Article Text

Abstract
Background Motor Unit Number Index (MUNIX) is a novel neurophysiological measure that provides an index of the number of functional lower motor neurons in a given muscle. So far its performance across centres in patients with amyotrophic lateral sclerosis (ALS) has not been investigated.
Objective To perform longitudinal MUNIX recordings in a set of muscles in a multicentre setting in order to evaluate its value as a marker of disease progression.
Methods Three centres applied MUNIX in 51 ALS patients over 15 months. Six different muscles (abductor pollicis brevis, abductor digiti minimi, biceps brachii, tibialis anterior, extensor dig. brevis, abductor hallucis) were measured every 3 months on the less affected side. The decline between MUNIX and ALSFRS-R was compared.
Results 31 participants reached month 12. For all participants, ALSFRS-R declined at a rate of 2.3%/month. Using the total score of all muscles, MUNIX declined significantly faster by 3.2%/month (p≤0.02). MUNIX in individual muscles declined between 2.4% and 4.2%, which differed from ASLFRS-R decline starting from month 3 (p≤0.05 to 0.002). Subgroups with bulbar, lower and upper limb onset showed different decline rates of ALSFRS-R between 1.9% and 2.8%/month, while MUNIX total scores showed similar decline rates over all subgroups. Mean intraclass correlation coefficient for MUNIX intra-rater reliability was 0.89 and for inter-rater reliability 0.80.
Conclusion MUNIX is a reliable electrophysiological biomarker to track lower motor neuron loss in ALS.
Statistics from Altmetric.com
Introduction
Motor Unit Number Index (MUNIX) is a novel quantitative electrophysiological technique which provides an index of the number of functional lower motor neurons (LMNs) in a muscle. Recent studies have demonstrated good test-retest reliability in healthy participants and patients with amyotrophic lateral sclerosis (ALS).1–5 It has been suggested that this technique may serve as a marker in diseases with progressive loss of motor units (MUs), such as ALS.1–6
MUNIX applies a statistical method, using the area and power of the compound muscle action potential (CMAP) after supramaximal electrical stimulation, and area and power of the surface electromyography (EMG) at different levels of voluntary isometric activation (figure 1). These values are used to compute the ‘ideal case motor unit count’ to estimate the amount of functioning motor neurons. In comparison to other MUNE (MU number estimation) techniques, MUNIX does not identify individual MU potentials, which makes this method very fast to perform in usually less than 5 min per muscle. MUNIX first calculates the number of MUs and then the average size of MUs. By contrast, most MUNE methods first determine the average size of MUs to calculate the MU number. MUNIX is not only a very fast technique, it is also non-invasive and can be applied to any distal or proximal muscle in which a CMAP can be elicited by supramaximal electrical nerve stimulation. The method has been described in detail.3 ,7

(A–C) Motor Unit Number Index (MUNIX) calculation in the abductor pollicis brevis muscle of a healthy participant. The compound muscle action potential (CMAP) is recorded using standard nerve conduction technique. The position of the active electrode is manipulated to record the CMAP with highest amplitude (A). The surface electromyography interference pattern (SIP) is recorded when the patient maintains a constant isometric force of contraction at different force levels. Five different force levels from slight to maximum are recorded twice (B), resulting in 10 SIP epochs. For each SIP epoch, the area under its rectified waveform and its power are measured. This is used in conjunction with the CMAP to compute the so-called ‘ideal case motor unit count (ICMUC)’. A plot of ICMUC versus SIP area is made, and the relationship of data points is modelled as a power regression equation (C). Using the parameters of regression, MUNIX is calculated as the ICMUC value when SIP area is 20 mVms.
Three previous multicentre MUNE studies in patients with ALS have examined only a single muscle, usually the musculus abductor digiti minimi (ADM) or musculus abductor pollicis brevis (APB).8–10 Although these studies have revealed a significant MUNE decline over time, comparison with the ALS Functional Rating Scale-Revised (ALSFRS-R) was only determined in one study utilising historical ALSFRS-R data. Furthermore, partial or complete denervation in these frequent clinically early affected and wasted muscles may limit their value as a suitable surrogate marker in more advanced stages of the disease. Moreover, it is unknown whether MUNE methods are equally sensitive to quantify LMN loss in bulbar-onset ALS as compared with limb-onset ALS.
As ALS usually begins focally in the limbs, bulbar or rarely in the thoracic region, and then spreads to contiguous neighbouring regions, measurements from several upper and lower limb muscles should provide more accurate information on the pattern of disease progression than those from single muscle measurements.11
The main aim of this multicentre study was to longitudinally track the loss of LMNs in ALS participants using a battery of distal and proximal limb muscles, and to compare these findings with a standardised functional outcome measurement (ALSFRS-R).
In addition, we sought to determine intra-rater and inter-rater reliability of MUNIX measurements for experienced examiners with this method.3 ,5 ,6
Participants and methods
Patients with ALS were recruited in three centres: Lisbon, Milwaukee, Wisconsin and St.Gallen. The protocol was approved by the local ethics committees. Written informed consent was obtained from all participants.
Patients with ALS had to fulfil the categories for possible, probable-laboratory supported, probable or definite ALS according to the revised El Escorial criteria.12 Diagnosis was performed by experienced ALS experts. Patients were excluded if they had other diseases that could influence cooperation or results (eg, polyneuropathy, focal nerve entrapment, etc). Symptom onset, defined as weakness, dysarthria, dysphagia, dyspnoea, gait impairment or disturbance of fine finger movements, had to be shorter than 24-month duration. The latter criterion was added to avoid bias in the study towards slow progressing patients, or patients with advanced stage and already numerous wasted muscles at study entry. Assessments were performed every 3 months±1 week.
Based on the data of a pilot study, power analysis indicated the need for a minimum of 30 recruited patients to allow reliable statistical analysis for test-retest reliability, with a relative error below 5%.5
To exclude variability due to electrode size and material,13 each centre used the same self-adhesive disposal surface ground and two disc recording electrodes with 15 mm diameter (Ref 019-415200, CareFusion, Middleton, Wisconsin, USA). Measurements were performed using commercial Keypoint-Classic-electromyographs, Keypoint.net-electromyographs and Synergy-electromyographs.
The protocol for MUNIX measurements, model and computation has been reported previously.3 ,5–7
MUNIX was performed in the APB, ADM, biceps brachii (BB), tibialis anterior (TA), extensor digitorum brevis (EDB) and abductor hallucis (AH) muscles after supramaximal distal stimulation of the corresponding nerves. It was mandatory to adjust the position of the recording electrode several times to achieve a maximal CMAP amplitude with minimum rise time and sharp negative take-off. Measurements were performed on the same side of the body throughout the study. The clinically stronger side was selected in order to avoid measurements in wasted muscles. Measurements in such muscles bears the risk of an early ‘floor effect’, since changes of the motor neuron pool will not be detectable. If both sides were symmetric in strength, the right side was the default choice.
At each visit, the ALSFRS-R score was assessed by the same ALS nurse or caring neurologist. ALSFRS-R raters and MUNIX raters were blinded to each other's results.
Test-retest examinations at the first visit and after 12 months were an optional part of the protocol. In one centre, two investigators performed retest MUNIX studies in 15 participants three times at the first visit and after 12 months. The order was rater A and then rater B; rater A gave a break longer than 15 min in between. In 20 participants, intra-rater reliability was investigated in two centres. Electrodes and marks were completely removed between each session. Raters were blinded to each other's results.
Statistics
To compare the MUNIX of various muscles as well as ALSFRS-R score during the time course of 15 months, percentage change from baseline was calculated for each parameter. Linear mixed-effect models with the dependent variable ‘percent change from baseline’; fixed factors ‘time (month), muscles, ALSFRS-R’; and a random factor variable were performed. To calculate the relative decline per month, month (in numeric values) was nested in the muscles as a fixed factor. To compare the relative decline for each muscle versus ALSFRS-R at each point in time, the fixed factor muscle was nested in the factor month. Results are presented as difference of means with the corresponding 95% CI and p value. A p value<0.05 was considered significant. For an appropriate comparison of the time series data, the SE was applied. All analyses were performed using the statistical programme R V.2.15.2.14
The two-way random, single measure intra-class correlation coefficient (ICC) was calculated for statistical analysis of the total variability (intra-rater and inter-rater variability). The variability of the mixed-effect model was verified routinely by inspecting the distribution of the residuals using quantile plots. No systematic deviation from normality was detected.
Intravariability and intervariability were estimated from mixed-effect models with subject as random effect without fixed effects. ICC is the percentage of the intersubject variability compared to the total variability. High ICC values near 1.0 indicate that the raters had performed their measurements similarly.
Results
MUNIX was well tolerated in all participants. One participant declined longitudinal measurement of the BB due to discomfort. No major technical issues occurred. Obtaining an isolated, non-contaminated BB CMAP (ie, free of volume conducted non-BB muscle coactivity) at times proved to be challenging. Measurements of the complete set of all six muscles required 20–40 min recording time.
Total cohort
A total of 51 patients were participated in this study. Each centre recruited between 15 and 18 patients with ALS. One centre recruited three patients who did not match inclusion criteria and were excluded from analysis (disease duration 27–58 months), resulting in a total of 48 patients (37 male, 11 female). Mean age of patients was 58.9 years±11.7 (SD). Mean disease duration at the time of first measurement was 14.1 months±6.0. Mean ALSFRS-R at first measurement was 40.1±5.1. Seventeen patients had bulbar disease onset (35.4%) and 31 spinal onset (64.6%). In the spinal group, 16 (33.3%) patients had upper limb and 15 (31.2%) patients had lower limb onset.
Of 48 participants, 31 reached the follow-up visit at month 12, and 25 patients reached at month 15.
ALSFRS-R declined from baseline—defined as 100%—to 72.1%±3.6 (SE) at month 12. The mean monthly relative decline was −2.3% per month or 0.92 ALSFRS-R points/month (table 1, figure 2 and see online supplementary table S1).
Relative decline rates (% per month) of the total cohort and different onset subtypes over 15 months
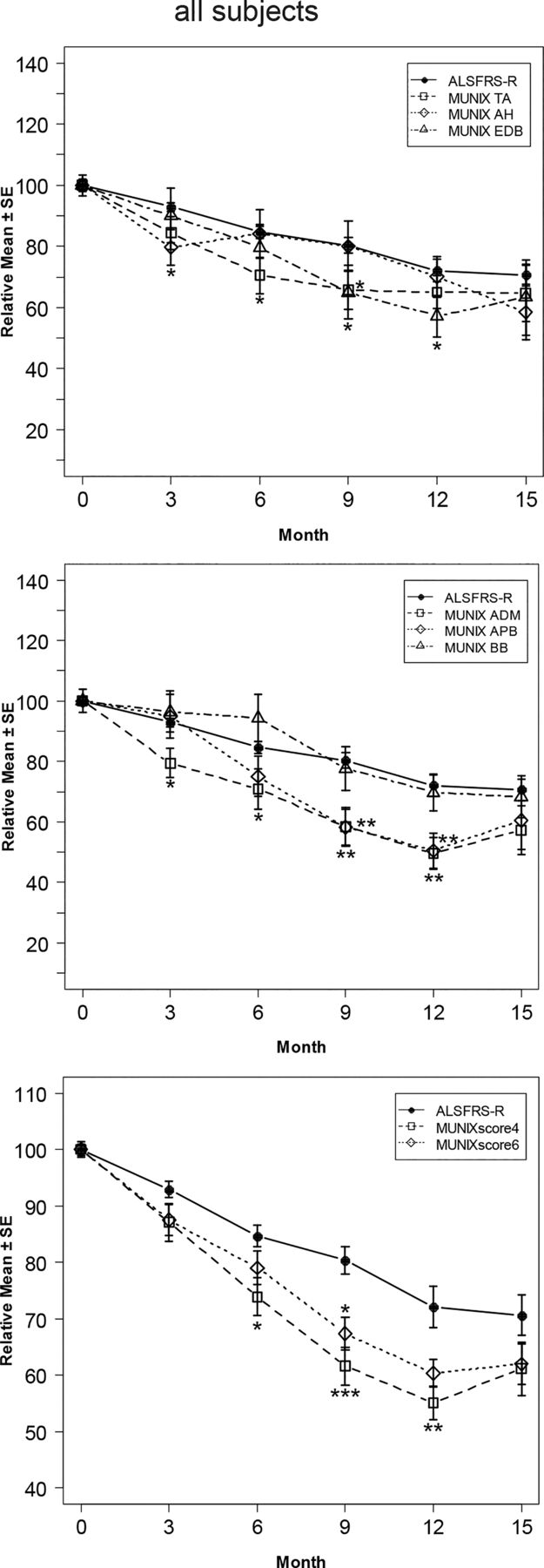
Decline of Motor Unit Number Index (MUNIX) and ALSFRS-R in the total cohort. Upper part: arm muscles, middle part: leg muscles, lower part: sum-scores. Significance levels for the comparison of ALSFRS-R versus MUNIX: *p≤0.05, **p≤0.01, ***p≤0.001. Monthly decline rates were most prominent for the abductor pollicis brevis (−4.2%) and abductor digiti minimi (−3.8%). The lowest decline showed the biceps brachii (−2.4%) and abductor hallucis (−2.6%), which were similar to the decline of the ALSFRS-R (−2.3%). MUNIXscore4 declined −3.7%, which was highly significant from month 6 to month 12 compared to ALSFRS-R (p≤0.03 to 0.0005).
The most prominent drop was visible in the ADM (49.6%±5.3) and APB (50.5%±5.8), followed by the EDB (57.2%±6.8) (figure 2 and see online supplementary table S1). Monthly decline rates ranged from −2.4% to −4.2% per month.
The mean of all MUNIX values—MUNIXscore6—declined to 60.3%±2.5 at month 12, at a rate of −3.2% per month. The decrease was significantly higher than the decline of ALSFRS-R at month 9 (p≤0.02) (figure 2 and see online supplementary table S1).
Excluding the two muscles with the lowest decline and prominent variability (AH and BB)—denoted MUNIXscore4—revealed a decline to 55.1%±2.9 at month 12 with an average decline rate of −3.7% per month. The difference of MUNIXscore4 compared to ALSFRS-R was highly significant from month 6 to month 12 (p≤0.03 to 0.0005).
Onset subgroups
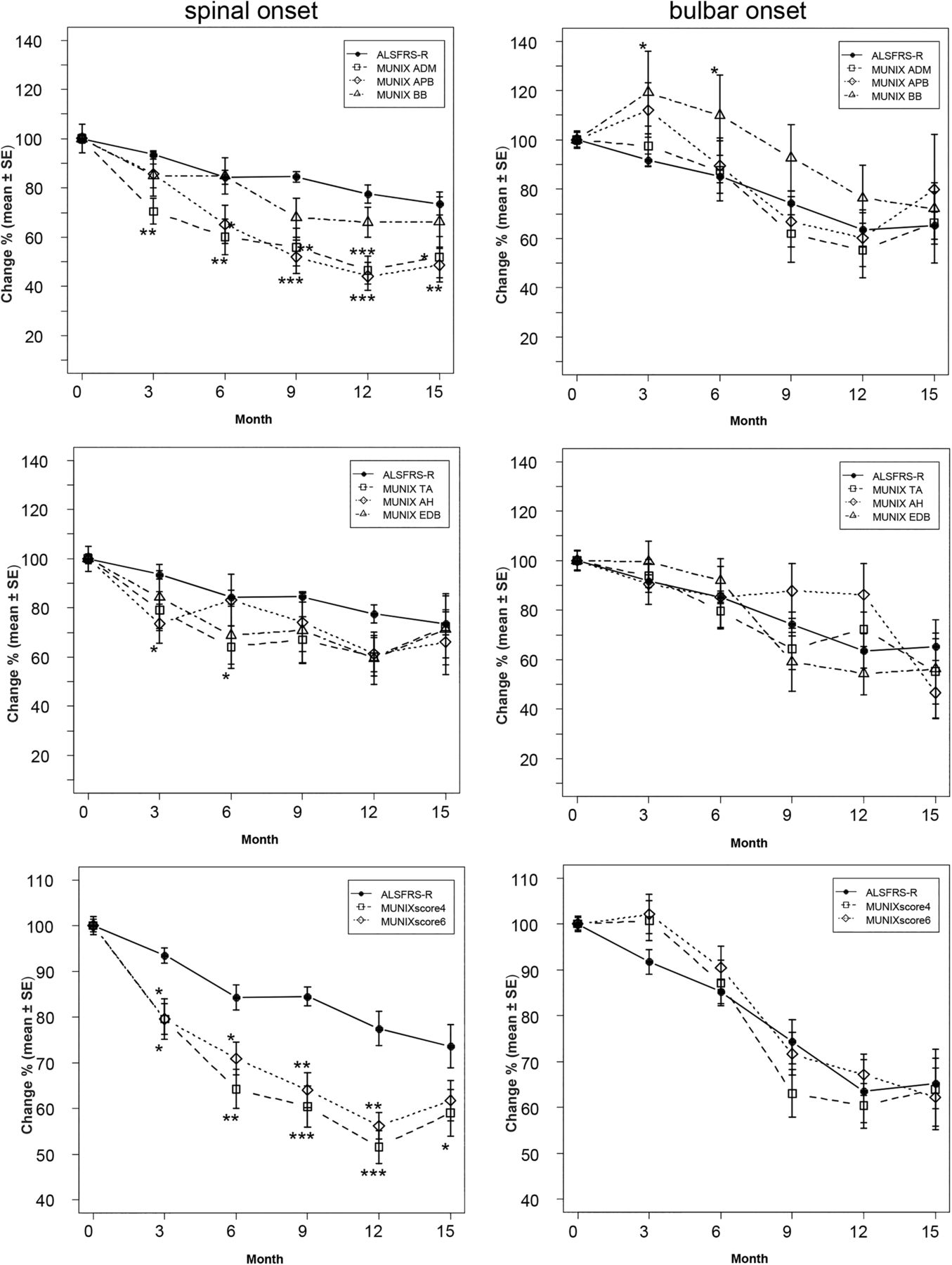
In the spinal onset and bulbar onset subgroups, the muscles changed in different patterns. In bulbar patients (n=17), the decline of individual muscles MUNIXscore6 and MUNIXscore4 was not different from ALSFRS-R decline. In spinal onset patients (n=31), the APB, ADM, MUNIXscore6 and MUNIXscore4 showed a consistently significant greater decline starting at month 3 (p≤0.05 to 0.0005). (figure 3A+B, see online supplementary tables S2 and S3) This was most prominent in the upper limb onset group (n=16) (figure 4A and see online supplementary table S4).
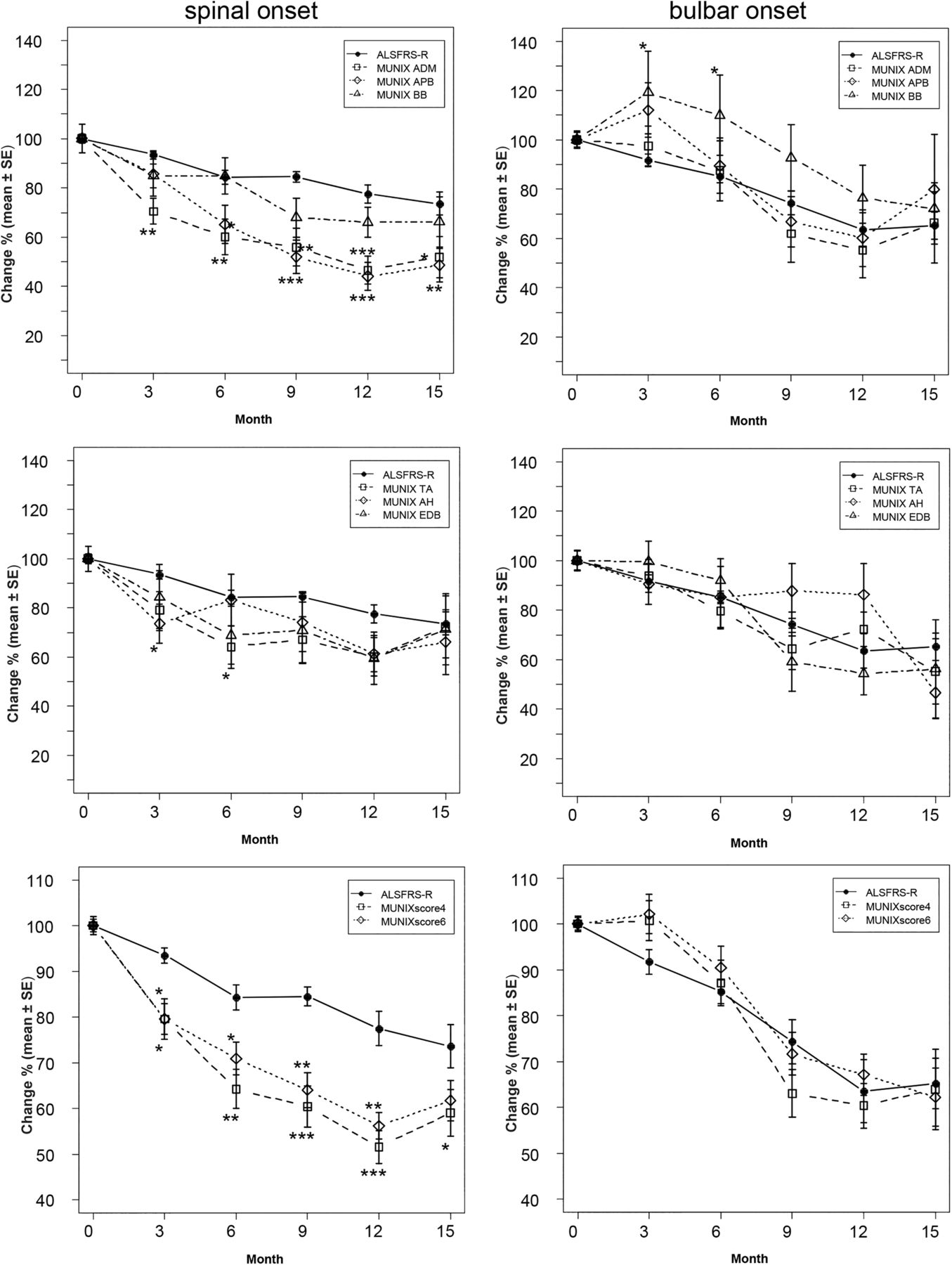
(A) Decline of Motor Unit Number Index (MUNIX) and ALSFRS-R in the spinal onset group. Significance levels as in figure 2. The abductor pollicis brevis (APB) had the greatest monthly decline rate (−4.7%), followed by the abductor digiti minimi (ADM) (−3.9%). APB, ADM, MUNIXscore6 and MUNIXscore4 showed a consistently significant greater decline starting at month 3. (B) Decline of MUNIX and ALSFRS-R in the bulbar onset group. The decline of individual muscles, MUNIXscore6 and MUNIXscore4 was not different from ALSFRS-R decline. The biceps revealed a significant lower decline from month 3 to 6 (*p≤0.05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
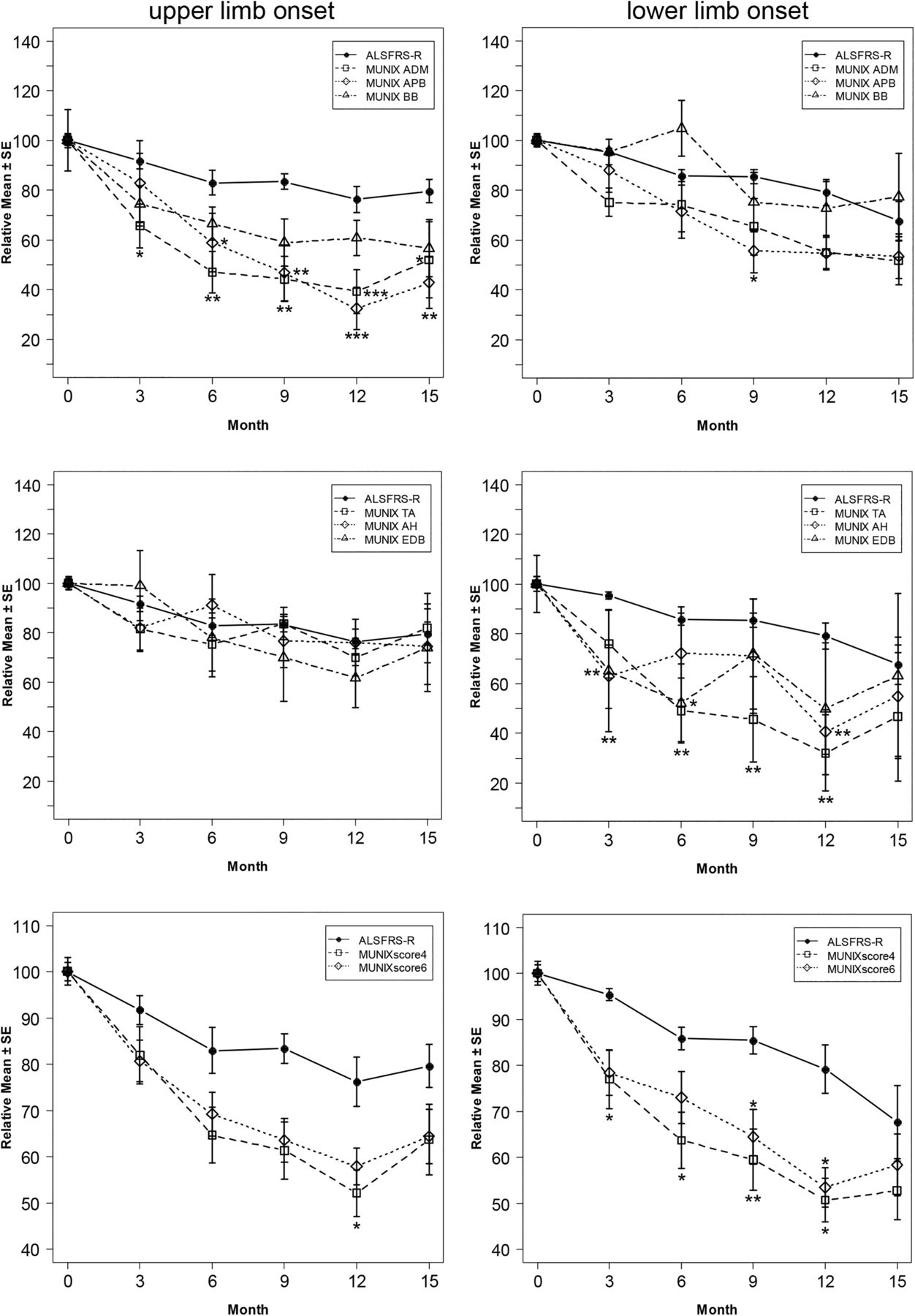
(A) In upper limb onset (n=16) the abductor pollicis brevis had the greatest monthly decline rate (−5.4%), followed by the abductor digiti minimi (−4.5%) and deviated significantly from ALSFRS-R (p≤0.04 to 0.0004) starting at month 3. Significance levels as in figure 2. (B) In lower limb onset, the tibialis anterior (TA) showed the greatest decline rate of −5.9% per month. Motor Unit Number Index (MUNIX) of TA, extensor digitorum brevis, abductor hallucis and MUNIXscore4 and −6 deviated significantly from ALSFRS-R (p≤0.03 to 0.002). Significance levels as in figure 2.
In the upper limb onset (n=16), APB and ADM deviated significantly from ALSFRS-R (p≤0.04 to 0.0004) starting at month 3. In the lower limb onset group (n=15), MUNIX of EDB, AH, MUNIXscore4 and MUNIXscore6 and most prominently for the TA deviated significantly from ALSFRS-R (p≤0.03 to 0.002) (figure 4A, B and see online supplementary tables S4 and S5).
CMAP amplitudes declined at similar, but slower rates compared to MUNIX (see online supplementary figures S1–S3). Values of MUNIXscore6 and MUNIXscore4 were significantly lower compared to CMAP amplitudes after 1 year (p=0.005 and 0.001, respectively).
Slow versus fast progressing participants, total cohort
Stratifying patients into two equal groups based on slower and faster ALSFRS-R decline rates revealed −1.3% per month for the slow group versus −3.8% per month for the faster group. The corresponding decline rates of MUNIXscore6 were −2.2% per month and −5.1% per month, and for MUNIXscore4 −2.5% per month and −5.7% per month, respectively. In the slower group, MUNIXscore4 decline was significantly higher compared to ALSFRS-R at month 9 (p=0.016) and at month 12 (p=0.004).
In the fast group, MUNIXscore4 was significantly lower at month 9 (p=0.008). MUNIXscore6 and MUNIXscore4 slopes between both groups were significantly different from month 3 to month 15 (p≤0.04 to 0.00 000).
Stratifying into two equal groups (n=24) based on slower (−2.1% per month) and faster (−5.0% per month) decline of MUNIXscore6 revealed ALSFRS-R decline rates of −1.7% per month and −2.9% per month. ALSFRS-R slopes between both groups were significantly different from month 6 to month 15 (p≤0.008 to 0.00 001). Similar results were obtained when stratifying using MUNIXscore4. The slow MUNIXscore4 group (−2.6% per month) showed a slower ALSFRS-R decline of −1.9%, while the faster MUNIXscore4 group (−5.7% per month) demonstrated a corresponding faster ALSFRS-R decline of −2.8% per month.
To detect a given difference of monthly decline for MUNIXscore4 between two groups (eg, verum vs placebo), sample size calculations were performed using one-sided power calculations of mixed-effects models.15 With a total of 100 patients (50 per group), a δ of 45% relative to the decline rate of MUNIXscore4 can be detected on a significance level of 5% with 80% power. Consequently, a reduction of 25% relative to the initial value of MUNIXscore4 will take 11.6 months. For the ALSFRS-R values, it will take 26.5 months to achieve the same reduction.
Test-retest reliability
Variability expressed by the means of SD was higher for MUNIX than for ALSFRS-R, which was expected due to the higher range of absolute numeric values (range: MUNIX 0–452, ALSFRS-R 10–46).
For 20 ALS patients, MUNIX and CMAP intra-rater test-retest variability was evaluated (two centres) at entry and for 15 patients, inter-rater variability was tested (one centre). All muscles demonstrated a high ICC. Intra-rater reliability for MUNIX was best for the AH with an ICC of 0.97 and lowest for the BB with 0.81 (table 2A).
(A+B) Test-retest reliability
Test-retest reliability of CMAP amplitude measurements was slightly higher for most muscles. Inter-rater variability revealed similar results except for the TA, in which ICC values were lower (MUNIX 0.46 and CMAP 0.66).
One centre tested intra-rater (n=6) and inter-rater (n=5) variability again after 12 months; mean MUNIX ICC were similar to the results at the first visit (table 2B).
Floor effect of measurements
Five patients (10.4%) had already one or more completely wasted muscle at baseline. Of 30 patients at month 9, three had developed a completely wasted APB (10%) and two a wasted ADM (6.7%). MUNIX of the ADM declined below 10% of baseline in six patients (17.6%) by month 9 and APB MUNIX in four patients (12.1%). MUNIX of all six muscles did not decline to zero in any participant until the end of follow-up.
Discussion
This is the first longitudinal multicentre study that applied the MUNIX method in multiple muscles of ALS patients, demonstrating that loss of LMNs can be tracked. An important observation is, that even when measuring the clinically less affected side, the decline of MUNIX was significantly steeper in several muscles than the functional decline as reflected by ALSFRS-R, which is in concert with previous MUNE findings in asymptomatic muscles of SOD1-mutation carriers.16 This was also the case when using the mean MUNIX values of all muscles—denoted MUNIXscore6—and even more remarkable for MUNIXscore4, when excluding the AH and BB muscles from analysis. Reasons for this exclusion were that stimulation of the musculocutaneus nerve is technically challenging and costimulation of neighbouring nerves can result in erroneously high CMAP amplitudes. Likewise, CMAP amplitudes of the AH can be generated by coactivation of adjacent muscles, extending beyond the intended targeted muscle response.17 Furthermore, performing voluntary pure abduction of the hallucis for optimal surface EMG recordings can be difficult. It has also been shown that MUNIX values are influenced by the direction of movement with multifunctional muscles, making the AH recording procedure prone to error.18 ,19
The ‘sum-scores’ (MUNIXscore6 and MUNIXscore4), which may be viewed as an ‘electrophysiological body-scan’ over two regions, showed nearly identical average decline rates in all different subgroups (bulbar, spinal, lower and upper limb onset) over 15 months (MUNIXscore4: −3.6% to −3.8% per month). By contrast, the ALSFRS-R was different in bulbar and spinal onset patients (−1.9% to −2.8% per month) (table 1). Therefore, the average decline rates of MUNIX sum-scores over 15 months seem to be independent from the region of onset. It can also be concluded that MUNIX is capable of detecting progressive spinal LMN loss in bulbar onset patients.
Bulbar onset patients comprised 35% of our population, and the average clinical deterioration of the ALSFRS-R at a rate of 0.92 points per month is in concert with the reported average functional decline in ALS patients.20 ,21 Therefore, our study population seems to be representative.
It should be emphasised that the ALSFRS-R represents a ‘functional sum-score’, combining different body regions and includes not only assessment of LMN loss, but also upper motor neuron impairment. MUNIX reflects LMN loss and is most likely independent from external factors which impact on the ALSFRS-R (eg, non-invasive ventilation, percutaneous gastric feeding tube, medical interventions for sialorrhoea, etc). This suggests the use of MUNIX as a complementary objective biomarker to measure disease progression, especially in phase II exploratory trials. The time to detect 25% relative difference of decline with 80% power between two groups (each n=50) would take 11.6 months for MUNIXscore4, but 26.5 months for ALSFRS-R.
However, the relative and absolute variability of MUNIX was higher than variability of ALSFRS-R. This is due to the technique itself (ie, the high range of MUNIX values) and is also an issue for MUNE methods.10 ,22 In our study, the impact of variability can be diminished when using a nested statistical model. Therefore, high variability and SD does not necessarily mean that a method is less suitable than others with lower variability, as more prominent changes over time are also likely to produce a more prominent variability.
Another advantage of MUNIX is that rapidity in recording time allows measurement of multiple muscles in two regions, even if one or more muscles are completely wasted. Recording from a single muscle bears a higher risk of a floor effect. This has not been considered in previous studies.8–10 In our cohort, approximately 10% of patients had already one or more completely wasted muscle at the first measurement. After 9 months, in 17.6% of patients MUNIX ADM dropped below 10% from baseline and in 12.1%, in the MUNIX APB. In these participants, further LMN loss will not be detectable by any MUNE method in such muscles.
This study did not aim to test MUNIX as a prognostic factor. Further data from controlled ALS trials is needed to approach this issue. However, stratifying our data into two groups based on fast and slow change of ALSFRS-R revealed significantly faster and slower MUNIX decline rates already at month 3. This indicates that MUNIX can accurately discriminate between faster or slower disease progression.
The results of the subgroup analysis were limited by the relatively small number of participants, as this study was not powered for such detailed analysis. Nevertheless, change of MUNIX followed the reported pattern of spread of disease. MUNIX changed differently in different muscles and different onset types. LMN loss was very prominent for the clinically less affected (contralateral to onset) arm muscles in the upper limb onset and for the (contralateral to onset) leg muscles in the lower limb onset. This is consistent with a spread of disease from the site of onset to the contralateral side as well as to the ipsilateral neighbouring regions.11
In bulbar onset patients, MUNIX data suggest an initially relative stable number of MU in the limbs over a 3–6-month period, followed by a spread of disease with a more or less simultaneous decline in both regions (figure 3B and see online supplementary table S3).
The most prominent changes were seen in the small hand muscles (APB, ADM), TA, and EDB, while the BB was relatively preserved. This reflects the observed clinical pattern of early wasting of the small hand muscles.23 The APB had (with the exception of the bulbar onset subgroup) faster decline rates and deterioration than the ADM, and may be the MUNIX analogue of the ‘split-hand’ phenomenon. However, this difference was not statistically significant.24–26 The recently suggested electrophysiological ‘split-hand-index’, which uses the CMAP amplitude for calculation, might also be adapted for MUNIX measurements.24 ,25 ,27 ,28 This index additionally uses the first interosseus dorsalis muscle (FDI).27 ,28 MUNIX measurements from the FDI have already been performed.18 It is likely that MUNIX should be capable to detect the split-hand pattern earlier than using the CMAP, because in our results the decline of MUNIX exceeded the decline of the CMAP amplitudes.
After 15 months, mean MUNIX in several muscles tended to be higher than at month 12, which is most probably related to a drop-out bias of patients with faster disease progression rate. This is mirrored by a flattening decline of the ALSFRS-R score between month 12 and 15 (figure 2).
An essential attribute of every measure of disease progression is its reliability within (intra-rater) and in-between (inter-rater) examiners. In previous studies, a ‘moderately high’ to ‘high reliability’ could be demonstrated for MUNIX by different workgroups in healthy volunteers and patients with ALS.1 ,4 ,5 Other groups have compared MUNIX with other more complex MUNE methods like the high-density MUNE (HD-MUNE) and the incremental stimulation MUNE (IS-MUNE), and found a similar or better reproducibility for MUNIX, yet a comparable rate of LMN loss.2 ,29 Our results demonstrate a very good reliability of MUNIX measurements in multiple muscles in patients with ALS at first evaluation as well as further on in the course of the disease.
In conclusion, longitudinal MUNIX measurements in patients with ALS in a multicentre setting are very feasible and suggest that MUNIX can be employed as a biomarker in multicentre ALS trials.
Acknowledgments
The authors would like to thank all participating patients and their caregivers. The authors are thankful to Urs Simmen (DTC, Basel, Switzerland) for performing the statistical analysis. Dr Nandedkar thanks CareFusion for support. Dr Barkhaus acknowledges funding support from the Dolores and Carroll Fund from the Milwaukee Medical Foundation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
- Data supplement 2 - Online tables
Footnotes
Funding This work was supported by the Swiss ALS Foundation, the Swiss NeRAB Foundation and the EU Joint Programme—Neurodegenerative Disease Research (JPND) project (grant number SNF 31ND30_141622).
Competing interests CN and MW have received honoraria from Hänseler AG, Switzerland, as advisory board members. MW has received advisory board honoraria from Biogen Idec and Merz Pharma, Switzerland.
Patient consent Obtained.
Ethics approval Ethic Committee St. Gallen, Wisconsin and Lisbon.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary