Article Text

Abstract
Study objective: To describe the impact of changes between employment and various forms of non-employment, and vice versa, on the psychological wellbeing of men and of women.
Design: Separate multivariate models for men and for women were constructed to study the association between employment transitions and episodes of psychological distress (general health questionnaire).
Participants: 13 359 employment transitions from 5092 people aged 16–74 years in the British household panel survey from 1991 to 1998.
Main results: Transitions from paid employment to either unemployment or long term sick leave were associated with increased psychological distress for both men and women. Starting maternity leave or staying home to look after the family were also associated with psychological distress for women. Transitions from these roles to formal employment resulted in an improvement in mental health. There was some evidence that the effects were felt most strongly within six months of the transition.
Conclusions: This paper provides further evidence that movements between paid employment and various forms of non-employment, in addition to unemployment, have an impact on mental health. The emphasis on transitions between a full range of employment states for both men and women from a large population based longitudinal study and a comparison of the relative magnitude of effects are unique features of this analysis. Interventions are suggested to minimise the psychological distress associated with transitions.
- GHQ, general health questionnaire
- BHPS, British household panel survey
Statistics from Altmetric.com
Becoming unemployed is associated with increased mortality and worsening physical and mental health.1 There is also evidence that gaining or regaining employment is beneficial for mental health.1,2 There is considerable debate about the direction of causality in this association. Does unemployment cause poor health or does being in good health mean that a person is more able to gain and keep a job?3 A recent review2 found that many earlier studies were cross sectional, so that they could not address this issue of causality; lacked the use of a standardised mental health instrument; and, were often focused on a specific occupational setting. More recent studies have overcome some of these limitations. In general, the evidence supports the hypothesis that unemployment is associated with increased psychological distress compared with people who are in paid employment, after controlling for various factors such as, socioeconomic status, education, and income. Such studies minimised the potential bias attributable to health selection by controlling for baseline health status.2
There is also an increased awareness that other forms of non-employment need to be considered.4 For example, research to date shows that retirement may have a beneficial effect on mental health.1,5 People looking after the home have been shown to have similar mental health to those in employment unless they have significant child caring responsibilities and/or they are seeking employment.6,7
Only a small number of studies have been conducted using British longitudinal data8,9–12 and few of these examine the full range of non-employment experiences. Moreover, studies generally examine the association between health and the experience of a specific employment state rather than the effect on health of transitions to and from these. Often these studies fail to consider the important differences in the relations between employment and health for men and for women, either grouping them together in a single model11,12 or only including men in their analyses.8,9,10 Against this background, the aim of this paper is to undertake a systematic exploration of the effect of transitions between employment and all types of non-employment and vice versa on the mental health of men and of women in the general British population. Using longitudinal data, this paper addresses the following questions:
-
How do transitions to and from paid employment affect mental health?
-
What part does health selection play in these associations?
-
Do these associations vary for different forms of non-employment?
-
How do these transitions affect mental health differently for men and women?
METHODS
Data
Data for this study were obtained from the first eight waves (1991–98/99) of the British household panel survey (BHPS); an ongoing longitudinal survey of a nationally representative sample of private households in Great Britain.* Originally, the BHPS consisted of 5000 households, and all eligible adults (aged ⩾16 years at each wave) within them are followed up and interviewed annually.
Employment transitions
This paper makes use of the detailed employment information collected annually, which has then been converted into employment episodes.14,15 In the first eight waves of the BHPS there were 36 791 employment episodes recorded for 14 168 respondents. From these, employment transitions were constructed for people who changed employment states between 1991 and 1998/99. Sufficient information was available to describe changes of state in both directions between employment and different types of non-employment as defined in the BHPS (unemployed, retired, full time study, maternity leave, family care, and long term illness) for 22 623 transitions. Although information was available for within state transitions, and these are included in the analyses here, they are not the focus of this paper.
Figure 1 shows the transitions that were excluded as a result of specific exclusion criteria adopted or missing data. This study focused on people who were less than 75 years old at the time the transition took place because very few transitions occurred over this age (n = 129). Employment data were missing from some of the remaining transitions (n = 1753), and general health questionnaire (GHQ) information was either missing or not available within the time period surrounding the employment change for 7382 transitions. The final dataset therefore consisted of 13 359 transitions from 5092 people, which was representative of the age and sex distribution of the total transition sample.

The effect of exclusion criteria and missing data on the employment transitions and population studied.
Health measure
In this study the 12-item GHQ (GHQ-12), which is a well validated screening instrument for minor psychiatric morbidity in longitudinal studies16,17 was used as the main outcome measure. Each of the 12 items has four possible responses. Endorsement of either of the two most extreme responses, for example, “more than usual” or “much more than usual” as compared with “same as usual” or “not more than usual” elicits a score of 1 with a total score ranging from 0 to 12. A dichotomous variable was created using a threshold of three or more (the mean score from the study population) to indicate the presence of mental illness.18
The GHQ measures from the two annual interviews before and after each transition date were identified for this paper. This means that the time between the transition and the measurement of GHQ varied for each transition. To ensure the GHQ information was sufficiently close to the transition event, only transitions where a GHQ measure could be identified within the two years before the transition occurring and within one year after the transition had occurred were analysed. This approach, however, meant that the same GHQ measure could be obtained for more than one transition; the effects of such “intervening” transitions were considered in the analysis.
Statistical analysis
To explore the effect of different kinds of employment transitions on whether or not a person was a GHQ case after a transition, logistic regression models with robust standard errors to account for the multiple observations from participants were constructed19 using Stata 7.0.
The analysis was undertaken in two parts. Firstly, in model 1, the effect of broad transitions to and from paid employment was examined, controlling for age and sex. To examine the importance of health selection in these associations, two measures of prior health were then added to the model. A binary variable indicating GHQ caseness before the transition was included in all models to adjust for baseline mental health. Using the BHPS non-employment category “long term illness”, a binary variable (called “sick”) was constructed to identify people who were unable to work because of ill health.†
To focus on the subtle differences in the relation between different employment transitions and changes in mental health, these models were kept comparatively simple. We recognise that a wide range of confounders are included in models in the literature.12 However, without a clear theoretical rationale, this may obscure rather than clarify a relation.20 While it is important to explore the role of different confounders, mediators, and moderators within a theoretical framework, we wished to keep a clear focus in this paper on the direct relation between employment changes and health. The other factors included were the number of previous transitions experienced, whether other transitions intervened between the transition of interest and the GHQ measure, and the duration between the prior GHQ measure and the transition. However, none of these variables proved significant.
Secondly, separate models were constructed to test the association between more detailed transitions. Model 2 examines the subset of transitions from paid employment to the different forms of non-employment and model 3 examines transitions from the various types of non-employment into paid employment.
Men and women were analysed separately because of their very different employment patterns, and the models included the same covariates as described for the first part of the analysis. In addition, separate models were estimated for those transitions where the GHQ measure was obtained less than and more than six months after the transition. These models are not presented here, but the key results are highlighted.‡
RESULTS
Employment transition patterns
Table 1 describes the pattern of the employment transition types for men and for women. Most transitions occurred within formal employment and between employment and various types of non-employment. Overall, more transitions involved women than men; however, there were slightly more women (2757) than men in the sample (2335). The average number of transitions per person was three for both men and women across the eight years of the survey. For transitions between paid employment and non-employment, those into unemployment were the most common for men, and those into family care, in addition to unemployment, were the most common for women.
The number of employment transition in each transition category for 2335 men (6204 transitions) and 2757 women (7155 transitions) from the BHPS 1991–1998
The effect of broad employment transitions on psychological distress
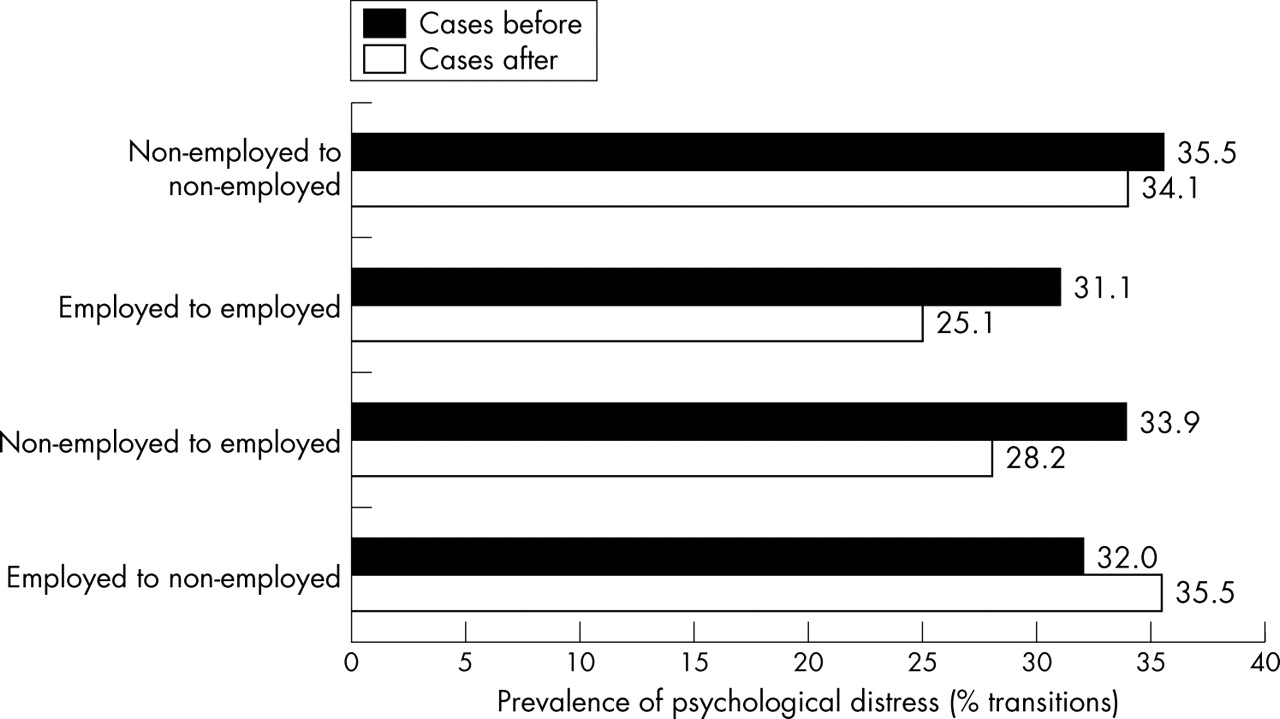
Figure 2 presents the number of GHQ cases as a percentage of transitions by the main type of transition. The highest percentage of cases was found for the non-employment groups both before and after a transition. For those who remained in non-employment, the percentage of cases before transition was slightly higher than for those who became formally employed after non-employment. This suggests that there may be health selection effects operating with healthy people being selected into employment. The largest percentage of cases after transition occurred for those who either remained or became non-employed. The number of GHQ cases fell by about 6% for transitions to paid employment, either after non-employment or from another form of paid employment.
{kind=link}
{kind=link}
The prevalence of psychological distress (GHQ-12 score ⩾3) before and after employment transitions (n = 13 359 transitions).
Table 2 displays the adjusted odds ratios for GHQ cases associated with the main types of employment transitions. In comparison with those people who had transitions within different types of formal employment, those who moved in either direction between employment and non-employment, and those who moved within different categories of non-employment were significantly more likely to be a GHQ case after the transition, having controlled for age and sex (column one).
Model 1: the effects of broad employment transition types on psychological distress*—multivariate models
In column two a binary variable (sick) was added to the model to identify those people who were unable to work because of ill health either before or after their transition. As can be seen, this reduced the odds ratios for all of the different transitions, but they remained statistically significant when compared with transitions within paid employment. This suggests that although some of the association between employment transitions and mental health was attributable to movements in and out of long term sick leave, this only contributed a minor part of the explanation.
In column three a binary variable was added to model one to indicate whether or not people were GHQ cases before the transition. The odds ratio for this variable was large (OR = 3.66, 95% CI = 3.31 to 4.06) and highly significant, showing that being a case after an employment transition was highly associated with being a case before. This may be the result of health selection out of employment or the added stress experienced during employment in anticipation of the transition. However, the odds ratios for the employment transition variables did not change substantially and remained statistically significant after the addition of the variable for GHQ caseness before the transition, which suggests that although health selection played a part in the association it did not account for all of it. Finally, column four controls for both of these factors. Each transition type was statistically significantly associated with GHQ caseness within 12 months of the transition having occurred compared with transitions within the formal employment sector.
In all the models, women were significantly more likely to be a GHQ case after a transition than men and a non-linear trend with age existed that peaked in the 35–44 year age group. Variables indicating whether another transition intervened between the transition of interest and the GHQ measure, the number of previous transitions, and the number of months from the GHQ measure until the transition were included in the model. These were not independently significant and had no effect on the employment transition odds ratios.
Detailed transitions from formal employment to non-employment
As table 3 shows, transitions from paid employment into non-employment, except for those into study, adversely affected mental health when compared with transitions within paid employment. Both men and women were twice as likely to become GHQ cases after transition from employment to unemployment, and two to three times as likely to become cases after transition to long term illness. In addition, for women the odds of becoming a GHQ case increased by about 50% for transitions to maternity leave and to family care. A transition to study was associated with a halving of the odds of becoming a GHQ case for men, but not for women. The odds ratios for transitions to unemployment, family care, and long term illness were larger for those people whose GHQ was measured in the first six months after the transition had occurred than for those measured after this period, suggesting that the proximity to the transition was important for its effect on mental health (data not shown).
Model 2: the effects of detailed transitions from employment to non-employment on psychological distress*—multivariate models
Detailed transitions from non-employment to formal employment
Table 4 summarises the results from the multivariate models for transitions from non-employment into formal employment. Compared with those who remained non-employed, becoming formally employed was generally associated with a reduced risk of being a GHQ case. This was significant for transitions from study for men and from family care for women. Surprisingly, although transitions from unemployment to paid employment were associated with improved psychological wellbeing this was statistically significant for women only. When the models were limited to those whose GHQ was measured within six months of the transition having occurred, the associations were stronger; however for men unemployment was still not statistically significant. A further examination by age group found that re-employment only improved mental health for men aged 41–74 years after a transition from unemployment.
Model 3: the effects of detailed transitions from non-employment to employment on psychological distress*—multivariate models
DISCUSSION
This study is unique in using transition information from a British longitudinal dataset to examine the association between the full range of transitions between employment and non-employment, and vice versa, and changes in psychological wellbeing for men and for women separately.
The results from this study contribute to the evidence that becoming unemployed is associated with increased psychological distress. This is consistent with a recent analysis of BHPS data that found a similar association between losing a job and psychological distress.12 Furthermore, the separate analyses for men and for women in this study, not often found in the literature, showed that the strength of the association was similar for both sexes. In addition, there was a higher prevalence of GHQ cases during paid employment before becoming unemployed compared with people who entered other non-employment categories (except for long term illness) that may have been related to anticipation of unemployment21 or to health selection effects.
Previous studies show that retirement is beneficial to psychological wellbeing.1 However, the results from this study did not show a significant effect on psychological distress, either positive or negative, for transitions into retirement compared with people who changed jobs. The results from the Whitehall II study found an improvement in mental health after retirement only for those in high employment grades only.5 This may explain the lack of association found here in a general population sample, and requires further examination.
While studies of unemployment and health are comparatively common, few papers consider the full range of employment transitions that men and women experience. A unique aspect of this study is that it shows the significant increase in psychological distress associated with leaving formal employment to start maternity leave or a period of family care. This transition is mainly neglected in the literature and its association with decreases in mental wellbeing is unlikely to be the result of health selection, as generally only healthy women have children.22,23 By definition those on maternity leave were having a baby and planned to return to their jobs afterwards. Those undertaking “family care” were a more mixed group, although most were women (95%). The prevalence of postnatal depression among some new mothers24 is obviously a more serious manifestation of the raised GHQ levels identified here for those on maternity leave. Some authors have questioned the validity of the GHQ during pregnancy and motherhood25,26 and it is therefore possible that by identifying somatic as well as psychological symptoms there may be overestimation of rates of psychological distress in this sub-population. More detailed analyses (results not shown) suggested that for family leave, the lowest prevalence of GHQ cases was among those with no children or caring responsibilities, while the highest was for those who had significant caring responsibilities, either looking after both children and others, or doing more than 20 hours per week caring for a sick person. Poor psychological health among carers has been found in other studies.27–29 Those respondents only looking after children also had comparatively high levels of GHQ caseness.
This study also makes an important and new contribution to the literature by examining transitions from non-employment to formal employment. In general studies tend to examine the harmful effects of negative social experiences rather than beneficial effects of positive ones.30 A number of studies have found improvements in mental health after re-employment from unemployment, which is supported by the results presented here.2 However, this study also finds beneficial effects of transitions into paid employment from full time study and family care that remained after controlling for psychological distress and ill health before the transition. An unexpected finding was the beneficial effect of transitions from employment into full time education and vice versa for young men. There is some evidence that school leavers who go on to higher education have better psychological wellbeing than those who become unemployed.31,32 In this study, most transitions between paid employment and full time education in either direction occurred in the 16–24 year age group for both men and women. The duration of jobs before entering full time education was on average shorter than those for older age groups. The associations seen, therefore, may simply represent the influence of temporary jobs before and during periods of study.
Key points
-
For both men and women, transitions from paid employment into either unemployment or long term illness were associated with poor mental health.
-
Transitions into maternity leave or family care were also associated with poor mental health for women.
-
Transitions from non-employment into paid employment were associated with good mental health.
-
The effects of transitions on mental health seem to be felt most strongly within the first six months of the transition.
-
Poor mental health did not have a strong influence on selection into non-employment.
Policy implications
-
In general, transitions from employment into non-employment, for whatever reason, may be associated with psychological distress. This should be anticipated before leaving work and prepared for. Additional social support after the transition may reduce this distress.
-
The provision of resources to assist people faced with employment termination may help prevent psychological distress by improving the chance of finding new employment in a shorter period of time.
-
Increased social support to new mothers, those who stay at home with their children, and other carers should also reduce the higher levels of psychological distress associated with these transitions.
The effect of health selection, that is, healthier people are more likely to become employed than less healthy people, was evident from the results. Among people who were non-employed, there was a higher prevalence of GHQ cases before the transition for those who changed categories within non-employment compared with those who entered paid employment. This shows that people with considerable psychological distress during non-employment were less likely to become employed.33 Multivariate analyses were able to show an association between transitions to unemployment, and other non-employment roles, and psychological distress after controlling for being a GHQ case before the transition. Prior psychological distress, therefore, did not seem to have a strong influence on selection into non-employment.
The effect of time between the GHQ measures and the transitions, both before and after the transition, was considered in the analysis. Firstly, the effect of worsening mental health closer to the end of an employment episode21 was considered by including time from GHQ measurement until the transition in multivariate models. This was not significant. Secondly, sub-analyses were undertaken based on the time from the start of a new episode and the subsequent GHQ measure to check if the effect of a transition was related to time. The results from this indicated stronger associations and varying patterns of relations within the first six months after transition, suggesting that the effect on health is greater the more recent the transition. These results should be interpreted with caution because the data were from subgroups of the study population—those whose interview date and hence GHQ measurement occurred within six months of the transition compared with those interviewed more than six months after the transition. Nevertheless, other studies have found that long term unemployment is particularly detrimental for mental health.34
In conclusion, the results from this study highlight two important issues; employment transitions have varying relations with psychological distress depending on the type of transition, and are different for men and for women. It also suggests that the effect of employment transitions is felt most strongly within the first six months. The results have some important policy implications. The provision of resources to assist people faced with employment termination, for example counselling, skill development, careers advice, and financial management advice, may help prevent psychological distress and improve the chance of finding new employment in a shorter period of time. Increased social support to new mothers, those who stay at home with their children, and other carers should also reduce the higher levels of psychological distress associated with these transitions. Initiatives such as Newpin, which provides peer support to mothers, have been shown to reduce depression35 and respite care and support can improve the wellbeing of carers.36
Acknowledgments
The data used in this paper were made available through the UK Data Archive. The data were originally collected by the ESRC Research Centre on Micro-social Change at the University of Essex (now incorporated within the Institute for Social and Economic Research). We have made particular use of the work life history file developed by Brendan Halpin14 to whom we are grateful. Neither the original collectors of the data nor the archive bear any responsibility for the analyses or interpretations presented here.
REFERENCES
Footnotes
-
↵* Full details concerning the design of the BHPS and the sampling strategy can be found in Taylor.13
-
↵† For brevity the term “long term illness” in the data tables relates to the occurrence of the transition, “sick” relates to the derived indicator variable.
-
↵‡ Tables of these results can be obtained from the authors if desired.
-
Funding: this project is funded by the Medical Research Council Health Services and Public Health Research Board’s Health of the Public Programme (strategic project grant number 51878).
-
Conflicts of interest: none declared.