Article Text

Abstract
Study objective: To explore how the increased supply of coronary bypass operations and angioplasties from 1988 to 1996 influenced socioeconomic and gender equity in their use.
Design: Register based linkage study; information on coronary procedures from the Finnish Hospital Discharge Register in 1988 and 1996 was individually linked to national population censuses in 1970–1995 to obtain patients’ socioeconomic data. Data on both hospitalisations and mortality attributable to coronary heart disease obtained from similar linkage schemes were used to approximate the relative need of procedures in socioeconomic groups.
Setting: Finland, 2 094 846 inhabitants in 1988 and 2 401 027 in 1996 aged 40 years and older, and Discharge Register data from all Finnish hospitals offering coronary procedures in 1988 and 1996.
Main results: The overall rate of coronary revascularisations in Finland increased by about 140% for men and 250% for women from 1988 to 1996. Over the same period, socioeconomic and gender disparities in operation rates diminished, as did the influence of regional supply of procedures on the extent of these differences. However, men, and better off groups in terms of occupation, education, and family income, continued to receive more operations than women and the worse off with the same level of need.
Conclusions: Although revascularisations in Finland increased 2.5-fold overall, some socioeconomic and gender inequities persisted in the use of cardiac operations relative to need. To improve equity, a further increase of resources may be needed, and practices taking socioeconomic and gender equity into account should be developed for the referral of coronary heart disease patients to hospital investigations.
- equity
- coronary operations
- CHD, coronary heart disease
- CABG, coronary artery bypass graft
- PCTA, percutaneous transluminal coronary angioplasty
Statistics from Altmetric.com
- CHD, coronary heart disease
- CABG, coronary artery bypass graft
- PCTA, percutaneous transluminal coronary angioplasty
In Finnish health care, equity is understood to mean providing health care for all, universal coverage of and equal access to care, and use of services according to need.1 Since the 1960s these objectives have been stated repeatedly in various Finnish health policy documents. In the 1990s the equity goal was further strengthened by including it in the decrees on social rights in the constitution and in legislation on patients’ rights.2
Several studies on the socioeconomic distribution of overall ambulatory and hospital services have shown that although the Finnish healthcare system is in general fairly equitable,3,4 socioeconomic discrepancies exist in the use of surgical procedures.5–7 There were particularly wide disparities between social groups in the rates of coronary artery bypass operations in the late 1980s; for example, 26% more operations were performed for upper white collar than blue collar men,6 despite mortality from coronary heart disease (CHD) among blue collar men being nearly twice as high. Similar, but less pronounced discrepancies were observed among women. The supply of services also influenced these inequities; socioeconomic gradients tended to be somewhat steeper in areas with low overall rates of coronary operations.
In the early 1990s, the Finnish healthcare system experienced great upheaval. The economic depression in 1991–1994 slashed over 10% of Finnish GDP and resulted in cuts of 15% in total health expenditure per capita.8 In general hospital care spending was reduced by about 5%. At the same time, however, the productivity of the Finnish hospital sector, increased strongly. Discharges in the general hospitals rose by 12% and outpatient visits by 30%.9 In CHD treatment the number of bypass operations (CABG) more than doubled from 1988 to 1996, from 43 to 89 per 100 000, and the number of percutaneous transluminal coronary angioplasties (PTCA) increased even more, from 6 to 41 per 100 000.
This study set out to explore how these changes, particularly the marked increase in resources for invasive treatments of CHD, influenced socioeconomic and gender equity in the use of coronary revascularisations. We investigated the socioeconomic and gender disparities in the use of CABG and PTCA in Finland in relation to the need for these procedures in 1996, and compared the findings with the situation in 1988.6 We also charted the distribution of coronary angiographies in 1996.
METHODS
We established the rates of coronary procedures and hospital utilisation for CHD for all patients aged over 40 years for 1988 and 1996 from the Finnish Hospital Discharge Register, covering all public and private hospitals in Finland. In 1988, five public and two private hospitals offered revascularisation procedures. In 1996, coronary procedures were performed in eight public and three private hospitals, of which two public hospitals provided only angiographies. The Discharge Register records the patient’s residence, personal identification number, and clinical data, such as three diagnoses, operation room procedures with two procedure codes in 1988 and three codes in 1996, and the patient’s discharge status. In 1988, diagnoses were coded according to the Finnish version of the 9th revision of the International Classification of Diseases and in 1996 by the 10th revision. In both years, surgical operations were coded according to the classification of procedures by the Finnish Hospital League.10 This classification does not contain catheterisation procedures, but from 1994 onwards coronary angiographies and angioplasties have been recorded with supplementary questionnaires attached to cardiac patients’ discharge reports. For 1988, data on catheterisation procedures were not available. However, according to the aggregate data collected by the Finnish Heart Association the total number of angioplasties in 1988 was a mere 272, corresponding to 11.4% of all coronary revascularisations.11,12
The data accuracy of the Finnish Hospital Discharge Register was evaluated in the 1980s and found to be generally good. Moreover, about 95% of hospital discharges and 90%–95% of surgical procedures were recorded in the register.13–15 The register for 1988 was estimated to have covered over 90% of all 1988 bypass operations in Finland.6 In 1996, according to a comparison with the aggregated data collected by the Finnish Heart Association, our data comprised over 95% of coronary bypass operations and angioplasties and 85% of angiographies.11 The lower coverage for catheterisation procedures is partly attributable to procedures performed for ambulatory patients, which are not required to be reported to the discharge register.
To obtain the socioeconomic data, the procedure data from the 1988 Hospital Discharge Register were linked by personal identification number to the 1987 population census and to occupational data from the 1970, 1975, 1980, and 1985 censuses. Correspondingly, the 1996 procedure data were linked to the 1995 population census and to data on occupation in the earlier 1970–1990 censuses. The social class of employed persons was obtained from the most recent census. Married women were classified using their own occupation or, if not employed, according to their husband’s occupation. The social class of retired persons was derived from their most recent pre-retirement occupation in the censuses of 1990, 1985, 1980, 1975, or 1970. The data on the population at risk came from the 1987 and 1995 censuses.
In both years social class was defined identically according to the person’s occupation as follows:
Upper white collar employees: upper level administrative, managerial or professional employees
Lower white collar employees: lower level administrative or clerical employees
Blue collar workers: skilled or unskilled manual workers
Farmers: farmer employers or farmers on own account
Others: employers, self employed workers, students or occupation unknown
The level of education was classified into three categories.
High: university degree or a qualification requiring 13 years or more of education.
Intermediate: secondary school matriculation requiring 10–12 years of education.
Low: basic education of less than 10 years.
Disposable income was derived from the 1988 and 1995 registers on taxes and welfare benefits. It was adjusted for family size using the OECD equivalence scale, where the first adult of a family is weighted as 1.0, other adults as 0.7, and children under 18 years old as 0.5.16
The relative need for revascularisations in socioeconomic groups was assessed using hospitalisation and mortality attributable to CHD as proxies. Hospital use in 1988 and 1996 attributable to CHD was derived from the same datasets as data on coronary procedures. As proxy for need for bypass operations in 1988, data on mortality from CHD in the age group 40–69 were calculated from a dataset linking the 1986–1991 cause of death registers, the 1985 population census and supplementary occupational data from the 1970–1985 censuses. As revascularisation rates were analysed for the age group 40–69 because of the low numbers of procedures on older patients, CHD mortality in 1986–1991 was established for this age group. Because 1995 was the last year with mortality data available, we proxied the 1996 need from the 1991–1995 CHD mortality linked to the population censuses of 1990 and to supplementary occupational data in the 1970–1985 censuses. The methods for the linkage procedure, calculation of person years, and mortality figures are described in detail by Valkonen et al.17 Socioeconomic data in the datasets for procedures, hospitalisations, and mortality were based on the same primary data sources and classified identically.
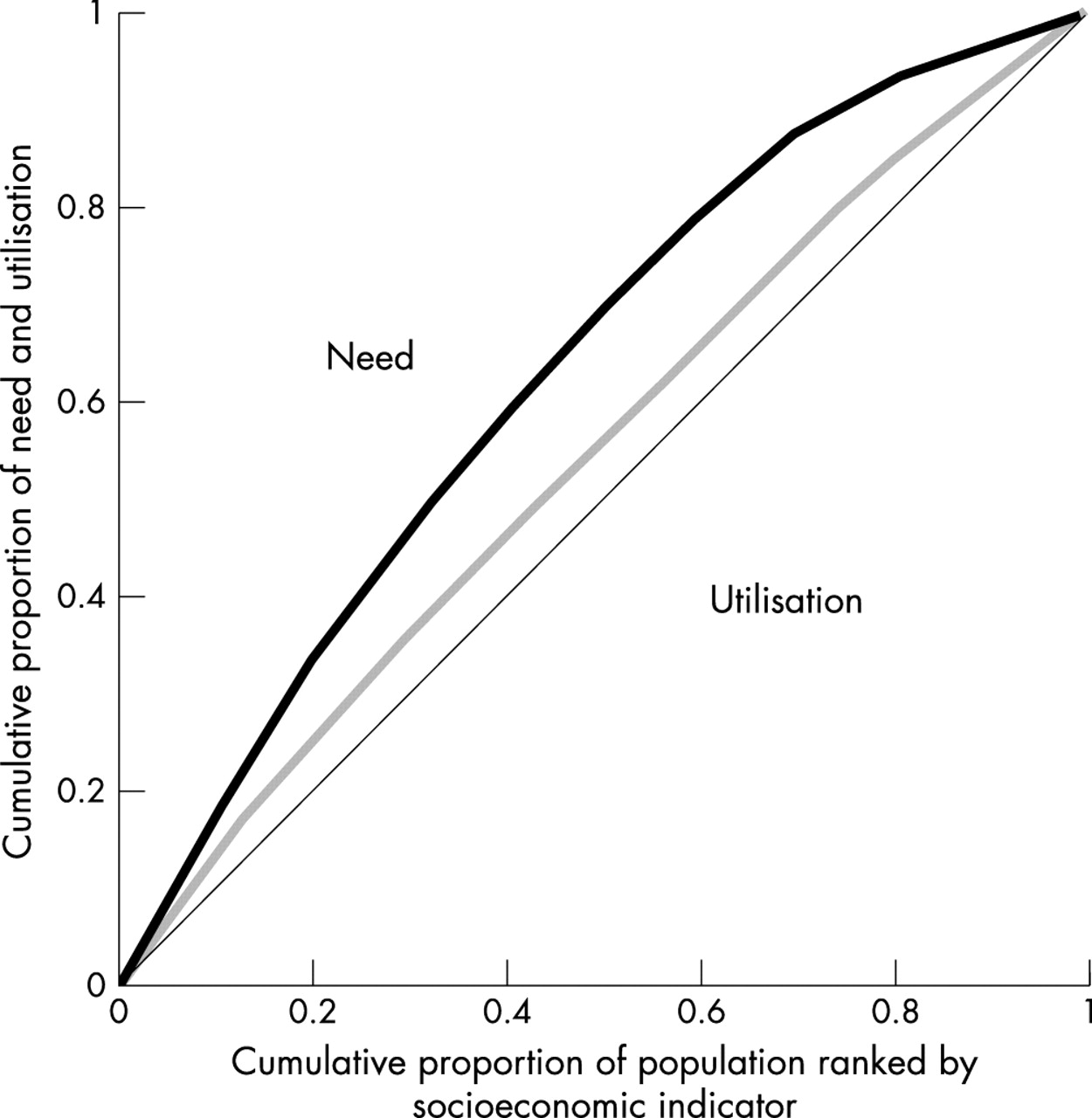
To compare the need for coronary procedures with their use in socioeconomic groups among women and men, age specific and gender specific mortality and annual risk of hospitalisation for CHD in social classes as well as educational and disposable income groups were compared against the respective rates of revascularisations and coronary angiographies. Five year age categories were used in plotting death rates against operation rates. Moreover, we calculated inequity indices based on Kakwani’s index of tax progressivity from the same data. This index is calculated from the concentration curves of need and use (fig 1). In the theoretical figure the horizontal axis represents the cumulative proportion of the population arranged by rising socioeconomic status, and the vertical axis depicts the cumulative proportions of need and use of services. The value of Kakwani’s index equates two times the area between the need and use concentration curves dived by the area of the whole square. The value of the index varies between −2 and 1. If the concentration curve for utilisation is below the curve for need, the index value is positive, depicting the distribution of utilisation favouring the better off. The details of the index calculation were presented by Wagstaff et al,18 who proposed its use for assessing horizontal equity in health services utilisation. Because the index assumes an ordinal classification of socioeconomic variables, the occupational categories for “farmers” and “others” were excluded.
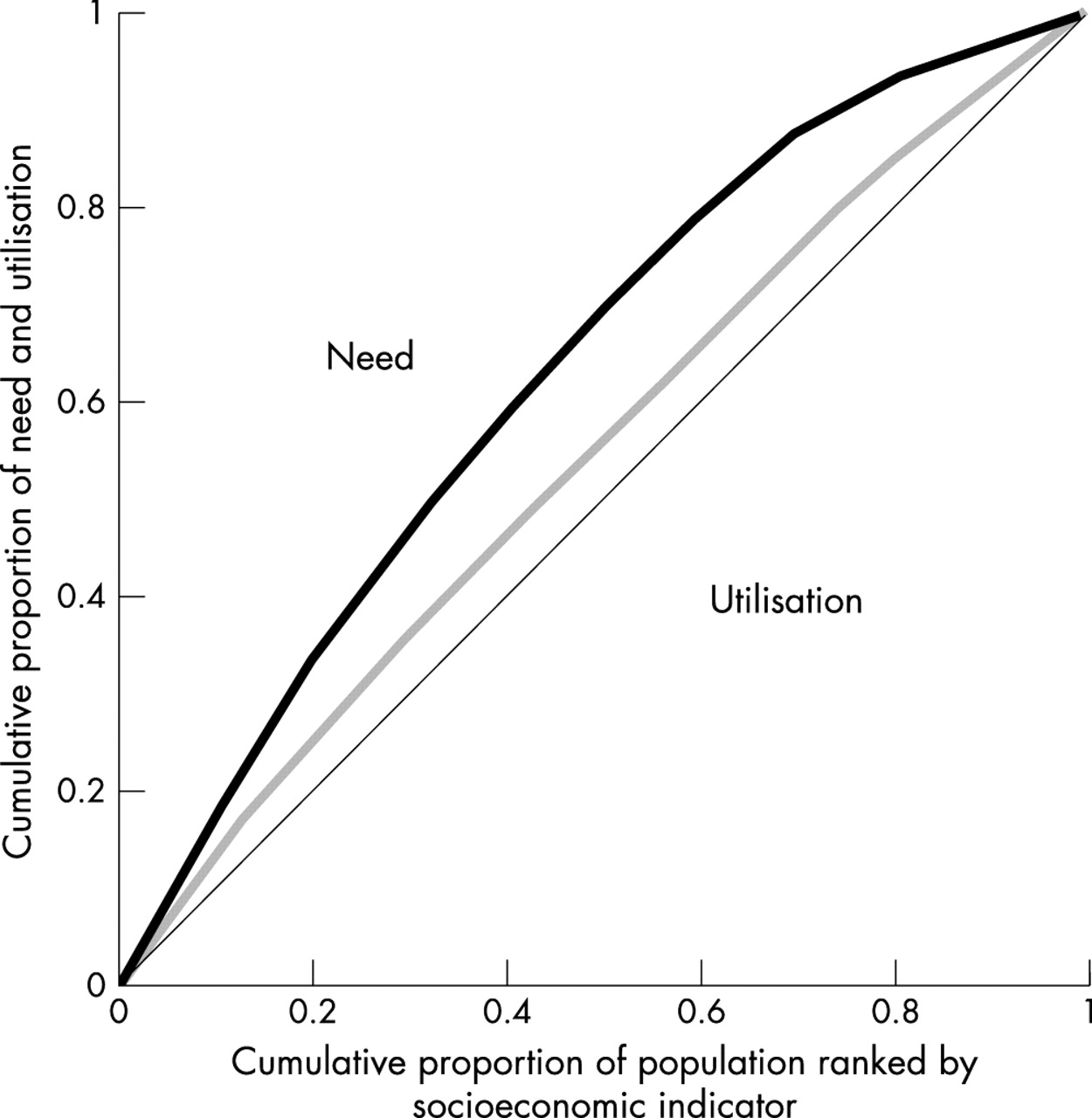
A theoretical example of the calculation of Kakwani’s inequity index: the index value equates double the area between the need and utilisation curves.
To assess the influence of the regional supply of revascularisations on gender and socioeconomic gradients in operation rates, we estimated the correlation between the overall procedure rate in each hospital district and the regional rate ratios for socioeconomic and gender groups using multilevel Poisson regression. Our outcome was the number of procedures observed in groups defined by age, gender, and socioeconomic status within each hospital district. We adjusted for population size and age structure by including the population at risk as an offset. We obtained point estimates of the correlation coefficients and their 95% confidence intervals from the posterior distributions estimated using Markov Chain Monte Carlo (MCMC).19 Because of low numbers of procedures in some of the 21 hospital districts we studied only the rate ratios for blue collar and white collar groups, for those with low education (≤9 years) and more than low education (≥10 years), and for those in the two lowest and two highest income quintiles. Analyses were carried out using MlwiN.20
RESULTS
According to the 1996 Finnish Hospital Discharge Register, Finnish hospitals performed 3510 coronary bypass operations, 1709 angioplasties and 7764 angiographies for patients aged 40 to 69 years. The numbers corresponded to 440 coronary revascularisations and 597 angiographies per 100 000 men and 121 and 232 per 100 000 women. The study data for 1988 comprised only coronary artery bypass procedures. In 1988, patients aged 40–69 underwent 1779 bypass operations altogether, corresponding to 185 for men and 35 for women per 100 000. Making allowances for the lack of data on angioplasties in 1988, the male rate of coronary revascularisations increased by about 140% and the female rate by 250% over the study period.
Table 1 presents coronary operations, hospital utilisation, and mortality from CHD for men and women aged 40 to 69 years. Along with the increasing overall rates of coronary procedures, socioeconomic differences in operation rates changed between 1988 and 1996. While male age adjusted rates for coronary bypass operations in 1988 showed a pronounced gradient favouring the better off, independent of socioeconomic indicator used, no systematic socioeconomic trends existed in rates for coronary revasularisations or angiographies in 1996 (table 1). However, according to all three socioeconomic indicators male mortality from CHD in 1991–1995 systematically increased towards the lower socioeconomic groups. In both study years hospitalisations attributable to CHD displayed higher rates in the men worse off in terms of social class and education. However, in the lowest income group risk of hospitalisation attributable to CHD was lower than in middle groups in both years. The pattern was similar for men aged 70 years and older in hospitalisations attributable to CHD in 1996. In operation rates among elderly men a gradient favouring the better off was observed (table 2).
Age adjusted rates, Finnish population in 1996 used as standard population, and 95% confidence intervals (95% CI) for coronary artery bypass grafting (CABG), percutaneus transluminal coronary angioplasty (PTCA), coronary angiography, hospital utilisation attributable to coronary heart disease (CHD) and mortality from coronary heart disease by social class, education, and family disposable income in 1988 and 1996 in Finland, men and women aged 40–69
Age adjusted rates and 95% confidence intervals (95% CI) for coronary artery bypass grafting (CABG), and percutaneus transluminal coronary angioplasty (PTCA) in Finland by social class, education, and family disposable income in 1996, men and women aged 70 years and older
For women aged 40 to 69 years, the 1988 socioeconomic differences in bypass operations were less distinct; no clear gradient was found according to any socioeconomic indicator used (table 1). In 1996, gradients in the rates of coronary revascularisations and angiographies favoured the lowest groups according to social class and education, while according to income the highest rates occurred among women with intermediate family incomes. Female mortality in 1991–1995 and the 1988 and 1996 annual risks of hospitalisation attributable to CHD showed similar overall gradients for socioeconomic indicators used: the lower the socioeconomic status the higher the mortality and hospitalisation rate. This was also true for women aged 70 years and older in 1996. For this age group the pattern for the operation rates showed no clear gradient (table 2).
Figure 2 presents age specific curves for revascularisation rates in 1988 and 1996 for white collar and blue collar men and women against mortality from CHD for 40 to 69 year olds. Figure 2 shows that in both study years white collar male employees received more operations than blue collar workers with the same level of need, indicated by CHD mortality. For women the results were similar but the relative differences smaller, and the curves crossed for the older age groups in 1996. However, for both genders the distances between the curves of procedure rates and mortality in socioeconomic groups diminished from 1988 to 1996. Corresponding patterns emerged for men and women when we plotted similar curves for education and disposable income groups and when we examined angiographies instead of revascularisations in 1996. For the lowest income group, age specific curves also reproduced the diverging relation of utilisation and need indicators in comparison to other income groups (see table 1)—that is, the exceptionally low level of operation rates compared with mortality. This was true especially for men and women younger than 60 years. Patients aged 60–69 received comparatively more operations in 1996 than in 1988; the curves declined for older age groups in 1988 but rose in 1996 (fig 2). While few operations in 1988 were performed on patients older than 70 years, in 1996 operation rates markedly dropped only for those aged 80 or more.
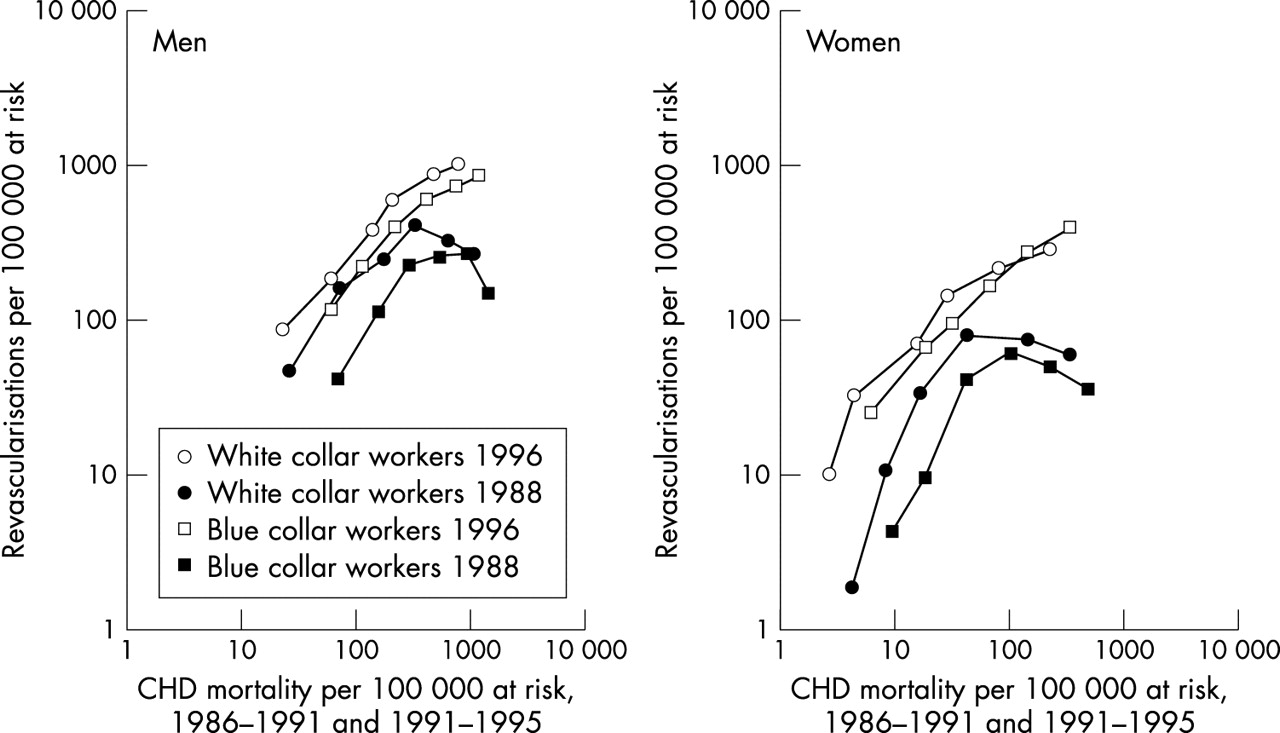
Effect of socioeconomic group on the relation between rates of revascularisations* and mortality attributable to coronary heart disease (CHD); each point describes a five year age band across the age groups 40–69 years, men and women. *1988 CABG and 1996 CABG+PTCA.
We also calculated Kakwani’s inequity indices for the socioeconomic distribution of coronary revascularisations using deaths and hospitalisations attributable to CHD as proxies for need (table 3). Among those aged 40 to 69 all the indices, except that for women’s education, were smaller in 1996 than in 1988, suggesting a more equitable distribution of revascularisations in 1996. The changes in the indices were larger when hospitalisation attributable to CHD was used as a proxy for need. Still, all the index values were positive in 1996, indicating that the distribution of operations favoured higher socioeconomic groups. For age groups over 70 years, Kakwani’s inequity indices were mostly concordant with the results for those aged 40–69. However, the indices were somewhat higher when annual risk of hospitalisation and lower when mortality attributable to CHD were used as proxy for need. Furthermore, the indices for angiographies for those aged 40 and more closely resembled to those for revascularisations in 1996.
Kakwani’s inequity indices for the socioeconomic distribution of revascularisations in Finland using mortality and annual risk of hospitalisation attributable to coronary heart disease (CHD) as proxies for need, 1988 and 1996, men and women aged 40–69
To study the influence of the supply of coronary revascularisations on socioeconomic and gender differences in their utilisation, we analysed the associations between the overall coronary operation rates in the 21 hospital districts and the regional revascularisation rate ratios for women and men and for low and high socioeconomic groups. As an example, figure 3 plots ratios of revascularisation rates among women compared with those for men, and the corresponding rate ratios for blue collar and white collar groups among men against overall hospital district rates in 1988 and 1996. Among all four groups plotted there seems to be a positive association between the overall district rate and the rate ratio, an increase in the overall rate corresponding to an increase in the rate ratio. Our measure of the strength of this association is the correlation coefficient, and estimates of the correlation between the overall rate and the rate ratio—both on the log scale—together with 95% confidence intervals, are presented in table 4. In 1988, there was a clear association between the hospital district rates of coronary revascularisations and the rate ratios for genders and socioeconomic groups among men. For women, the correlation coefficients in 1988 were only significantly different from zero for the correlation between regional operation rates and rate ratios for educational categories. By 1996, the association between the regional supply of coronary operations and trends in operation rates had weakened and only the rate ratios for gender differences and men’s social class differences displayed a statistically significant correlation with overall hospital district rates.
Correlation coefficients and their 95% confidence intervals for the correlation—on the log scale—between the overall coronary revascularisation rates in the hospital districts and the regional rate ratios between genders and socioeconomic groups among Finns aged 40–79 in 1988 and 1996

{kind=link}
{kind=link}
{kind=link}
Coronary revascularisation rate ratios for genders and blue collar and white collar men by overall hospital district revascularisation rate among Finns aged 40–79 in 1988 and 1996.
DISCUSSION
From 1988 to 1996 the resources for invasive treatments of CHD expanded substantially in Finland, as portrayed by the 2.5-fold increase in the total number of coronary bypass operations and angioplasties. In general, older patients, women, and those with low socioeconomic status benefited more than other groups from the increased supply of coronary procedures. However, when we related the procedure rates to the two proxies for the relative need for procedures (mortality from and risk of hospitalisation attributable to CHD), inequities favouring the higher socioeconomic groups in the use of coronary procedures were apparent in both genders in 1988, and although they somewhat diminished they still remained in 1996. Moreover, very low procedure rates in the lowest income group and the association of the regional supply of coronary operations with men’s social class differences in the use of the operations indicated that socioeconomic inequities in access to invasive coronary treatments still prevailed in Finland in 1996.
Key points
-
The rapidly increasing supply of coronary revascularisations in Finland coincided with diminishing socioeconomic and gender disparities in operation rates.
-
However, socioeconomic and gender inequities, particularly pronounced in the elderly population, remained in the use of coronary revascularisations in relation to need.
-
The socioeconomic and gender distributions of coronary revascularisations and angiographies were parallel suggesting that disparities arose before referrals to angiography.
-
Practices taking socioeconomic and gender equity into account should be developed for the referral of CHD patients to hospital investigations.
In our study a clear gender difference was found in revascularisation and angiography rates with women receiving less operations compared with men in Finland. Similar results on angiographies and revascularisations have been reported for instance in the United Kingdom,21 Canada,22 and the United States.23–27 Findings are not completely consistent, as there are some studies reporting no gender differences in coronary procedures.23,28 Additionally, several studies have reported no gender disparity in receiving revascularisations26,29 or bypass operations among patients who had undergone angiography.25,27,28 Because of gender differences in the symptoms, natural history, and prognosis of CHD,30 disparities between men and women in the use of coronary operations are difficult to assess, but in our study a tendency of smaller gender differences in rates in hospital districts with a high overall supply of coronary procedures suggests that gender inequities favouring male patients persisted in access to coronary operations in the mid-1990s.
A potential explanation for socioeconomic disparities in coronary revascularisation rates could be operations performed in private hospitals or on patients treated in the special payment category (pay beds) in public hospitals.7 However, these operations obviously explained only a minor part of the socioeconomic differences observed in 1988 and 1996. For example, of the revascularisations performed on upper white collar employees in 1996, 14% were carried out in the private sector, while the figure was 8% for blue collar workers aged 40 years and older. Consequently, as we calculated the age adjusted rates for revascularisations and angiographies performed in public hospitals, the socioeconomic patterns that emerged were similar to those observed for all procedures in both study years.
In 1988 the influence of pay bed operations on socioeconomic differences in coronary revascularisations was modest.6 As data on pay bed patients were not recorded separately in the National Discharge Register in 1996, the impact of the pay bed system could not be analysed for that year, but other evidence indicates that it remained small. According to statistics on health insurance claims from the Finnish Social Insurance Institution, annual applications by pay bed patients for refunding included only about 30 to 60 bypass operations in the mid-1990s. However, in some specific groups, such as elderly patients, private and pay bed operations may have had some impact on access to services. For instance, the overall amount of revascularisations performed in the private sector was 11%, but among those aged 70 years or more the proportion was almost double, at 19%. The corresponding socioeconomic disparities in operation rates were greatest in these old age groups.
The 1988 hospital discharge data did not encompass angiographies. However, the 1996 results suggest that the socioeconomic differences in the use of coronary revascularisations may have been largely determined by uneven access to angiographies. In 1996 the distributions of coronary revascularisations and angiographies were parallel according to all indicators of socioeconomic status and in both genders. The socioeconomic patterns of Kakwani’s inequity indices for revascularisations and angiographies were also similar. These results correspond to findings in other countries of no or only small differences between genders or income or ethnic groups in revascularisation rates among patients who have undergone angiography.24–26,28,29,31 Consequently, an evaluation of equity in access to invasive cardiac treatments is likely to be biased if based solely on hospital data and ignoring the population at risk and its morbidity. Alter et al drew a similar conclusion from examining access to invasive cardiac procedures after acute myocardial infarction, and reported that access to angiography was the rate limiting step in access to revascularisation.31 One obvious challenge for future research on equity in access to coronary procedures is to disentangle factors contributing to socioeconomic differences in pathways to treatments before angiography and hospitalisation.
Taking account of the potential importance of access to angiography, it is plausible that socioeconomic disparities in coronary operation rates could be caused either by patients’ different ways of seeking care or by physicians’ socially biased referral decisions. Research on this topic in Finland is lacking, but some findings from the United States suggest that patients’ preferences may somewhat explain differences in invasive coronary treatments.32 However, study findings are not altogether consistent.28,33
Finland’s partially two tier system of ambulatory physician services may cause socioeconomic disparities in referrals to invasive CHD treatments. The mandatory health insurance reimburses only part of the costs of private services, with the result that utilisation of private practitioners—about 20% of all outpatient visits to doctors—is clearly concentrated among well off patients.34 As physicians working in private practice are often specialists, they may be more prone to recommend further investigations for their patients than doctors in public health care. The socioeconomic distribution of private sector patients did not change between the late 1980s and mid-1990s.34
The rapid increase in supply of coronary revascularisations in Finland between 1988 and 1996 was more or less expected to be associated with a decrease in socioeconomic and gender inequities in their utilisation. Corresponding results have emerged in other countries. Manson-Siddle and Robinson reported from England that services were socioeconomically equitable in a district with the highest revascularisation rate.35 In another study these researchers reported that additional resources for tertiary cardiology may have reduced socioeconomic inequities in angiography utilisation, although improved equity in revascularisations was not apparent.36 Black et al reported that when the supply of revascularisations increased in the United Kingdom the gender disparity decreased,37 which accords with our result.
However, although the number of revascularisations in Finland increased 2.5-fold from 1988 to 1996, the socioeconomic and gender inequities in the use of cardiac operations in relation to need remained. These persisting inequities may, of cause, be attributable to remaining inadequacies in healthcare resources for coronary revascularisations. When estimating the need for revascularisations in Finland in 2000, a Finnish expert group considered that the need is more than double in near future for angioplasties, while the supply of coronary bypass operations was considered fairly sufficient.38 Some international comparisons support this view; for instance, revascularisation rates after myocardial infarction in the late 1990s were still much lower in Finland than in North America or Australia.39 Furthermore, when comparing revascularisation rates to CHD mortality in western European countries in the mid-1990s, CHD mortality in Finland was the second highest but the revascularisation rate was on the average level.40,41 If this is the case, the further increase of resources might equalise the use of coronary operations in socioeconomic groups. On the other hand, these inequities may largely result from the structure of Finnish outpatient care; heavy reliance on the private sector possibly leads to socioeconomic disparities in overall referrals to CHD investigations. Correction of this potential cause would require other measures, such as developing and intensifying treatment practices in public outpatient care.
REFERENCES
Footnotes
-
Funding: the study was financially supported by the Doctoral Programs in Public Health of University of Helsinki and the Academy of Finland.
-
Conflicts of interest: none.
Linked Articles
- In this issue