Article Text

Abstract
STUDY OBJECTIVE To analyse trends in socioeconomic differences in cardiovascular disease risk factors among an urban Chinese population using educational attainment as the socioeconomic indicator.
DESIGN Population surveys with randomly selected independent samples were carried out in 1989 and in 1996. Educational attainment, blood pressure, body mass index, cigarette smoking and lack of leisure time physical activity were determined.
SETTING Urban areas of the city of Tianjin, China.
PARTICIPANTS A total of 14 275 respondents aged 25–64 years.
MAIN RESULTS Diastolic blood pressure increased and the proportion of people without leisure time physical activity decreased in both sexes during the study period. The prevalence of smoking and the number of cigarettes smoked daily increased significantly among men. Smoking decreased in the least educated men and increased in those who had studied at least to college level. Body mass index decreased across all educational strata in women, but blood pressure increased in women with at least college level education.
CONCLUSIONS These data reveal a different picture in trends in the association of education and cardiovascular risk factors from those depicted in developed countries. This highlights the need for an effective intervention programme in the study population.
- trends
- socioeconomic status
- cardiovascular disease risk factor
Statistics from Altmetric.com
There is abundant epidemiological evidence that socioeconomic status (SES) is inversely and consistently associated with cardiovascular disease (CVD) morbidity, mortality and levels of CVD risk factors in developed countries.1-5 Over time, the differences in the occurrence of CVD6 and the level of CVD risk factors7-9 between higher and lower socioeconomic groups have even become accentuated, though total CVD mortality is drastically falling in the affluent societies.10
CVD is emerging as a major cause of death in developing countries.11 The association of SES and CVD in developing nations is not as consistent as those observed in developed countries. Some studies have indicated that SES is inversely associated with the occurrence of CVD12 and the level of CVD risk factors,13-15 whereas there are studies revealing an opposite trend.16-19 China is the largest developing country in the world, CVD has become the major cause of death especially in urban areas.11 20 Two studies13 14 indicated an inverse association of SES and CVD risk factors in urban populations of China. To our knowledge, there has been no previous study reporting the trends in socioeconomic differences in CVD risk factors in the Chinese population. The purpose of this paper was to analyse trends in educational differences in CVD risk factors in the urban population of Tianjin, China between 1989 and 1996.
Methods
The city of Tianjin, with a population of nine and a half million, is the third largest city in China. Four million of the population lives in six urban districts. Mortality from heart diseases and stroke accounted for 51–56% of all deaths in the mid-1980s. The Tianjin Project was started in 1984 to find a way for preventing and controlling CVD in China.21 The baseline survey for a community-based intervention programme was conducted in 1989.22 A five year follow up survey was carried out in 1996. For both surveys, independent random samples were drawn using two stage sampling. Firstly, altogether eight communities in 1989 and 14 communities in 1996 were drawn randomly with at least one community from each of the six urban districts. In the second stage, samples stratified by gender, 10 year age group and community were taken from the local population registers. Altogether 19 300 people aged 15–69 years were examined with overall participation rates of 92–100%. In all, there were 14 046 participants in 1989 and 4000 participates in 1996. This study was restricted to those respondents aged 25–64 years (table 1).
Sample structure by sex, age, and year in this study
Self reported education level was divided into three categories: 0–6 years (less than elementary school studies), 7–12 years (middle to high school studies) and 13 years or more (more than college studies). The participants were classified as current smokers—persons regularly smoking at least one cigarette each day during the past 30 days—and non-smokers. Respondents who reported that they had less than one time leisure time physical activity on average per week were considered as having a lack of exercise.
Anthropometric measurements were done in the local health centres by the intensively trained local public health workers. Blood pressure was measured from the right arm using a standard mercury sphygmomanometer after five minutes of rest with the subject in the sitting position. The fifth phase Korotkoff sound was recorded as the diastolic pressure. The mean value of the two blood pressure measurements was used for the analysis. Hypertension was defined as systolic blood pressure ⩾ 140 mm Hg or diastolic blood pressure ⩾ 90 mm Hg, or both. Height and weight measurements were taken using a stadiometer and beam balance scale with subjects wearing usual light indoor clothing without shoes. Height and weight were measured twice and the mean values of the readings were used for the analysis. Overweight was defined as 25 ⩽ body mass index (kg/m2) < 30 and obesity as body mass index ⩾ 30. CVD risk factor clustering was also assessed by people who had more than two of the three CVD risk factors (hypertension, being overweight or obesity and cigarette smoking).
Differences in CVD risk factors between educational attainment, study year and time trends in the differences (interactions of education and study year) were examined by analysis of covariance for continuous variables and logistic regression analysis for categorical variables.23 The mean age of the study sample in 1996 was younger than that of the 1989 survey. This is because of the relatively fewer number of subjects aged 55–64 years in 1996. To improve the statistical power, we report the results of people who were overweight or obese in the same group as only 4% of men and 8% of women were obese (body mass index ⩾ 30) in the study sample. Also, when assessing cigarette smoking in women by education level between the study year, we have combined the two higher educational categories because there was only one self reported current smoker among the best educated women in 1996.
Results
key points
-
Educational attainment was inversely associated with blood pressure, body mass index, cigarette smoking and lack of leisure time physical activity.
-
No major downward trends in the cardiovascular disease risk factors were observed over the seven year study period.
-
The prevalence of smoking increased in the best educated men and decreased in the least educated.
-
These trends in cardiovascular disease risk factors across educational strata are different from those reported in developed countries.
Over the study period from 1989 to 1996, educational attainment increased significantly in the study population (table 2). There were no downward trends in major unadjusted levels of the CVD risk factors in men over the study period. In contrast, in women unadjusted levels of the CVD risk factors seemed to decrease with the exception of the universal increases of diastolic blood pressure and cigarettes consumed each day among current smokers in both sexes (table 3).
Distributions of educational attainment in people aged 25–64 years by sex and study year in Tianjin, China, 1989 and 1996
Unadjusted means (SD) or proportions (95% confidence intervals) of cardiovascular risk factors in people aged 25–64 years by sex and study year in Tianjin, China, 1989 and 1996
Most CVD risk factors were inversely associated with educational attainment in the study population. The association was more consistent in women than in men (tables 4 and 5). Over the seven year study period, diastolic blood pressure increased and the proportion of people who did not take leisure time physical activity decreased significantly in both men and women. However, 74% of men and 76% of women still did not have leisure time exercise in 1996 (table3).
Age-adjusted cardiovascular risk factor levels in men aged 25–64 years by years of education and study year in Tianjin, China, 1989 and 1996
Age adjusted cardiovascular risk factor levels in women aged 25–64 years by years of education and study year in Tianjin, China, 1989 and 1996
For men, the number of cigarettes smoked daily and the percentage of current smokers increased significantly between 1989 and 1996. The study year by education interaction was statistically significant for the prevalence of smoking, indicating that while the prevalence of smoking declined in the least educated men, it increased steeply in the best educated men over the study period. Nevertheless, the best educated men still contained the smallest proportion of current smokers (table 4).
For women, systolic blood pressure increased in those who had better than college level studies and decreased in the least educated women, although there was no time trend between the two surveys (table 5). Body mass index decreased across all educational groups over the study period.
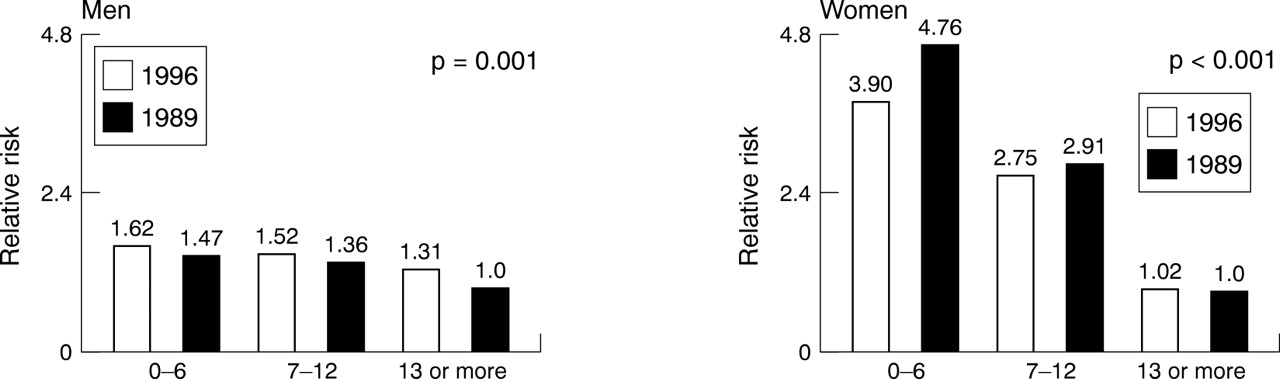
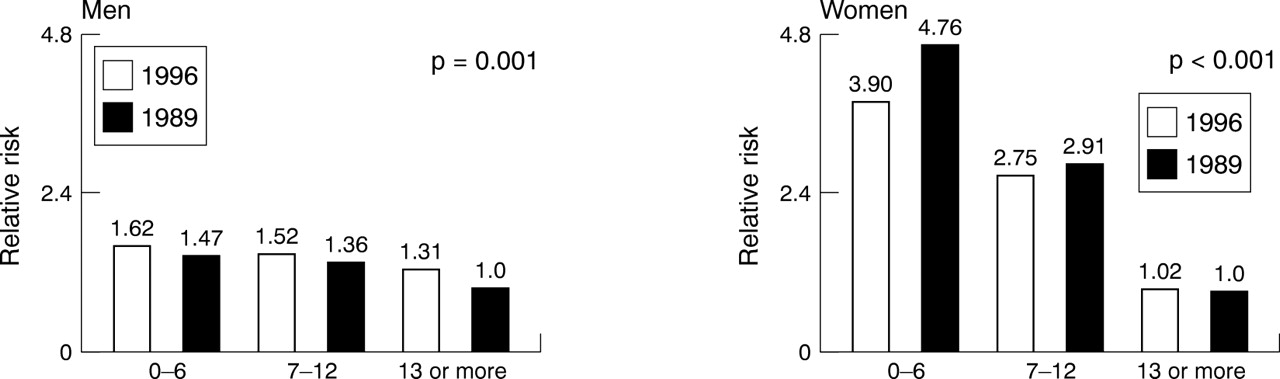
Additional analyses showed that the probability of having CVD risk factor clustering increased across all of the educational strata among men, with the best educated men having the greatest increases (31%) in 1996 compared with their counterparts in 1989. In contrast, the probability of having the risk factor clustering decreased in women with less than high school studies and was almost unchanged in those with at least college level studies in 1996 (fig 1). However, educational differences in the risk factor clustering still remained in both sexes in 1996. Defining hypertension as systolic blood pressure ⩾ 140 and/or diastolic blood pressure ⩾ 90 and/or self reported history of hypertension diagnosed by physicians did not change the pattern of the results on hypertension or CVD risk factor clustering.
{kind=link}
Relative risks of people who had more than two of the three CVD risk factors (hypertension, cigarette smoking and overweightedness or obesity) by sex and years of education in Tinajin, China, 1989 and 1996. The relative risks have been adjusted for age. The reference group is the best educated people in 1989 (relative risk = 1.0).
Discussion
Our results indicated an inverse association between educational attainment and CVD risk factors in the study population, which was more consistent for women than for men. These findings are in agreement with conclusions drawn from the studies carried out in developed countries.1-4 Similar findings have also been reported for some developing countries12-15 though not in others.16-19
Over the seven year study period, we found no major downward trends in the CVD risk factors with the exception of increased participation rate in leisure time physical activity. However, we found that the number of cigarettes smoked daily and the prevalence of smoking increased significantly in men. The best educated men experienced the worst unfavourable changes in the prevalence of smoking and in risk factor clustering. In contrast, it seems that no upward tendencies in any of the risk factors were observed in women. Mean body mass index decreased significantly during the study period. However, blood pressure increased among the best educated women.
To our knowledge, this is the first study reporting trends in CVD risk factors with regard to socioeconomic status for developing countries. In industrialised societies, the major CVD risk factors are declining steadily across the entire socioeconomic spectrum in both sexes, although socioeconomic inequalities still exist.7-9Divergent trends were displayed for smoking, with the prevalence of smoking decreasing drastically in higher socioeconomic groups and declining slowly or levelling off in lower socioeconomic groups.7-9 Our findings on the trends in the prevalence of smoking with respect to education level in men seem to be opposite to those observed in developed countries.
The reason that diastolic blood pressure increased irrespective of the education level in both sexes remains unknown. Blood pressure is positively associated with salt intake and body mass index and to a lesser extent, it is inversely associated with cigarette smoking. Our data showed that body mass index levelled off in men and decreased in women. Cigarette smoking increased in men and decreased in women. There is some evidence24 that there were no major changes in salt intake in the study population during this study period. It seems likely that the evidence presented here cannot account for the overall increases in diastolic blood pressure in the study population.
The deterioration of the risk factors seemed to concentrate in the best educated people in this population over the study period. In developed countries,7-9 major CVD risk factors are declining across all educational strata. Highly educated people experience an earlier onset or display a faster decline in CVD risk factors compared with less educated people. There are no upward trends in the risk factors found in highly educated people. Winkleby et al 2 pointed out that education might, in some way, influence risk for disease rather than vice versa—that is, risk factors could influence the extent of education. Higher levels of education may positively affect health by allowing the person to gather the necessary skills and assets required to insulate them from adverse factors or to reduce exposure to negative influences on health, adopting a positive health behaviour2 3 5 and having access to preventive health services.2-4 In this study, the better educational level, however, did not seem to be able to prevent the worsening of the risk factors in those highly educated people even though the best educated people still had the lowest levels of risk factors.
In our study, there were some improvements in the risk factors found in women. However, a deterioration in some of the risk factors took place in men. It is also apparent that the best educated men tended to experience a relatively greater deterioration. Our data may indicate the need of CVD prevention with respect to socioeconomic disparities and gender differences in developing countries.
CVD has been described as a marker of modernisation and social affluence17 25 and can mirror a society's stage of economic development.26 From the mid-1980s to the mid-1990s, the Chinese economy experienced strong growth, with an average annual 8.3% increase in gross national product per capita.27 During this period, CVD became the leading cause of death, especially in urban areas. A prospective study25suggested that the direction of the association between SES and CVD is not immutable. Social and environmental forces at play in the societies in which you live may be a major component of the impetus for the transition. On the basis of our analyses, it can be proposed that the contribution of educational attainment to the CVD risk factors in the study population may possibly be affected by the interaction of education with social and environmental factors. The influence of education and the synergism of education with social and environmental factors through which a person's health is affected may differ between men and women.
Given the deterioration of CVD risk factors that mainly occurred in the best educated people in this Chinese population, our data do not seem to wholly support the proposal5 that increases in a person's educational status inevitably lead to improvements in their health.
References
Footnotes
-
Funding: this study was supported jointly by grants from the Graduate School of Public Health, University of Kuopio, and the Academy of Finland.
-
Conflicts of interest: none.