, study population (country, size, age and gender), duration of follow-up (for cohort studies) or source of controls (hospital or population based for case–control studies), and definition of exposure categories according to drinking pattern were also recorded. Finally, absolute number of cases and non-cases, RR, and corresponding precision, were recorded for each exposure category, stratified by gender, whenever available.
Data analysis procedures
First, we tested the hypothesis that the pattern of alcohol drinking implies different RRs of CHD when compared with abstainers. The drinking pattern was classified in two categories according to what was reported in the original article: (i) binge or irregular heavy drinking and (ii) regular heavy drinking. Pooled estimates (RRp), and corresponding 95% confidence intervals (CI), were separately obtained for the two categories of drinking pattern, each compared with abstainers. The estimates were derived from fixed effects method, and homogeneity between categories of drinking pattern was tested according to Greenland.26
Secondly we tested the hypothesis that frequency of drinking days per week modifies the dose–response relationship between the total amount of alcohol intake consumed in a week and CHD risk. This analysis was restricted to studies reporting different combinations of quantity and frequency of alcohol consumption. Since studies used different units of measure to express daily alcohol consumption (grams, ounces or drinks), we adopted grams as the standard unit of measure, considering the following equivalences: 28 grams per oz and 12.5 grams per drink. The pattern of alcohol drinking was defined according to the categories of frequency of intake, considering regular and irregular drinkers as those who consumed alcohol for more than 2 days a week, and for 2 days a week or less, respectively. Since both quantity and frequency of alcohol intake were given by a range, we assigned to each level the value corresponding to the mid-point of the range.
Owing to the expected non-linear relation between alcohol and CHD, flexible meta-regression models were fitted. These fractional polynomials fitting aggregate meta-data are described in detail elsewhere.22 Briefly, second-order fractional polynomials are a family of models generated from power transformations of a continuous exposure variable (in our case quantity of alcohol intake), restricted to a predefined set of exponents (in our case the following exponents were tested: −2, −1, −0.5, 0, 0.5, 1, 2). The best fit among the family of models generated from the combinations of exponents is defined as that with the lowest residual deviance. The family offers considerably flexibility, since a rich set of possible functions, including some so called U-shaped and J-shaped relations, may be accommodated.27 28 The comparison between two hierarchical models (the first only considering two power transformations of the exposure level and the second also the interaction terms with the categories of drinking pattern) was tested by the likelihood ratio test. Significance offers evidence that drinking pattern modifies the dose–risk relation between alcohol intake and CHD risk. The Meta Command in STATA929 and SAS macro software22 were respectively used for the first and the second data analysis procedure.
RESULTS
General characteristics of the included studies
The Medline search allowed 1032 articles to be retrieved. Among them, 113 concerned the topic of this study. Eighty-nine were excluded because they did not provide any information on irregular drinking pattern, whereas another five did not present any risk measure. Nine articles investigated overall mortality rather than cardiovascular, and another four studies were excluded because the exposure was subsequent to the cardiovascular event or because the reference category was not adequate. In total, six studies investigating drinking pattern and CHD risk satisfied our criteria and were included in the meta-analysis.30–35
Table 1 summarises their main characteristics according to study design. From the four cohort studies (including 41 946 participants),30–33 a total of 3329 coronary events were observed. The follow-up period ranged from 5.7,33 to 16.3 years.32 The two studies involving a case–control design34 35 in total included 12018 cases and 6555 controls.
Drinking pattern and CHD risk
As shown in table 1, heavy irregular or binge drinking was defined in a wide variety of ways in different studies, ranging from high consumption in a single occasion30 31 35 to heavy intake a few times a week.33 34 In one study,32 the total volume of alcohol consumed in 1 year was separated into volume consumed during heavy drinking occasions and non-heavy drinking occasions.
Figure 1 shows forest plots of study-specific RR estimates (and their confidence intervals) both for heavy regular drinkers and heavy irregular/binge drinkers compared with abstainers, stratified by study design and gender (when available). Overall, 6 and 10 individual effects respectively looking at heavy regular and heavy irregular/binge drinking affecting CHD risk were used. Individual RRs associated with heavy regular and heavy irregular/binge drinking respectively ranged from 0.4 to 1.4 and from 0.7 to 2.3. Pooled RR of 0.75 (95% confidence interval 0.64 to 0.89) and 1.10 (1.03 to 1.17) respectively were obtained by assembling heavy regular and heavy irregular/binge drinkers individual estimates. The two pooled RRs, also reported in the forest plots, were significantly different (p<0.001). There was no statistical evidence of between-study variation across the individual estimates for heavy irregular/binge drinkers (p = 0.088), whereas for heavy regular drinkers heterogeneity was significant (p<0.01).

Pooled estimates calculated separately for men and women were not significantly different from each other, both for heavy regular and for heavy irregular/binge drinkers (data not shown).
Drinking pattern and dose–risk relation
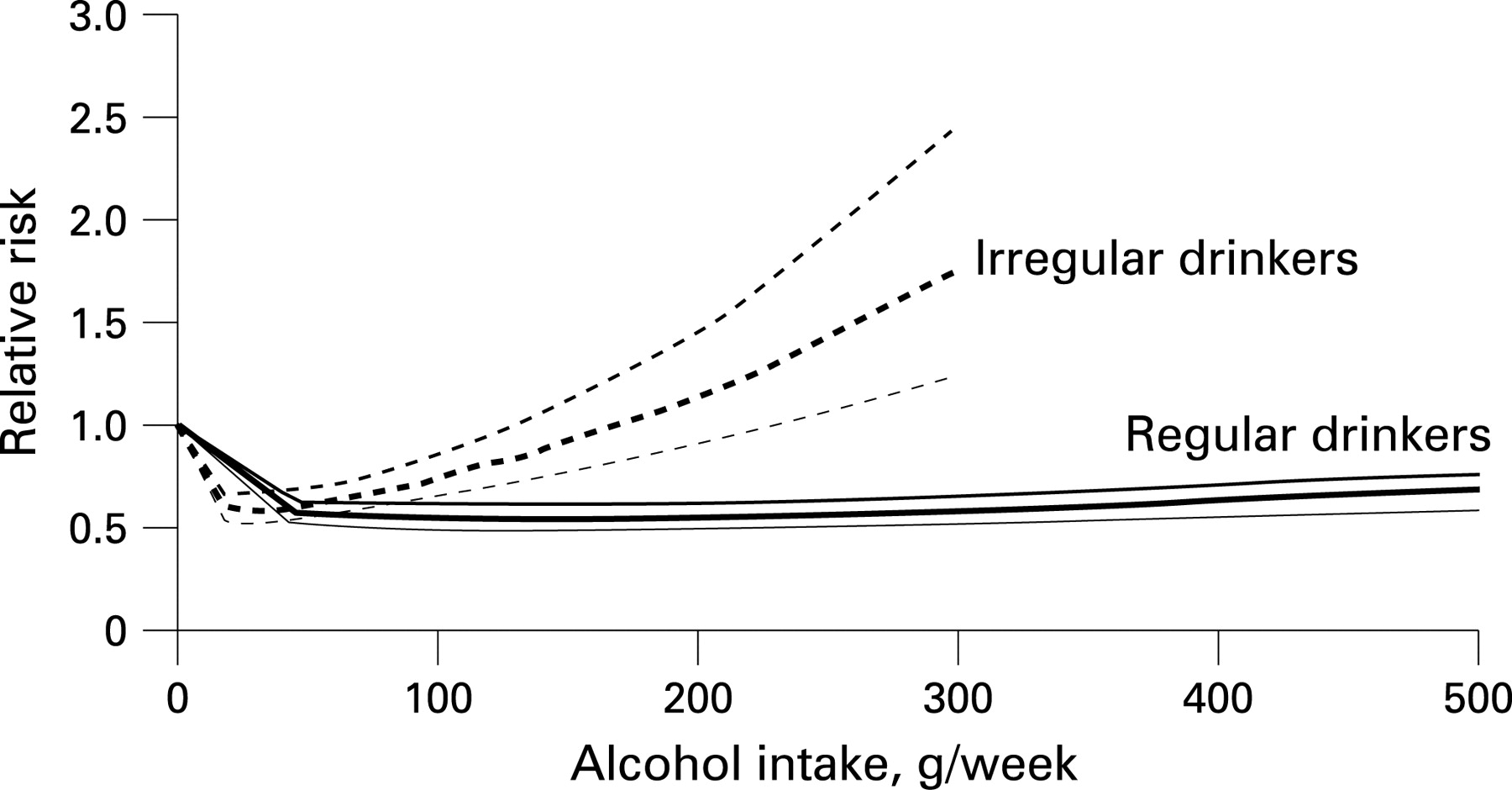
Only two studies,33 34 providing four separate dose–response relations, were considered for this analysis. Altogether, 10 094 CHD events were considered (7072 men and 3022 women). Owing to the small number of studies, no attempt to evaluate separate gender effects have been performed. Figure 2 compares pooled curves (and corresponding 95% confidence bands) describing the dose–response relation between weekly alcohol consumption and CHD risk separately in regular and irregular drinkers.

{kind=link}
{kind=link}
A J-shaped curve was found for irregular drinkers: the nadir and the last protective dose were 28 g per week (RR 0.59; 95% CI 0.53 to 0.65) and 131 g per week (RR 0.85; CI 0.72 to 0.99) respectively. The dose–response function for regular drinkers showed an L-shaped curve with significant protective effects even for the highest dose of alcohol intake. The dose–risk curves were significantly different (p = 0.047).
DISCUSSION
This meta-analysis, including most published information on alcohol drinking pattern and CHD, offers evidence that drinking pattern modifies the action of alcohol intake on the CHD risk. In particular, the well-established protective effect of alcohol on CHD risk is confirmed for regular drinkers, even with heavy amounts of alcohol intake. Conversely, compared with abstainers, binge and heavy irregular drinkers are at increased risk of CHD.
Several studies, using baseline comparators other than those who abstain from alcohol, have consistently shown excess CHD risk among problem drinkers. Compared with non-problem drinkers, a significant fourfold risk excess in subjects consuming six or more drinks per day was found in a longitudinal study from Chicago.36 A Finnish study comparing non-abstainers and subjects with frequent hangover, reported a RR of 2.4 for subjects with hangover at least once a month.37 A Swedish study reported non-significant RRs of 0.8 and 1.8 for men and women who on the same occasion drank at least a half bottle of spirits, or a bottle of wine, or often felt intoxicated compared with subjects reporting never having this drinking pattern.38
In a cohort study, conducted on 38 077 US male health professionals, a significant protective effect (RR = 0.63) of heavy regular drinking (⩾30 g/drinking day per 5–7 drinking days/week) was reported, compared with subjects drinking less than 1 day per week. No significant effect was observed for heavy irregular drinkers (⩾30 g/drinking day per 1–2 drinking days/week).39
Favourable changes in high-density lipoproteins described for regular alcohol drinkers do not affect binge drinkers to the same extent; however, adverse changes in low-density lipoproteins are observed. Irregular drinking predisposes also to histological changes of the myocardial conducting system and to a reduction in the threshold for arrhythmia, in particular ventricular fibrillation.40 These factors may explain the absence of the favourable effect of binge and irregular heavy drinking on CHD risk.
It has been shown that studies finding harmful effects of alcohol on CHD risk have less chance of being published than studies reporting protective effects (publication bias).1 41 Other potential sources of selection bias exist, since the studies included in our meta-analysis did not report information published in non-English language articles and abstract-only publications.
Residual confounding, due to incomplete adjustment for risk factors of CHD and/or to uncontrolled factors, cannot moreover be excluded. In particular, socioeconomic status may play a role, since problem and binge drinkers are more likely to belong to lower socioeconomic groups than regular drinkers or abstainers.31
Binge and irregular heavy drinkers were defined in a wide variety of ways in the included studies. In spite of this, we did not find any evidence of RR heterogeneity across them. However, heterogeneity tests are known to be underpowered.42
Few epidemiological studies included information to test the hypothesis that drinking pattern could modify the protective effect of alcohol on the risk of CHD, and the present meta-analysis reflects the scarcity of data on this issue. These limitations notwithstanding, this meta-analysis still includes most published information on drinking pattern and CHD. Our results support the hypothesis that binge and heavy irregular drinking is associated with excess CHD risk.
What this study adds
Few studies published so far examined the effect of drinking pattern or heavy irregular drinking on CHD.
Our meta-analysis suggests that both binge and heavy irregular drinking do not show a favourable effect of alcohol intake on the CHD risk, as opposite to regular drinking.
Binge and heavy irregular drinking is associated to increased CHD risk.
Policy implications
The unfavourable effect of CHD is an additional reason to avoid binge and heavy irregular drinking.
Acknowledgments
The work on this manuscript was conducted within the European Commission Public Health Project: HEM – Closing the Gap – Reducing Premature Mortality. Baseline for Monitoring Health Evolution Following Enlargement (grant agreement no 2003121) to the Cancer Centre and Institute of Oncology, Cancer Epidemiology and Prevention Division, Warsaw (principal investigator, Witold Zatonski). Additional support for this study was provided by LILT (Italian League Against Cancer). Carlo La Vecchia was supported by a Senior Fellowship of the International Agency for Research on Cancer, Lyon.
REFERENCES
Footnotes
Competing interests: None declared.
Linked Articles
- In this issue