Article Text

Abstract
Background and purpose Psychosurgery, such as anterior capsulotomy, is a therapeutic option for treatment-resistant obsessive-compulsive disorder (OCD). In this paper, we present a prospective, long-term follow-up study aimed at evaluating both the efficacy and the safety of anterior capsulotomy for the treatment of severe, refractory OCD.
Methods Twenty-four patients were surgically treated in our centre between 1997 and 2009, 19 of whom were included in this study. Patients were assessed at 3, 6, 12, and 24 months and last follow-up (mean of 7 years) was carried out by phone. OCD symptom severity was evaluated using the Yale-Brown Obsessive Compulsive Scale (Y-BOCS). A patient with an improvement rate of over 35% in the Y-BOCS score was considered a responder, while a patient with a 25% improvement was considered a partial responder.
Results With a mean improvement of 31% in the Y-BOCS score at long-term follow-up, 36.8% of the patients responded fully to the procedure and 10.5% were considered partial responders, for an overall response rate of 47.3% of patients. At the end of the study, 3/19 patients had recovered (Y-BOCS score <8) and 3/19 were in remission (Y-BOCS score <16). No cases of mortality were reported and the overall adverse event rate was 57.9%. Only 2 patients had permanent surgical complications.
Conclusions Anterior capsulotomy is an effective and safe technique for the treatment of severe refractory OCD in patients who have no other alternative to improve their symptoms.
- NEUROPSYCHIATRY
- NEUROSURGERY
Statistics from Altmetric.com
Introduction
Obsessive-compulsive disorder (OCD) is a chronic and debilitating disease defined by recurrent, persistent and intrusive thoughts, images or impulses (obsessions), causing significant distress and anxiety. Acts or behaviours that reduce or prevent the discomfort caused by these obsessions often arise (compulsions). Classification based on the nature of the obsessions and/or compulsions experienced has been defined by Rück and colleagues,1 dividing OCD into four subtypes: (a) forbidden thoughts, (b) contamination/cleaning, (c) order/symmetry and (d) hoarding. Considering that OCD is the 10th most common cause of disability, affecting 1 adult in 100 in the USA, this disease has a significant socioeconomic burden due to the costs entailed by the chronic nature of the illness and the impact on work, leisure activities and interaction with family and the social environment.2 Importantly, OCD is not only associated with suffering for the patients and a reduced quality of life but also with significant mortality3; recent studies suggest that 10%–27% of patients might attempt suicide during their lifetime.
The standard first-line medical treatment usually consists of antidepressant medication such as selective serotonin reuptake inhibitors (SRIs) or tricyclic antidepressants often supplemented by cognitive behavioural therapy (exposure to feared stimuli and prevention of a subsequent response). Despite this therapeutic approach, symptoms do not improve in about 20%–30% of patients with OCD.4 Patients with OCD are considered refractory following a lack of improvement after: (a) a trial of at least three different SRIs taken at optimum dosage for a minimum of 12 weeks, (b) the use of at least two atypical antipsychotics and (c) psychotherapeutic augmentation strategies (30 h or more).5 For such patients, psychosurgery procedures are the last therapeutic alternative.
Psychosurgery has been practiced for decades for a variety of debilitating psychiatric conditions, including schizophrenia, bipolar disorder and OCD. However, its use has been extremely controversial and relatively few patients with OCD have been treated with such procedures. Moniz was the first to describe psychosurgery in 1935,6 while Talairach and colleagues published the first report on capsulotomy in 19497 for patients with anxiety neurosis. The specific target for neurosurgical treatment of OCD relies on data from electrophysiological and functional neuroimaging studies, which have found hyperactivity of the orbitofrontal, anterior cingulated cortex and caudate nucleus in patients with OCD.8 To date, four major targets are used along the cortico-striato-thalamic circuit for the treatment of OCD: anterior capsulotomy targets the anterior limb of the internal capsule (ALIC), cingulotomy targets the anterior cingulated cortex as well as the fibres of the cingulum, subcaudate tractotomy interrupts the frontothalamic fibres at different sites and limbic leucotomy combines the lesions of anterior cingulotomy with those of the frontothalamic projection.9 These different psychosurgical procedures are roughly comparable in efficacy, offering benefits for about 45%–65% of patients with intractable OCD,10 and all appear to be relatively safe with a low risk of long-term adverse effects.11 Note that capsulotomy and cingulotomy performed by radiofrequency thermolesions or radiosurgery are the most published procedures for OCD. Deep brain stimulation (DBS), a non-ablative, reversible and adjustable neurosurgical procedure, has recently been considered as a potential therapeutic alternative for the management of resistant OCD, presenting several advantages over lesioning. In 2009, the US Food and Drug Administration granted limited humanitarian device exemption to DBS for severe OCD, the first such approval for a psychiatric illness. While only small groups of patients have been studied to date, the results are encouraging.12 ,13
Relatively few studies have examined the benefits of surgery for OCD, with most including few patients, and no randomised control trials have been conducted as yet. To prevent 21st-century psychosurgery from suffering the same fate as its 20th-century predecessor, careful documentation of its efficacy and complications is needed. The current study is a prospective study aimed at evaluating the efficacy of anterior capsulotomy in severe refractory patients with OCD on a long-term scale. We also carefully report peri- and postoperative adverse events associated with this procedure.
Material and methods
Patients
This study was approved by the Centre hospitalier universitaire de Québec Research Ethics Board and informed consent was obtained from each participant or from their representative for patients who were unable to consent (mental retardation).
Twenty-four patients underwent bilateral capsulotomy in our centre between 1997 and 2009, five of whom (20.8%) were lost at follow-up and were not included in this study (these patients were followed in other institutions after surgery). OCD was diagnosed by an independent psychiatric team using the DSM-IV criteria.
Inclusion criteria for the present study were: a severe case of OCD, with a Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score greater than or equal to 24; a duration of the disease of more than 5 years; and to be defined as treatment refractory, that is, non-responsive to medical treatment with SRIs (≥3 types of SRIs at optimal dosage for ≥12 weeks) and psychotherapy (≥30 h). Symptom severity, causing significant reduction in functioning, was determined by the Global Assessment of Functioning Scale (GAF) and the patient's score had to be less than 50 at study inclusion. Patients who had another psychiatric diagnosis according to the DSM-IV criteria were not excluded.
Surgical procedure
To localise the intended target, the ALIC, patients underwent MRI, angiographic and perfusion studies prior to surgery. Up until 2004, all patients underwent bilateral capsulotomy using the Mec-Inov stereotactic system (Mec-Inov. Lévis, Quebec, Canada). The stereotactic frame was placed under local anaesthesia before CT-scanning and the images obtained were co-registered with MRI and cerebral angiography to determine a trajectory avoiding any major vessel.
All surgeries after 2004 were performed using a neuronavigation system and a CRW frame (Integra, Plainsboro, New Jersey, USA) to determine the surgical target. Coordinates were determined using the Stealth Framelink neuronavigation system (Medtronic Inc., Minneapolis, Minnesota, USA). The entry point was pre-coronal and 20 mm off the midline. The trajectory was oblique at 20° in the coronal section plane and pass 5 mm posterior to the frontal horn of the ventricle, following the internal capsule angle. The target (the inferior limit of the lesion) was defined with respect to the mid-commissural point: 17 mm lateral, 30 mm anterior and horizontal to the AC-PC line.
All surgeries were performed by the same neurosurgeon (CP) and consisted of bilateral capsulotomy by mechanical lesioning using a Bertrand leucotome. The leucotome was inserted through a burr hole until it reached the target, and four lesions were made, achieving a total lesion length of 20 mm and a 5–6 mm diameter; the same procedure was carried out on the controlateral side.
MRI and CT were performed within 48 h after surgery to visualise the localisation of the lesion and also to monitor for possible complications (figure 1).

Postoperative MRI. (A) Axial T2 MR image showing the localisation of bilateral lesions in the anterior limb of the internal capsule (ALIC). (B) Coronal T2 image of the same patient.
Assessment
Evaluations were done before surgery and at 3, 6, 12 and 24 months following surgery. All included patients were contacted for a long-term follow-up (mean of 7 years, range 3–11). Patients were evaluated by raters not involved in the treatment; at long-term follow-up, evaluations were carried out over the phone. The raters were not trained for inter-rater reliability. The severity of OCD symptoms was assessed using the French version Y-BOCS,14 ,15 a reliable and valid instrument widely used in clinical trials for OCD. Y-BOCS is a clinician-rated, 10-item scale, each item rated from 0 (no symptoms) to 4 (extreme symptoms), yielding a total possible score ranging from 0 to 40. The scale includes questions about obsessions and compulsions (amount of time the patient spends on obsessions or compulsions, how much impairment and distress they experience, etc.). Accordingly, the result can be interpreted based on a total score: a score of 0–7 is subclinical; 8–15 is mild; 16–23 is moderate; 24–31 is severe; and 32–40 is extreme.16 A 35% reduction in the Y-BOCS severity score from baseline is a typical response criterion in trials, and patients with an improvement between 25% and 35% are considered partial responders. Moreover, patients who achieve a Y-BOCS score of ≤8 are rated as recovered and a score ≤16 means that patients are in remission.
The GAF17 was administered before surgery to rate the severity of impairments for the social, occupational and psychological functioning of adults on a global score ranging from 0 to 100.
Statistical analyses
Baseline data were compared between patients lost at follow-up and included patients using a Mann–Whitney test for continuous variables and χ2 tests for categorical variables. Patients responding to the treatment were also compared with non-responder patients using the same tests.
Growth curve analyses with mixed models were used to describe the evolution of the Y-BOCS score over time. To adequately model the non-linear evolution of the Y-BOCS score over the course of the assessment, piecewise-linear regression was used to allow different slopes of change over time. Thus, a node was generated at 3 months after surgery, the minimum time lapse considered for optimal outcomes in lesional psychosurgery.
Results
Patient characteristics
Twenty-one surgical procedures were performed in 19 patients (2 reoperations, 10.5%), Two patients included in this analysis underwent a second anterior capsulotomy owing to a relapse a few weeks after the first surgery (the apparent lesion was smaller than predicted). The second capsulotomy was performed after 6 and 4 weeks, respectively. Assessments of these patients were performed after the second surgery. The male to female ratio was 7 to 12, the mean age at the time of surgery was 40.8 (SD, 11.6; range 20–60) and these patients had been suffering from OCD for an average of 16.2 years (SD, 8.4; range 7–40).
Before surgery, the average Y-BOCS score was 34.9 (SD, 4.8; range 28–40), 16 out of 19 were considered extreme (Y-BOCS score over 32) and 3 were rated as severe (Y-BOCS score between 24 and 31). The mean GAF score was 37 (SD, 11; range 25–60), indicating serious to major impairment in several areas (social, occupational, etc.) (table 1).
Clinical and demographic characteristics of patients included in the study
Demographic and clinical data did not differ significantly between the patients lost at follow-up and those included in the study.
Most of the patients studied presented a subtype of OCD with a predominance of checking compulsions or obsessions about contamination. Only one patient had a hoarding symptom (table 2). Patients could have more than one subtype.
Distribution of OCD symptoms among the cohort
As shown in table 3, most patients (n=14; 73.7%) had an axis I or II disorder concomitant with their OCD, while only five patients had no other psychiatric comorbidity. Five patients were diagnosed with personality disorders and one with mental retardation. Among the patients studied, 31.6% had made a suicide attempt before surgery.
Frequency of psychiatric comorbidities
The majority of participants were on medication at the time of surgery, with most receiving a selective serotonin reuptake inhibitor.
Assessment of OCD symptoms
The observed mean improvement in the Y-BOCS score varied from 22.8% (p=0.02) at 3-month follow-up to 36.3% (p=0.001) at 1 year post-surgery, then remained relatively stable at 31% for the last follow-ups (p=0.049 and p=0.022 at 24 months and long-term follow-up, respectively; figure 2A). The pre-surgical mean Y-BOCS score of 34.9 (symptoms rated as extreme) showed a decrease to 22.9 at the 3-month control (classified as moderate) and this score remained constant (22.9–23.8) during all subsequent follow-ups (p<0.0001).
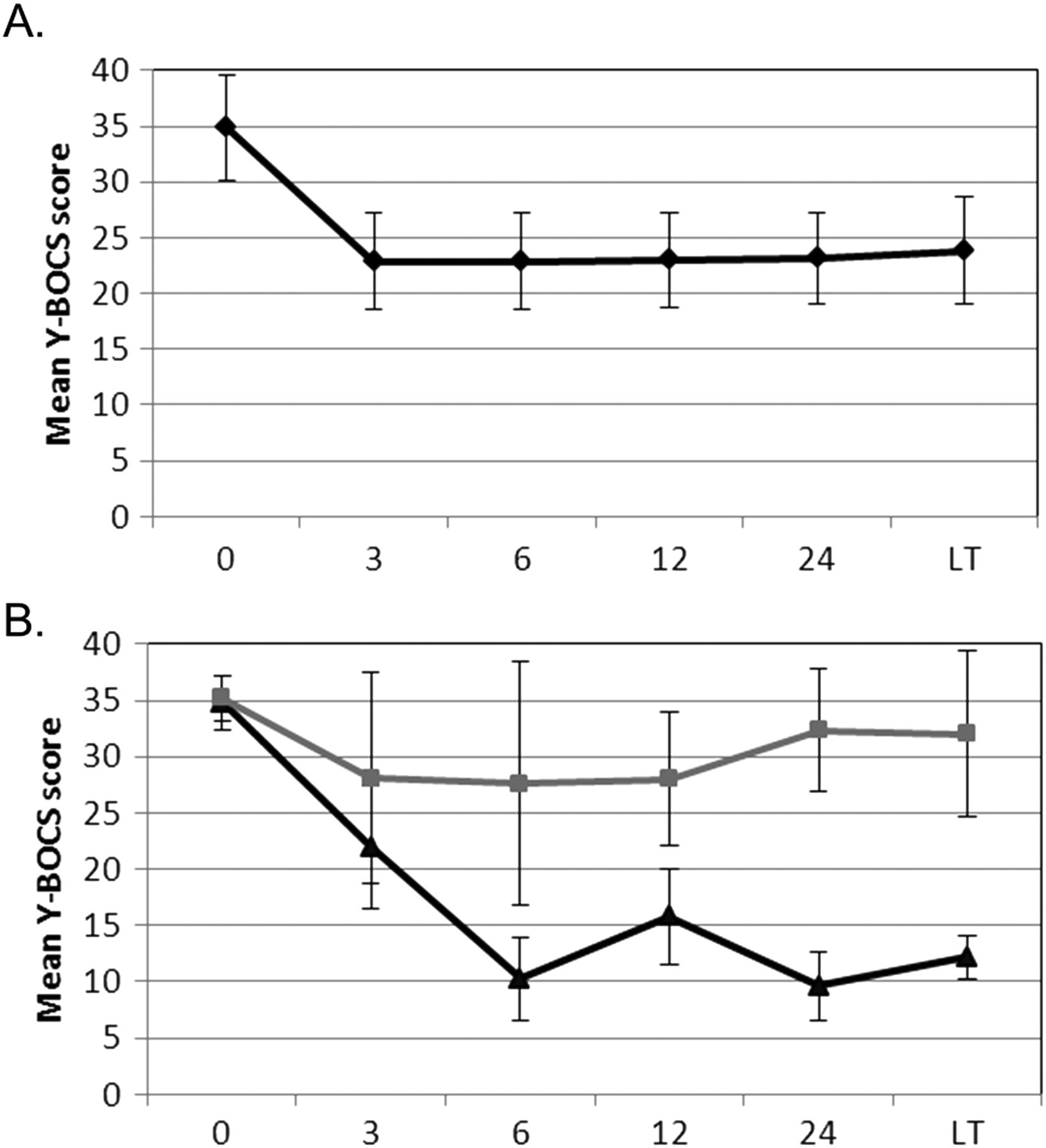
Mean Y-BOCS score of patients with obsessive-compulsive disorder over time. (A) All patients included in the study. (B) Responders (black line) compared with non-responders (grey line). LT, long-term follow-up. Y-BOCS, Yale-Brown Obsessive Compulsive Scale.
Applying the classical criteria of a 35% decrease in the Y-BOCS score for a full response, 7 out of 19 patients (36.8%) achieved a full response to the surgery at their last follow-up (two of them had no comorbidities). Considering the criteria of >25% for a partial response, 47.3% of patients were at least partial responders by the most recent follow-up (mean of 7 years after capsulotomy; figure 3).

{kind=link}
{kind=link}
{kind=link}
Response of patients with OCD following bilateral anterior capsulotomy at last follow-up (mean of 7 years). Full response: >35% improvement in Y-BOCS score; partial response: >25% to 35% improvement; non-response: <25% improvement; recovery: Y-BOCS score <8, remission: Y-BOCS score <16. OCD, obsessive-compulsive disorder; Yale-Brown Obsessive Compulsive Scale.
At long-term follow-up, three patients (15.8%) achieved a Y-BOCS score of less than 8 and were considered recovered. Three patients (15.8%) had a final Y-BOCS score of less than 16 and were classified as in remission, indicating that capsulotomy reduced their symptoms to a minimal level.
There were no significant differences between the 3-month and the long-term follow-up ratings, implying that improvement was generally stable from 3 months after surgery.
Comparing responders (>25% improvement in Y-BOCS score from baseline) to non-responders (figure 2B) showed that non-responders improved their mean Y-BOCS score by approximately 7 points during the first year but failed to maintain this initial improvement and relapsed.
In order to highlight a predictive variable for a better outcome, responder and non-responder patients were compared (table 4). Age at surgery and gender were similar between these populations. However, a longer duration of the disease seemed to predict fewer benefits from surgery (p=0.028) as responders had a mean duration of their disease of 12.4 years (SD=5.5) and this duration was 20.3 years (SD=9.4) for non-responder patients. OCD symptom severity according to the Y-BOCS score at baseline was in the same range (35.3 vs 34.6 for responders and non-responders, respectively). The presence of a psychiatric comorbidity did not influence the response to surgery.
Comparison of responders and non-responders
Complications
The patients tolerated the anterior capsulotomy well, with most presenting temporary side effects. We registered adverse events in 11 patients and most resolved during their hospital stay (table 5). The most frequent event was frontal syndrome, which was registered in five patients, with asymptomatic haemorrhage and deep vein thrombosis occurring in three patients. One patient reported urinary incontinence, while others complained of pneumonia and urinary infection. The only permanent side effects were a permanent hemiplegia due to a perioperative haemorrhage in one patient and cognitive impairment in another. Two patients underwent a second capsulotomy within the first month following the surgery because the lesion size was non-optimal as seen in postoperative MRI images, and also due to symptom recurrence.
Complications associated with anterior capsulotomy
Discussion
In the present study, we report the findings of a prospective, long-term follow-up study aimed at evaluating the efficacy and the safety of anterior capsulotomy for the treatment of severe, refractory OCD. To our knowledge, this is one of the longest follow-up studies based on OCD surgical treatment, with an average follow-up of 7 years. A single capsulotomy study has reported a longer follow-up period with a mean of 10.9 years18; otherwise most OCD studies reported outcomes after 12 or 24 months on average.19–21 Due to the neurophysiological circuits implicated in OCD and the chronicity of the disease, the sustainability of the treatment response is a major issue to evaluate.
At the last follow-up (mean of 7 years), 36.8% of the patients met the criteria for full response and 10.5% qualified for partial response. Thus, the overall response rate was 47.3%, which is similar to results from other studies with shorter follow-up designs (ranging from 38% to 100%)10 ,16 ,20 ,22 ,23 as well as from the study with the longest follow-up,18 which had a response rate of 48% after 10.9 years.
We found that the maximum improvement occurred shortly after surgery, within the first 3 months, and observed no significant change during later follow-ups. Mindus and colleagues have also previously described an optimal response within the first 2 months.24
At the end of the study, 10 patients were non-responders (53%). Three were at least partial responders during the first 3 months and then relapsed, while the seven remaining patients never responded to capsulotomy. Such a transient response probably results somehow from scar tissue and oedema due to surgery. The non-responder subgroup failed to maintain initial improvements over 1 year after surgery and relapsed, probably because of brain plasticity. Interestingly, three patients did not respond until 12 months follow-up. These findings are consistent with the recommendation that it may be beneficial to wait over 1 year after the surgery to let reorganisation processes occur before drawing conclusions about the definitive effect of the procedure.21
Our results demonstrated that the patients with a poor outcome (non-responders) had a longer duration of illness at baseline than those with a better outcome (at least partial response). There is no evidence in the literature about an effect of the duration of symptoms on CBT efficacy25 or capsulotomy outcomes,1 whereas a longer duration of illness was associated with a lack of response to SRI treatment by some authors.26 ,27 In fact, it has been argued that neurosurgical treatments are currently underused considering the pool of potential patients and should be performed earlier.
Capsulotomies performed in our study were mechanical compared with more modern procedures used in others studies that performed radiofrequency or radiosurgery. A recent comparison of these latest procedures revealed lasting improvement in 48% of patients with OCD with no significant difference in benefit between procedures.18 Also, the efficacy of our procedure is comparable to that of other procedures. Here, we present results concerning a therapy that will produce an improvement in about half of patients for whom many if not all therapies had failed. These results constitute a promising alternative for many patients suffering from severe therapy-refractory symptoms. Whereas gamma radiation technology is available in few centres worldwide, thermocoagulation and mechanical lesioning procedures are more widespread. In the last few years, neuromodulation procedures have tended to supplant ablative procedures. Even if DBS is a promising treatment, only short-term results on a few patients have been published so far. Results with DBS are along the same lines as those with lesioning procedures, with the number of responders varying from 10% to 61.5%.13 ,28–32 DBS is a reversible and adjustable procedure, which also raises the possibility of a double-blind, randomised trial. However, no data are available as yet on the cost-effectiveness of DBS for OCD. This technique is clearly more expensive than lesioning procedures, implies long-term costs and could be a challenge for healthcare funding bodies, limiting its accessibility. Furthermore, patients who live in remote areas are not candidates for DBS, as any complications or urgent stimulator programming issues could not be dealt with appropriately. Therefore, there is still a place for bilateral anterior capsulotomy in neurosurgery for mental disorders, considering the low cost and the efficacy of this procedure compared with neuromodulation.
The cohort presented here was relatively homogenous in terms of OCD symptoms; most patients had forbidden thoughts/checking or contamination/cleaning symptoms. Capsulotomy has been shown to be particularly ineffective for patients with prominent symmetry/order symptoms1 and patients with hoarding symptoms also tended to benefit less from the surgery. The correlational analysis carried out on our patients did not reveal any relationship between the type of symptom and the long-term efficacy of capsulotomy (improvement at last follow-up), but the small size of our cohort could have biased the result.
In an attempt to avoid repeating the same mistakes in psychosurgery, it is important to adequately evaluate the benefits and the possible complications/side effects associated with the procedure. As reported in a recent review, complication rates related to ablative techniques are relatively low (0%–55%)18 ,33 and most of the adverse events are transient. In the present study, 11 out of 19 patients reported a surgical or medical complication. Only two patients had permanent impairment requiring rehabilitation. Considering all complications (including asymptomatic haemorrhage which had no noticeable effect on the patient), our rate of secondary events, 57.9%, is relatively similar to those reported in the literature18 ,19 ,33 ,34 but higher compared with DBS reporting minor and transient adverse events in few patients to date.32 We can therefore conclude from our results that capsulotomy is a safe procedure that can be considered with caution for patients who have no other issues.
The limitations of the present study first relate to the small sample size. However, the size of our cohort (19 patients), although limited, is comparable to the larger studies available in the literature.18 ,19 The number of patients was also too small to adequately investigate outcome predictors. Like most ablative surgery studies, our study lacked a control group. Without such a group, we could not ascertain that the improvement measured in some patients was exclusively due to surgery, even if there is little evidence for spontaneous remission or placebo effect in severe, intractable and longstanding OCD.35 Surgical follow-up was carried out by our team, but most of the patients were followed by external psychiatrists, which may add variability in long-term outcome and preclude access to certain data, such as medication.
Most of the studies published previously had a more homogenous patient sample and rarely described comorbidities, even if the great majority of patients with OCD met lifetime criteria for at least one other DSM-IV axis I diagnosis.36 Most of the patients presented in this study suffered from another axis I or II disorder, predominantly mood or personality disorders, and about one third of our patients had made a suicide attempt. Given the representativeness of our cohort of patients with OCD, our results are a better reflection of this heterogeneous population. However, this heterogeneity could have contributed to a lesser efficacy, since personality disorder could interfere with the outcome. Furthermore, the initial Y-BOCS score of our group was 34.9, which represents extreme cases of OCD; a better outcome could have been obtained in less heterogeneous and less severe cases of OCD.
Conclusion
In our limited experience, bilateral anterior capsulotomy is a relatively safe procedure that has demonstrated an antiobsessional effect in approximately half of chronic, intractable patients with OCD . The efficacy of this surgery was maintained for many years (mean of 7 years), with no newly acquired side effects. We are aware of the many ethical and sociopolitical considerations related to psychosurgery, but we think that such surgery is appropriate under thoughtful regulation, particularly when the disorder is chronic, intractable to non-invasive treatment modalities and when surgery is the last therapeutic option. Moreover, large-scale controlled studies are needed to identify reliable predictors of treatment response and then optimise the risk/benefit ratio of this surgery.
References
Footnotes
-
Acknowledgements The authors would like to thank Dr Pascale Lavoie and Dr Leon Tourian Jr for their input to this article.
-
Contributors MD participated in the study design, execution, performed the interpretation of data and drafted the manuscript. SC substantially interpreted data and revised the manuscript. MR carried out the neuropsychological assessments, interpreted data and revised the manuscript. CP participated in the design of the study and critically revised the manuscript. LC conceived of the study, interpreted data and critically revised the manuscript. All authors read and approved the final manuscript.
-
Competing interests None.
-
Ethics approval Centre hospitalier universitaire de Québec Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.