Article Text

Abstract
Background Several options exist for surgical management of essential tremor (ET), including radiofrequency lesioning, deep brain stimulation and γ knife radiosurgery of the ventralis intermedius nucleus of the thalamus. Recently, magnetic resonance-guided focused ultrasound (MRgFUS) has been developed as a less-invasive surgical tool aimed to precisely generate focal thermal lesions in the brain.
Methods Patients underwent tremor evaluation and neuroimaging study at baseline and up to 6 months after MRgFUS. Tremor severity and functional impairment were assessed at baseline and then at 1 week, 1 month, 3 months and 6 months after treatment. Adverse effects were also sought and ascertained by directed questions, neuroimaging results and neurological examination.
Results The current feasibility study attempted MRgFUS thalamotomy in 11 patients with medication-resistant ET. Among them, eight patients completed treatment with MRgFUS, whereas three patients could not complete the treatment because of insufficient temperature. All patients who completed treatment with MRgFUS showed immediate and sustained improvements in tremors lasting for the 6-month follow-up period. Skull volume and maximum temperature rise were linearly correlated (linear regression, p=0.003). Other than one patient who had mild and delayed postoperative balance, no patient developed significant postsurgical complications; about half of the patients had bouts of dizziness during the MRgFUS.
Conclusions Our results demonstrate that MRgFUS thalamotomy is a safe, effective and less-invasive surgical method for treating medication-refractory ET. However, several issues must be resolved before clinical application of MRgFUS, including optimal patient selection and management of patients during treatment.
- MRI
- Surgery
- Tremor
- Ultrasound
Statistics from Altmetric.com
Introduction
Essential tremor (ET) is the most common movement disorder in adults, with an estimated prevalence of 0.3–5.55%.1 ET is commonly viewed as a pure movement disorder with a relatively benign clinical course; however, this disorder is often not responsive to medications, and surgical treatment is frequently recommended for the management of disabling tremors.2 Stereotactic radiofrequency thalamotomy and deep brain stimulation (DBS) targeted to the ventralis intermedius nucleus of thalamus (Vim) have proven effective for treating ET and other tremors.3 Currently, DBS is more widely accepted for surgical treatment because the therapy is reversible and adjustable. Most importantly, quality of life in ET improves with unilateral and bilateral DBS therapies targeted to the Vim, and thalamic DBS is associated with long-term tremor benefits.4 ,5 However, tolerance to thalamic stimulation can occur in up to 30% of cases, and DBS has other drawbacks, including its inherent hardware-related complications, infection, haemorrhage, expense and maintenance demands.6 ,7
Recent development of less-invasive high-intensity magnetic resonance (MR) guided focused ultrasound (MRgFUS) technology has prompted investigations into its use in humans with brain tumours and neuropathic pain syndromes.8 ,9 Furthermore, unlike stereotactic radiosurgery, the treatment can be monitored continuously in real time with MRI and MR-thermography.10–12 Thus, MRgFUS brain lesioning could prove a much safer and more accurate approach compared with conventional radiofrequency thermal lesioning.
In this feasibility study, we investigated the therapeutic effects of and issues related to Vim thalamotomy with MRgFUS for medically intractable ET.
Methods
Patient selection
Patients with confirmed medication-refractory ET enrolled in this study. Patients were eligible for inclusion if they were between 18 years and 80 years of age and had received a primary diagnosis of ET, which was diagnosed by clinical history and examination by a movement disorder neurologist. Exclusion criteria included a diagnosis of a current or past psychiatric illness, current substance abuse, other neurological disorders that affect brain function such as idiopathic Parkinson's disease, contraindications for MRI, and known intolerance or allergies to the MRI contrast agent. Doses of medication for ET were stable for 30 days before enrolment and then maintained without adjustment during the study. A total of 11 patients met the inclusion criteria and underwent MRgFUS thalamotomy from March 2012 to November 2012. All patients received the standard clinical and imaging workup as part of the study's baseline requirements. All patients provided written informed consent before procedures, and this study received full ethics approval from the Korean Food and Drug Administration and local institutional review board.
Surgical procedure for MRgFUS
The entire scalp of each patient was closely shaved and the head was fixed with a Cosman-Roberts-Wells (CRW) stereotactic frame (Radionics, USA). A flexible silicone membrane with a central hole was then stretched around each patient's head and sealed to the outer face of the transducer in order to contain the degassed and chilled (15–20°C) water that was circulated in the area between the head and the transducer. This membrane was tight enough to prevent water leakage without impeding blood circulation to the scalp. The treatment was performed in a 3 T MRI system (GE medical system, Milwaukee, Wisconsin, USA) using the ExAblate 4000 device (InSightec, Haifa, Israel), which features a 30-cm-diameter hemispherical 1024-element phased-array transducer operating at 650 kHz and held by a mechanical positioner.
At the initial planning stage, Vim nucleus (14–15 mm from midline, 6–7 mm anterior to the posterior commissure and at the line of the intercommissural line) was identified. We then measured the distances from the initial coordinate to the wall of the third ventricle (optimal distance: 11–11.5 mm) and to the region around the lateral border of the thalamus (optimal distance: 2 mm), since it is the recommended target for γ-knife thalamotomy.13 ,14 Several low-power sonications below the ablation threshold were then applied for 10–20 s durations to induce peak temperatures of 40– 42°C. These sonications allowed us to assess the exact position and size of the thermal spot, and allowed us to determine the overall safety profile of the applied sonication parameters. Next, high-power sonications were applied under the guidance of MRI and MR thermometry, with stepwise increases in acoustic power and energy in order to finally achieve a peak target temperature of 55–62°C. After making a lesion with the abovementioned methodology, we made a second, larger lesion to aid in tremor treatment. This second lesion was especially important in cases where tremor was not sufficiently improved with the first lesion. The target direction of second lesion was determined according to tremor response to the first lesion and based on the development of adverse effects during test sonications.
During the entire series of sonications, patients were repeatedly examined and questioned to ensure their neurological integrity and to assess (1) changes in pain quality, extension and intensity; (2) potential somatosensory improvements; (3) the appearance of somatosensory, vestibular and/or vegetative manifestations experienced during the treatment; (4) the absence of any motor or somatosensory deficit and (5) any other unbearable discomforts or adverse effects from sonications.
Follow-up evaluations after MRgFUS
Tremor severity and functional impairment were assessed with the clinical rating scale for tremor (CRST)15 at baseline and then at 1 week, 1 month, 3 months and 6 months after treatment. Adverse effects were sought and ascertained by open-ended and directed questions and by neurological examination. Conventional 3 T MRIs (GE medical system, Milwaukee, Wisconsin, USA) were then serially performed on 1 day post-treatment, or at 1 week, 1 month, 3 months and 6 months post-treatment.
Statistical analysis
Clinical and imaging data were analysed together. To compare MR-induced vertigo (MRIV) and related factors, the non-parametric Mann-Whitney U test was used. Linear regression was used for analysing the correlation between maximal rise in temperature and skull volume statistical tests were performed using SPSS V.18.0 (NCSS statistical software, Kaysville, Utah, USA), and were all two-tailed. The threshold for statistical significance was set at p<0.05.
Results
Patient demographics and clinical outcomes
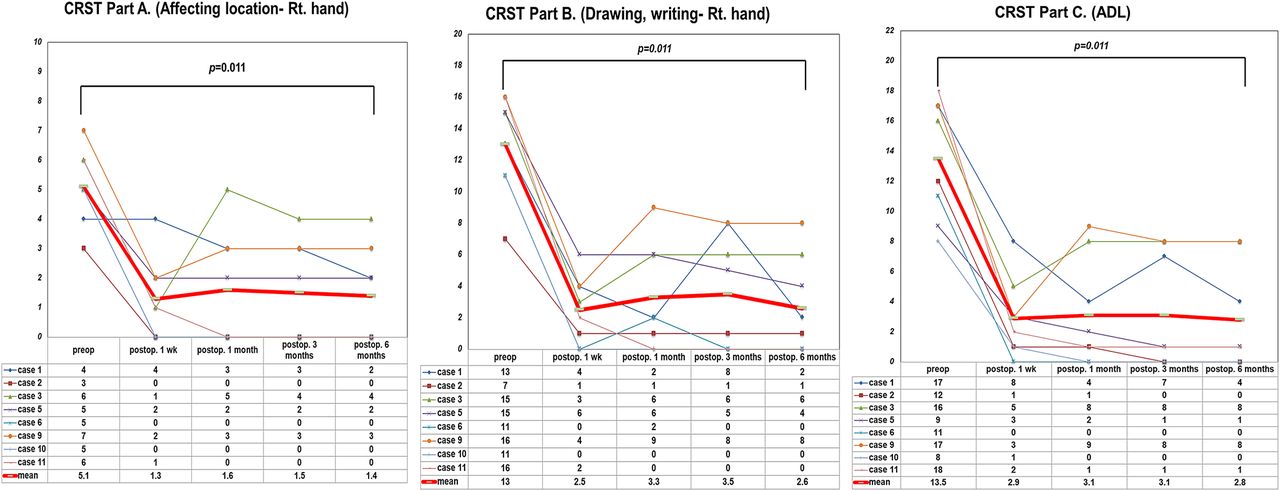
Serial axial T2-weighted MRIs of left Vim thalamotomy demonstrated a small and accurate lesion in the Vim thalamic nucleus (figure 1). MRgFUS treatment could only be considered complete in 8 of 11 patients (table 1). Tremor improvement was evaluated using CRST for these eight patients; results are listed in figure 2. At a postoperative period of 6 months, part A of the CRST was remarkably improved from 5.1 to 1.4 with MRgFUS. In the 6-month postoperative period, part B of the CRST was also improved from 13 (preoperative state) to 2.6, and part C was improved from 13.5 (preoperative state) to 2.8 (figure 2).
Patient demographics

Follow-up results with conventional 3 T MRI. MRgFUS, magnetic resonance-guided focused ultrasound.
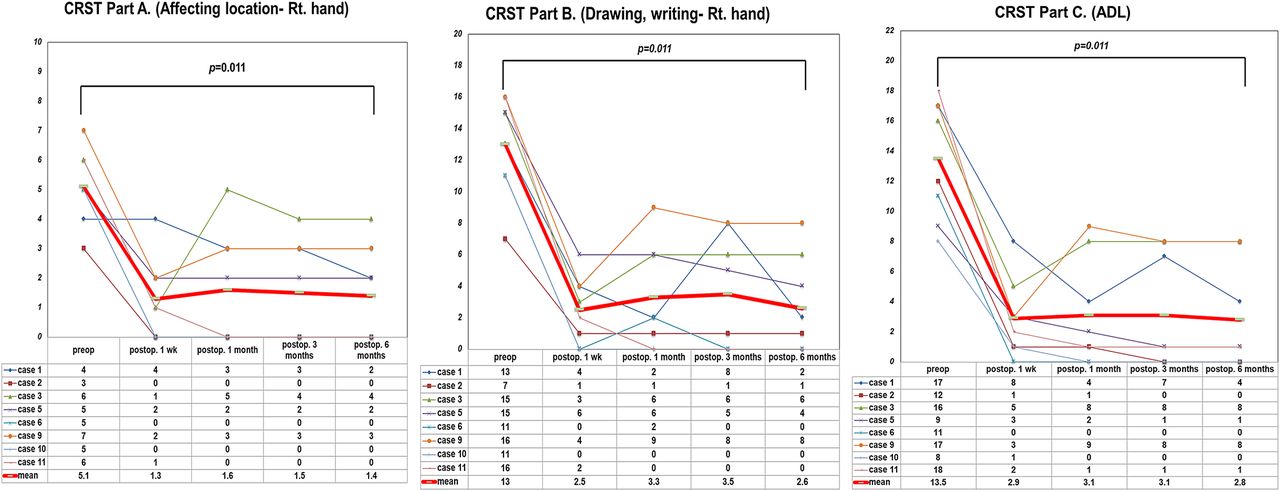
CRST changes before and after MRgFUS thalamotomy in successful cases, and comparison of pretreatment and post-treatment 6 months’ score. Non-parametric Wilcoxon test, p=0.011 (CRST Part A), p=0.011 (CRST Part B) and p=0.011 (CRST ADL). ADL, activity of daily living; CRST, clinical rating scale for tremor.
Rise in temperature during MRgFUS thalamotomy
The mean peak focal temperature achieved in the MRgFUS treatments was 53+3.3°C (range 48–61°C). We were unable to make significant thermal lesions in 3 out of the 11 patients (Cases 4, 7 and 8) because of inadequate increases in temperature (below 50°C). In these cases, we tried to increase the temperature by increasing sonication energy; however, the maximal temperature we were able to achieve was still under 42°C even with up to 24 000 J (1200W-20 s) and 28 times the originally applied sonication energy. Interestingly, measurements of larger skull volume above the anterior commissure-posterior commissure (AC-PC) line (HU 100–2000, AquariusNET V.4.4.6 (TeraRecon, San Mateo, California) were correlated to those cases in which we could not achieve adequate temperatures (figure 3).

Measurement of skull volume in treatment field (A) and correlation between maximal rise in temperature and skull volume (B) (one case of cardiac symptom during treatment was excluded. Linear regression, p=0.003).
Follow-up MR studies using conventional 3.0 T MR
MRIs were immediately taken post successful MRgFUS treatments, and again at 1 day, 1 week, 1 month, 3 months and 6 months following the MRgFUS thalamotomy. MRI sequences included T1-weighted (with and without contrast enhanced), T2-weighted, diffusion images and treated area tracking changes over time (figures 1, 4). Signal changes in T2-weighted and T1-weighted images were prominent until 1 month after MRgFUS treatment, which faded out and became invisible in images taken 3 months and 6 months after the procedure. Interestingly, contrast enhancement patterns of T1-weighted images also showed serial changes. On immediate post-MRgFUS images, rim enhancement was observed at the treatment area, but this enhancement disappeared 1 day postoperatively suggesting that this phenomenon could have been caused by permeability changes of the blood-brain barrier after MRgFUS.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Volume changes of lesions after MRgFUS thalamotomy (measured by GammaPlan 10.0.0, Elekta, Sweden). N/A, not assessable due to fade out; MRgFUS, magnetic resonance-guided focused ultrasound.
Complications during and after MRgFUS
We noticed that 5 out of the 11 patients suffered from various vestibular symptoms such as dizziness, nausea and vomiting in the middle of sonications. There was no statistical difference in the average time in MR room between patients with and without vestibular symptoms (260 min for patients with vestibular symptoms vs 227 min for those without vestibular symptoms, p=0.361) (table 2).
Magnetic resonance-induced vertigo (MRIV) during magnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy
Additionally, we had one patient with transient mild balance problems due to the oedema adjacent to the medial lemniscus. This patient was prescribed oral steroid therapy for 1 month, after which the patient recovered to normal. No other patient reported any other side effects.
Discussion
Clinical efficacy of MRgFUS
We found that MRgFUS provided effective tremor control with minimal adverse effects for patients with ET. Compared with conventional surgical approaches such as DBS, radiofrequency thalamotomy or γ thalamotomy, MRgFUS has substantial advantages for the management of disabling tremor given its capability to evaluate appropriate targets and symptoms during the procedure. For example, based on location determining via MRI, the size of the lesion can be enlarged in accordance with the degree of symptom improvement. In the current study, initial MRI findings after thermal lesions were made, using MRgFUS, were similar to those observed after radiofrequency thalamotomy. Additionally, we found that the temperature required for making a solid lesion with MRgFUS was usually less than 60°C, a temperature much lower than what is needed to make lesions using the radiofrequency approach.16
In this feasibility study, we demonstrated that MRgFUS treatment has stable and beneficial effects in the treatment of ET that extend to more than 6 months. Theoretically, the adverse effects of MRgFUS are predicted to be similar to those of conventional radiofrequency thalamotomy since damaging critical areas near the motor thalamus are possible in both techniques. However, the risk of incurring such damage using the MRgFUS approach is very low because of the capability to monitor lesions during sonications in real time.
Like γ knife thalamotomy, MRgFUS is a less invasive approach to interventions that target the thalamus. However, there are some differences between MRgFUS and γ knife treatment. For example, γ knife treatment can result in delayed side effects due to ionising radiations used by γ knife technology.17 In contrast, coupled with the advantage that MRgFUS can modify the target site and treatment parameter during the procedure, usage of ultrasonic energy has an added benefit regarding safety. There are two major mechanisms by which ultrasonic energy exerts its biological effect: thermal effect and non-thermal effect.18 Considering that thermal ablation techniques have been used for more than 50 years, we can assume that unexpected or delayed adverse effect may result from non-thermal mechanism. Non-thermal effects of ultrasonic energy are caused by alternating pressure, which can form air bubbles termed acoustic cavitations. The effect of acoustic cavitation on brain tissue is still under investigation, and therefore the production of these bubbles should be avoided during MRgFUS treatment. Current MRgFUS procedures give a solution for this problem by allowing for real-time monitoring of cavitation signals MRI. Therefore, it seems that MRgFUS might be safer in aspects of delayed or unexpected adverse effects; however, this cannot be verified until long-term follow-up data are available.
Targeting of Vim nucleus during MRgFUS thalamotomy
Currently, there are two methods for targeting specific nuclei during stereotactic surgery: anatomical targeting or electrophysiological targeting. Anatomical targeting included AC-PC based indirect and direct targeting with personalised imaging data. Both methods of anatomical targeting have their limitations. For example, indirect targeting does not consider individual differences in the shape and size of each nucleus, while direct targeting cannot be used if the border of the target nucleus is invisible in imaging data. To overcome these limitations, data for electrophysiological targeting especially microelectrode recordings (MERs) are usually used during stereotactic surgery. MER data can help in identifying target nucleus by observing specific firing patterns of each nucleus and detecting responses to motor and sensory stimulations. MER also can be helpful for demarcating the border of the target nucleus. As previously mentioned, one of the most important advantages of MRgFUS thalamotomy is that a skin incision is not needed during the procedures; however, this advantage limits the extent to which MER can be used during procedures. Therefore, targeting of the Vim nucleus during MRgFUS thalamotomy should be mainly restricted to anatomical targeting.
In the current study, we used direct and indirect methods for determining the target location of the Vim, referring to experiences from various thalamic procedures such as γ knife thalamotomy, radiofrequency thalamotomy and thalamic DBS. Additionally, we used neurological responses especially in sensory changes during test sonications, to identify the posterior border of the Vim. The ventralis oralis posterior (Vop) nucleus is located at the anterior border of Vim. Because the Vop was mainly connected to the pallidal circuit, test sonications to this area usually did not elicit any neurological changes. Although this means that lesioning of the Vop is relatively safe, it also makes it hard to demarcate the Vim-Vop border by test sonication. Furthermore, considering that the width of the lesion by MRgFUS was about 5 mm, similar to the anterior-posterior distance of the Vim, there was a possibility that the lesion could include a part of the Vop nucleus. To avoid making the main lesion at the level of the Vop nucleus, we carefully observed the changes of tremor symptoms during test sonications since the Vop is usually ineffective in controlling.13 If tremor suppression was not observed with test sonication, we changed the focus to a more posterior location and repeated sonication. With this step-by-step approach, we determined the optimal target for tremor suppression, and made a permanent lesion at the target site. We also determined the direction that we needed to move the sonication focus in for the next lesion. By using these targeting methods, we were able resolve tremors in all patients after MRgFUS thalamotomy if lesions were successfully made by this procedure. These results suggest that this targeting approach was suitable for controlling tremors even in cases where minor regions of the Vop nucleus were affected.
Optimal timing for imaging follow-ups: discordance between clinical and radiological findings
Imaging data can represent structural changes after surgical procedures, and most neurosurgeons take postoperative MRIs to predict surgical outcome and patient prognosis. However, optimal timing for taking MRIs is still controversial because postoperative changes, including soft tissue swelling, fluid collection and haematoma formation, can prohibit exact evaluation and interpretation.19 Elias WJ et al studied comparative analyses of imaging and histological changes after focused ultrasound, radiofrequency and radiosurgery lesions in the swine thalamus.20 In this comparative study, it was determined that focused ultrasound induced tissue necrosis and perilesional oedema and that these changes could be clearly visualised within 10 days of the procedure. However, these lesion cavities collapsed by 1 month, making it difficult to visualise them using MRI.
In our study, MRIs were also taken immediately after MRgFUS treatment as well as 1 day, 7 days, 1 month, 3 months and 6 months post-treatment (figures 1, 4). Because there has been no available information on imaging changes after human MRgFUS treatment, we worried that there might be unexpected transient or permanent alterations induced by MRgFUS. Furthermore, we did not have information about the optimal timing for taking MRIs to treatment outcome. Therefore we took MRIs over short intervals in order to obtain as much information as we could about imaging changes that occurred after MRgFUS treatment. Interestingly, target site changes were clearly visible on T2-weighted and T1-weighted images taken before the 1-month follow-up scan. However, these changes faded out as time progressed, and became nearly invisible on MRIs taken 6 months after treatment. This phenomenon has also been observed in other MRgFUS thalamotomy studies, which obtained follow-up images up to 3 months after treatment.21 ,22 In contrast, one report using MRgFUS thalamotomy for neuropathic pain continued imaging follow-ups for 1 year after treatment and were able to show discrete lesions over the treated areas.9 Taken together, 7–10 days after treatment should be regarded as the optimal time for estimating target locations and acute changes in affected tissue. Additionally, in cases where assessment of chronic changes is desired, MRI scans should be postponed for more than 6 months after treatment.
Another interesting result of this study was discordance between clinical and radiological findings. As mentioned above, lesions produced by MRgFUS treatment have been reported to fade out as time progresses. However, clinical benefits continued until 6 months after treatment. At the early stage of this trial, we worried about the durability of this treatment because of this phenomenon. Tolerance of surgical treatment for ET is not uncommon in long-term follow-ups of DBS.23 Therefore, although clinical improvement persisted until 6 months after treatment, there is still a possibility of delayed tolerance. Therefore, longer follow-up periods are needed for clinical and radiological evaluations.
Other unsettled issues of MRgFUS: effect of skull volume and thickness on rises in temperature
The concept of high-intensity focused ultrasound surgery was introduced in the early 1940s.24 However, it has taken a long time to be able to apply this technique in neurosurgical fields because the skull served as a barrier for transmitting ultrasonic energy into the brain. By developing the phased array technique, this problem seemed to be overcome, with one study demonstrating that it was possible to focus ultrasonic energy into the brain without craniotomy by using a 500-element ultrasonic phased array system.25
In our study, we failed to achieve a sufficiently high temperature at the target area of 3 cases out of the 11 participants. Possible reasons for this failure could be due to incomplete technology for transmitting energy by the skull, mechanical and/or technical errors, and unknown human factors. Because eight patients underwent successful treatment by this machine, we focused on the unknown factors, especially in relation to the skull. Interestingly, when we calculated skull volume, we found that there was a linear correlation between skull volume and maximum temperature achieved at the target area (figure 3). Although many other factors including skull shape, cortical and bone marrow densities, the ratio of cortical and bone marrow, and the angle of introducing ultrasound into the skull could possibly affect energy focusing, it seems to be the case that human factors, especially regarding the skull, are still a major problem for focusing energy at a target area. Therefore, along with demonstrating safe levels for sonication in order to avoid cavitation signals or complications such as bleeding, this problem should be solved before MRgFUS technology is used in clinical settings.26
Other unsettled issues of MRgFUS: high field MR-induced vertigo
During the procedure, about half of the patients experienced transient vestibular symptoms that mimicked the state of motion sickness, which included symptoms of nausea, vomiting and dizziness (table 2). Initially, we interpreted this phenomenon to be a result of severe anxiety. However, the incidence of this symptom was higher than we expected, so other possible factors must be considered.
One possible explanation could be attributed to magnetic field exposure which could exert effects ranging from cellular structure alterations to changes in vital signs, and even cognition and behavioural impairments.27 MRIV is also a relatively well-known phenomenon when patients are exposed to high-field MRI (>2.0 T), and symptom severity is known to proportionally increase according to the time of exposure and strength of the magnetic field.28 Although the effects of the magnetic field in the current study were usually transient and self-limiting, some patients could not tolerate the vestibular symptoms and needed to rest before continuing the procedure. This feasibility study also demonstrated that the current MRgFUS approach is mildly inconvenient for patients because of longer procedure times and potential issues such as dizziness during MRI. The duration of MRgFUS treatment is mainly related to sonication and cooling times. Considering the fact that sonication time is usually less than 20 s, cooling time after sonication is the main time-consuming component of this procedure. Moreover, cooling time proportionally increases when higher energy is delivered to the focus. Therefore, treatment time can be shortened by reducing the number of high-power sonications.
Since our study was a feasibility trial, we did not have much information about the tissue response after high-power sonication. Additionally, we also lacked information about the relationship between sonication power and temperature changes. Because of these gaps in knowledge, we increased sonication power very gradually, which may explain the lengthy procedure. Thus, the investigator and technical developer should make continuous efforts to decrease time of treatment and magnetic field exposure. The number of high-power sonications could be reduced by gaining more experience, and subsequently, it is expected that this will decrease treatment time and reduce the risk of MRIV.
Conclusions
The results of this feasibility study demonstrate the significant beneficial effects of MRgFUS treatment in patients with ET. This approach has several advantages over other conventional surgical techniques such as DBS, radiofrequency thalamotomy and γ knife thalamotomy. First, unlike DBS or radiofrequency thalamotomy, MRgFUS is less invasive. Second, the procedure is done in a MRI room where temperature can be selected and monitored in real time using MRI thermography, and where the lesion size and its location in the thalamus can be precisely visualised. These real time capabilities give surgeons the chance to make immediate adjustments if they are necessary. Additionally, thermal monitoring allows for safe and accurate lesioning without the need for physiological monitoring such as microelectrode recordings. Lastly, this approach is also superior for making immediate and optimal lesions in the motor thalamus compared with blind lesions with delayed responses characteristic of the γ knife thalamotomy approach. However, several issues must be resolved before clinical application of MRgFUS, including optimal patient selection and management of patients during treatment.
References
Footnotes
-
Acknowledgements This study was supported by a research grant from InSightec (Haifa, Israel) for clinical trial using the transcranial MRgFUS. InSightec was the regulatory sponsor of this study, and provided technical assistance. This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Contributors JWC, WSC conceived and designed the clinical trial. EZ and IR provided technical support, and execution and description of the methods. JWC, WSC, HHJ and EJK performed the procedures and provided pre-MRgFUS, intra-MRgFUS and post-MRgFUS assessments. JWC, WSC wrote the first draft of the manuscript, and all authors contributed to and approved the final manuscript.
-
Competing interests EZ and IR are employees of InSightec.
-
Patient consent Obtained.
-
Ethics approval Institutional review board of Severance hospital, Seoul, Korea.
-
Provenance and peer review Not commissioned; externally peer reviewed.