Article Text

Abstract
Background: The infant mortality rate (IMR) has been criticised as a measure of population health because it is narrowly based and likely to focus the attention of health policy on a small part of the population to the exclusion of the rest. More comprehensive measures such as disability adjusted life expectancy (DALE) have come into favour as alternatives. These more comprehensive measures of population health, however, are more complex, and for resource poor countries, this added burden could mean diverting funds from much needed programmes. Unfortunately, the conjecture, that DALE is a better measure of population health than IMR, has not been empirically tested.
Methods: IMR and DALE data for 1997 were obtained from the World Bank and the World Health Organisation, respectively, for 180 countries.
Findings: There is a strong (generally) linear association between DALE and IMR (r=0.91). Countries with low DALE tend to have a high IMR. The countries with the lowest IMRs had DALEs above that predicted by the regression line.
Interpretation: There is little evidence that the use of IMR as a measure of population health has a negative impact on older groups in the population. IMR remains an important indicator of health for whole populations, reflecting the intuition that structural factors affecting the health of entire populations have an impact on the mortality rate of infants. For countries with limited resources that require an easily calculated, pithy measure of population health, IMR may remain a suitable choice.
- infant mortality rate
- disability adjusted life expectancy
- population health
- DALE, disability adjusted life expectancy
- IMR, infant mortality rate
Statistics from Altmetric.com
A general measure of population health is useful for comparing the health status of a population over time, or between populations at a single point in time. It permits comparisons of health systems and programmes, and may highlight populations in need of particular attention from health services.1
The infant mortality rate (IMR), defined as the number of deaths in children under 1 year of age per 1000 live births in the same year, has in the past been regarded as a highly sensitive (proxy) measure of population health.2 This reflects the apparent association between the causes of infant mortality and other factors that are likely to influence the health status of whole populations such as their economic development, general living conditions, social well being, rates of illness, and the quality of the environment.
More recently it has been argued that proxy measures of population health like IMR are problematic3; and the past decade has seen IMR fall out of favour. The World Health Report 2000,4 for example, makes no reference to the measure.
Despite starting as indicators of a whole population’s health, measures like IMR often, it is reasoned, become the principal focus of health policy such that health strategies and health priorities are formulated with the proxy outcome measure in mind.3 As a consequence, health policies begin to target the chosen outcome measure, while ignoring the rest of the population for which the outcome measure was supposed to be an indicator. Thus, IMR may decrease, as infant mortality becomes the principal focus of health policy, but the whole population’s health may, unknown to the ministries of health, remain static or even degrade.
This view has lead to the development of more comprehensive measures of population health; for example, the disability adjusted life expectancy (DALE).5 Such measures are intended to (a) be sensitive to changes of health in the whole population, and (b) account for the morbidity associated with non-fatal health outcomes as well as mortality.1
The argument about the dangers of using IMR as a measure of population health has intuitive appeal, highlighting the fact that it derives from a small, non-representative portion of the population and excludes any consideration of non-fatal health outcomes. In contrast, the DALE combines information about life expectancy with information about the prevalence of disabling sequelae at different ages, with a severity weight that reflects the impact of the disability.5
If, however, ministries of health accept the argument against the use of IMR and choose to pursue an alternative measure of population health such as the DALE, they are faced with additional costs and complexity. In developed countries, the collection of the additional data may not be particularly onerous, and in some cases may already be collected. In those countries that are poorest, however, and have the worst population health, the cost of a more “comprehensive” measure may be prohibitive. Even if the cost were not prohibitive, the benefits of adopting a new measure would have to be significant.
In the absence of data, the argument that IMR is a poor proxy measure of population health is mere conjecture. The aim of this study was to examine the relation between IMR and DALE to ascertain the robustness or otherwise of IMR as a measure of population health.
METHODS
The relation between IMR and DALE was examined in all 180 countries for which data were available.
The DALE data for 1997/1999 for the total population at birth in each country were obtained from The World Health Report 2000 (annex table 5).4 The IMR data for 1997 were obtained from the World Bank’s Development Indicators.6
RESULTS
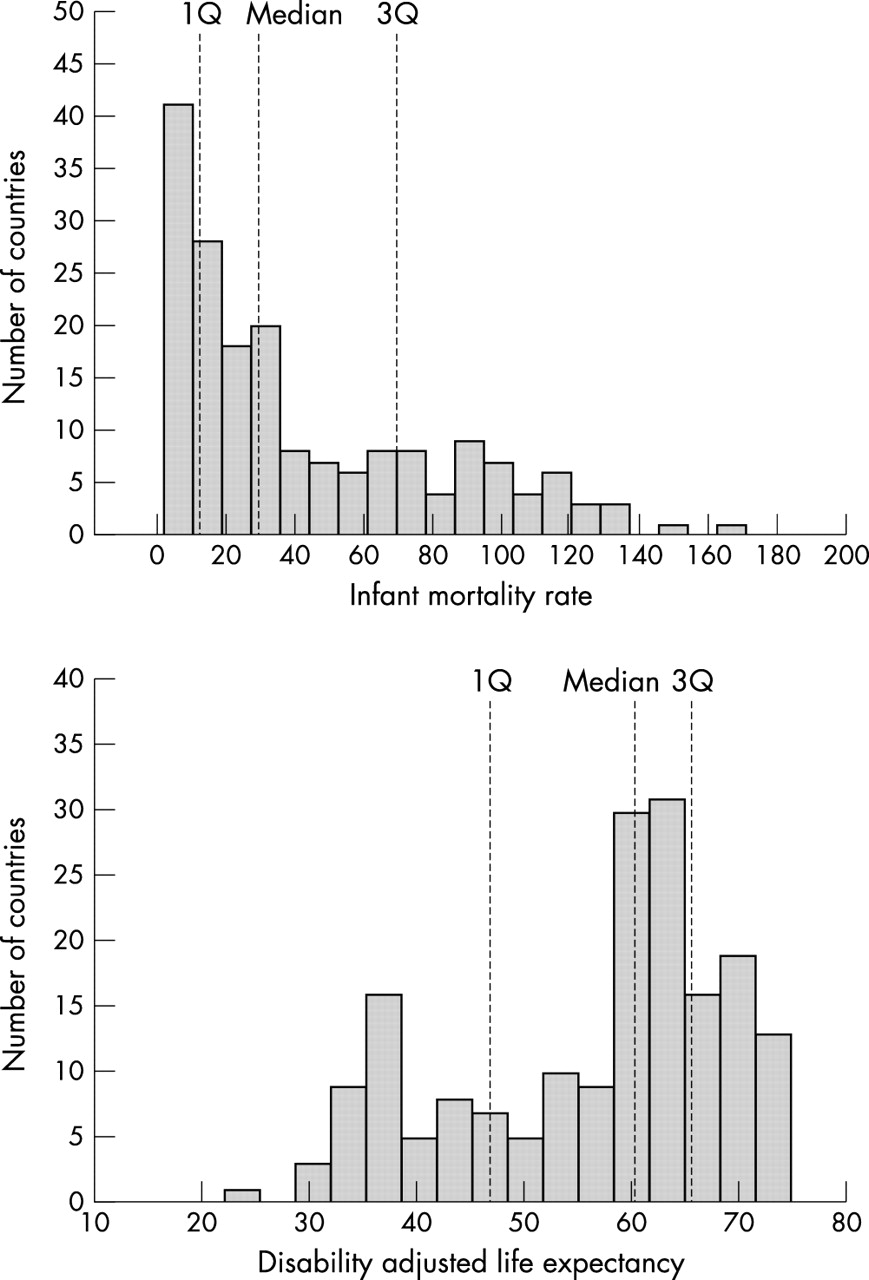
The distribution of IMRs for the 180 countries was skewed with a long right tail. The median IMR was 29 (Vietnam) and the interquartile range lay between 12 (Costa Rica) and 70 (Senegal) (see fig 1). The country with the lowest IMR was Japan (3.7) and Sierra Leone had the highest IMR (170).

Distributions of IMR and DALE with the median, first, and third quartiles shown.
Similarly, the distribution of DALEs was skewed, although, in this case the distribution had a long left tail. The median DALE was 60.5 (Grenada) and the interquartile range lay between 46.9 (Papua New Guinea) and 65.7 (Antigua) (see fig 1). The country with the highest DALE was Japan (74.5) and the country with the lowest was Sierra Leone (25.9).
Figure 2 shows a scatter plot with the regression line of the relation between IMR and DALE.

{kind=link}
{kind=link}
Relation between IMR and DALE with the ordinary least squares regression line shown.
There are a number of striking features about the plot. Firstly, there is a strong (generally) linear relation between IMR and DALE (r=0.91). As IMRs rise, DALEs fall. Secondly, there are a group of countries with very low IMRs for which the linear relation no longer seems to hold. Indeed, as the DALE rises beyond about 69 years the IMR seems to asymptote, suggesting a lower limit to the IMR around Japan’s rate of 3.7. Finally, the countries with low IMRs and high DALEs tend to fall tightly around the regression line, whereas the countries with high IMRs and low DALEs are more dispersed around the line (an example of heteroscedasticity). The standard deviation of the DALE for those countries with an IMR less than the median (29) was 4.5 while for those with an IMR greater than the median it was 10.6. A similar pattern was observable in the variability of the IMR data. The countries with an IMR greater than 29 showed the greatest variability in DALE, and they were without exception developing countries.
Key points
-
Infant mortality rate (IMR) had been criticised as a measure of population health because it could skew health resource allocation.
-
The disability adjusted life expectancy (DALE) was adopted in World Health Report 2000 as the preferred measure of population health.
-
The correlation between IMR and DALE is very high (r=0.91).
-
For many countries IMR may remain an effective and cheaper alternative to the theoretically more appealing DALE.
-
We should not throw the baby out with the bath water.
Each of these observations has significant implications for health planners choosing a measure of population health.
DISCUSSION
The strong linear relation between IMR and DALE means that IMR accounts for more than 80% of the variance of the DALE. It suggests that, in general, one measure could stand as a proxy for the other, and either could stand as a proxy for the measurement of population health. Indeed, there is little evidence that IMR is any worse than the DALE as a measure of population health.
The fact that there is greater dispersion around the regression line for the developing countries with IMRs greater than 29 suggests measurement error. The poorest countries with the least developed infrastructure are least able to collect accurate data for the calculation of the IMR or DALE. Furthermore, given that the calculation of the DALE requires the collection of more data than is required for the calculation of IMR, one might speculate that the DALE has more opportunity for measurement error to creep in and is, therefore, likely to be a less reliable measure.
If health policy were, as conjectured, going to be unduly influenced by IMR, then one would expect to have observed the effects most in those countries with the lowest IMRs. It is after all those countries with the lowest IMRs that are most likely to have concentrated their efforts on lowering infant mortality to the exclusion of the rest of the population. This should result in an uncharacteristically low DALE inconsistent with the regression line. The presence of the “asymptotic countries” with very low IMRs that sit above the regression line suggests that quite the contrary has occurred and governments have not had their health policies shackled by the use of IMR as an indicator of population health. Between these asymptotic countries however, there is little variation in either their DALE or their IMR, and this suggests that, for them, more sensitive measures of population health may be required.
The fact that the IMR and the DALE are so highly correlated merely goes to reinforce the intuition that the causes of infant mortality are strongly related to those structural factors like economic development, general living conditions, social well being, and the quality of the environment, that affect the health of entire populations. This also goes some way to answer why it is that a measure of pure mortality in infants could be so highly correlated with a measure of mixed mortality and morbidity over an entire population that includes dimensions of disability and severity.
Furthermore, because IMR is sensitive to structural changes as well as disease epidemics, it becomes an important indicator of “here and now” effects. Rapid changes in the determinants of population health captured by changes in IMR may be slow to be reflected in DALE, which is influenced by factors such as long term survival and morbidity—mirrored in features like birth cohort effects.
CONCLUSION
The IMR remains a useful and comparatively inexpensive indicator of population health. Its explanatory power is very similar to that of the DALE.
That is not to say that the collection of additional epidemiological data about the health of a population would not be advantageous. Multiple measures, particularly measures that can be disaggregated by age, gender, health condition, socioeconomic status, etc, will always be important for planning. However, if resources are limited, and a pithy, uncomplicated measure of population health is required, then countries with IMRs greater than 10 would seem to be safe using IMR as the indicator.
Acknowledgments
We would like to thank the two anonymous reviewers for contributing their ideas to the final form of this paper.