Article Text

Abstract
Objective Whether statins increase the risk of intracerebral haemorrhage (ICH) in patients with a previous stroke remains uncertain. This study addresses the evidence of statin therapy on ICH and other clinical outcomes in patients with previous ischaemic stroke (IS) or ICH.
Methods A systematic literature review and meta-analysis was performed in conformity with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines to assess observational and randomised studies comparing statin therapy with control (placebo or no treatment) in patients with a previous ICH or IS. The risk ratios (RR) for the primary outcome (ICH) and secondary outcomes (IS, any stroke, mortality and function) were pooled using random effects meta-analysis according to stroke subtype.
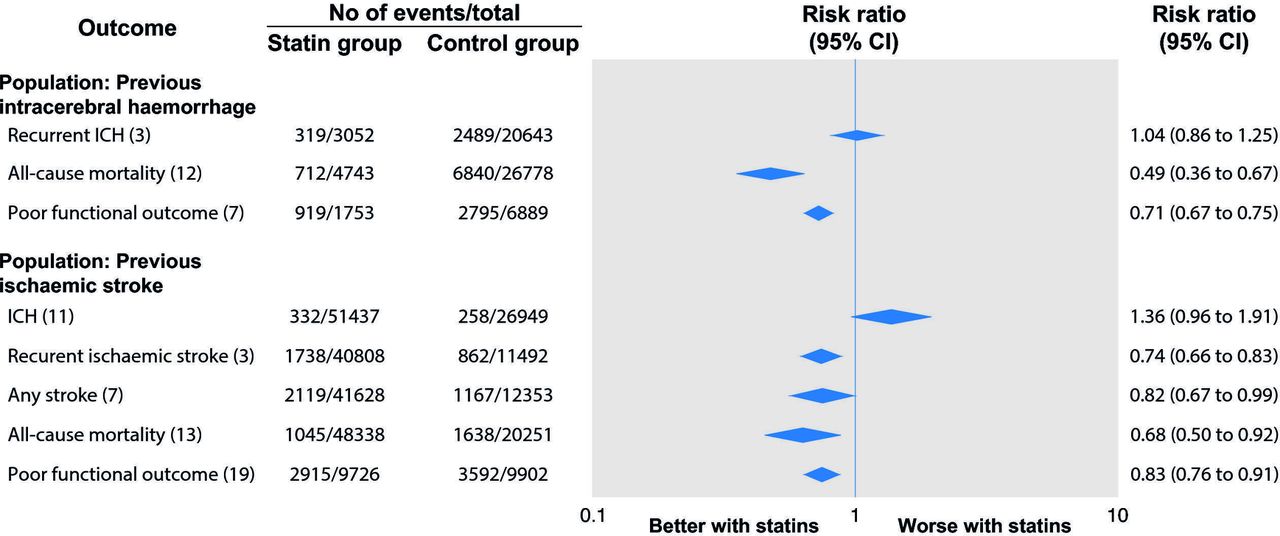
Results Forty-three studies with a combined total of 317 291 patient-years of follow-up were included. In patients with previous ICH, statins had no significant impact on the pooled RR for recurrent ICH (1.04, 95% CI 0.86 to 1.25; n=23 695); however, statins were associated with significant reductions in mortality (RR 0.49, 95% CI 0.36 to 0.67; n=89 976) and poor functional outcome (RR 0.71, 95% CI 0.67 to 0.75; n=9113). In patients with previous IS, statins were associated with a non-significant increase in ICH (RR 1.36, 95% CI 0.96 to 1.91; n=103 525), but significantly lower risks of recurrent IS (RR 0.74, 95% CI 0.66 to 0.83; n=53 162), any stroke (RR 0.82, 95% CI 0.67 to 0.99; n=55 260), mortality (RR 0.68, 95% CI 0.50 to 0.92; n=74 648) and poor functional outcome (RR 0.83, 95% CI 0.76 to 0.91; n=34 700).
Conclusions Irrespective of stroke subtype, there were non-significant trends towards future ICH with statins. However, this risk was overshadowed by substantial and significant improvements in mortality and functional outcome among statin users.
Trial registration number CRD42017079863.
Statistics from Altmetric.com
Introduction
Statin therapy has routinely been used to inhibit cholesterol synthesis and avoid cardiovascular events throughout the last three decades. They are recommended by both American and European guidelines to reduce risk of stroke and cardiovascular events in patients with cerebrovascular disease.1 2 Despite the demonstrated beneficial effects of statins in preventing first ever stroke, prescriptions remain suboptimal with age, gender, racial and geographic discrepancies.3 This may partially be explained by concerns around the potential risk of intracerebral haemorrhage (ICH) with statins due to their antiplatelet and anticoagulant effects, particularly in patients with a previous ICH.4 5
In two large randomised trials, Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL)6 and Heart Protection Study (HPS),7 the benefit in reducing recurrent ischaemic stroke was offset in part by an increased risk of haemorrhagic stroke. A risk benefit decision analysis of statin therapy in patients with prior ICH concluded that statin avoidance should be considered following ICH particularly in those with lobar ICH.8 Conversely, two meta-analyses of randomised trials enrolling patients without prior stroke found no significant association between statins and ICH with significant reductions in all-stroke and all-cause mortality with statin therapy.9 10 Additionally, statin use after ICH was associated with early neurological improvement at 6 months.11 There is, therefore, a clear imperative to define the place of statins in the clinical management of patients with a previous stroke at future risk of ICH.
In view of the potential usefulness of statins in patients with a previous stroke, and in an attempt to settle the uncertainty over adverse clinical outcomes, we assessed the efficacy and safety of statins by comprehensively meta-analysing all available observational and experimental studies. We aim to build on the previous meta-analyses by focusing on studies in which patients had an established ischaemic or haemorrhagic stroke. We used metaregression techniques to evaluate the association of study characteristics with the risk of clinical outcomes.
Methods
Eligibility criteria and search strategy
All studies comparing clinical outcomes in participants treated with statins and control (placebo or no treatment) were evaluated, regardless of study design. We excluded studies where statins were used for primary prevention or did not provide comparative outcomes. Studies assessing secondary prevention of cerebrovascular disease were included. The definitions of ICH and ischaemic stroke used by each individual study were accepted. A systematic review of MEDLINE (1960 to June 2017), EMBASE (1980 to June 2017) and the Cochrane Library (until June 2017 issue) was performed. The search strategy included keywords and MeSH terms relating to statins and ICH, ischaemic stroke, death and functional outcomes. We manually searched reference lists of relevant studies, investigated registers of ongoing trials and included studies after discussion with content experts. The review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and was prospectively registered with the PROSPERO database of systematic reviews (CRD42017079863).12
Data collection, synthesis and risk of bias
Two investigators (OJZ and GB) independently extracted and tabulated data in a standardised data extraction form. Discrepancies and missing data were resolved by group discussion, reference to the original publication and additional independent adjudication (DJW). All data were extracted from studies, including crude outcomes and adjusted analyses (multivariate adjustment and propensity matched). Careful note was made of the analysis method (including risk ratio (RR; preferred), OR or HR) and the population studied. Risk of bias was assessed with the Cochrane Collaboration’s Risk of Bias Tool for Randomised Controlled Trials (RCT) and the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS), which address key criteria including selection bias, exposure measurement, blinding and selectivity of reporting. Assessment of bias risk was performed independently from data extraction, with each study assessed by two authors.
Primary and secondary outcomes
The predefined primary outcome was ICH. Secondary outcomes included ischaemic stroke, any stroke, all-cause mortality and poor functional outcome. The definitions used by each individual study were accepted. To investigate whether treatment effects vary between stroke types, analyses were subgrouped by previous ICH and previous ischaemic stroke.
Statistical analysis
Baseline demographics in the statin and control groups were compared using meta-analysis and summarised as the OR. Random effects meta-analysis was prespecified to combine estimates from different studies. Pooled binary event data for statin and control cohorts were compared using an RR with associated 95%CIs using the method of DerSimonian and Laird. In cases where the OR was described, these were converted to RR (RR=OR/([1−pRef] + [pRef*OR]), where pRef is the prevalence of the outcome in the reference group). RR and corresponding CI were log-transformed before pooling. HRs were included in the systematic review but not meta-analysis due to a scarcity of results presented in this way.
Where studies reported several results for the same outcome, we extracted the result based on the longest follow-up duration and most adjustment factors. Sensitivity analyses were performed according to study design (randomised trials and observational cohorts). The degree of heterogeneity between studies was quantitatively assessed using the I2 statistic (I2 of≥50% indicates substantial heterogeneity, ≥75% suggests considerable heterogeneity). Metaregression was performed to quantify the heterogeneity, assess the impact of baseline variables and risk of bias on estimates of each outcome, according to stroke subtype. Publication bias was evaluated by inspection of funnel plots and quantitatively assessed using Begg’s and Egger’s tests to identify small-study effects. A p value<0.05 was considered statistically significant. Analyses were performed using STATA V.13.1 (StataCorp, Texas).
Results
The search strategy identified 51 studies for systematic review, including 1 324 450 patients on statin therapy or control (placebo or no treatment) and 4 098 285 patient-years of follow-up (online supplementary efigure 1). Of the 51 studies, 36 were observational,11 13–46 and 15 were randomised on the basis of statin therapy.6 7 47–59 Study descriptors are summarised in online supplementary etable 1. Forty-three studies were suitable for inclusion in the quantitative meta-analysis comparing statins with control in patients with a previous stroke. Of the 43 studies, 15 provided data on patients with a previous ICH6 11 17 34–36 38–44 47 48 and 29 reported outcomes in patients with a prior ischaemic stroke.13–15 17–32 45 46 49–56 A total of 84 356 patients were taking statins (47.1%) compared with 94 597 in the control arms (52.8%). The weighted average length of follow-up was 1.77 years with a range of 0.1–7.0.
Differences in key characteristics between statin and control groups are summarised in table 1 (for full baseline demographics, see online supplementary etable 2). Patients receiving statins had more diabetes, hypertension, hyperlipidaemia and coronary artery disease than controls and were more often receiving anticoagulant and antiplatelet drugs.
Pooled weighted characteristics
Meta-analysis was performed for five outcomes: ICH, ischaemic stroke, any stroke, all-cause mortality and functional outcome. A summary of the individual meta-analyses performed is presented in figure 1 and detailed results are discussed below. The risk of bias in individual studies is presented in online supplementary etables 3 and 4. As expected, this was proportional to the robustness of study design, with RCTs having the lowest risk of bias. There was no evidence of small-study effects or publication bias in any of the outcomes assessed (all Egger’s p>0.1).

Summary of meta-analyses in observational and randomised studies on safety and efficacy of statins in patients with previous stroke (total studies). See figures 2 and 3 for study-level results. ICH, intracerebral haemorrhage.
Population: previous ICH
Fifteen studies of patients with previous ICH were suitable for meta-analysis (n=50 374; table 2; figure 2).6 11 17 34–36 38–44 47 48
Summary of studies and patients according to cerebrovascular disease subtype

Forest plot of studies on association between statins and clinical outcomes in patients with previous intracerebral haemorrhage. The diamond represents the pooled difference using a random effects model. I2 is the percentage of total variation across studies due to heterogeneity. Egger’s test of small-study effects: ICH p=0.16; all-cause mortality p=0.88; poor functional outcome p=0.58. Poor functional outcome was defined as modified Rankin Scale (mRS) >2 by all studies, except those by Dowlatshahi et al 36 which defined as mRS>3, Tapia-Perez et al 11 42 which defined as National Institutes of Health Stroke Scale (NIHSS) >15 and Winkler et al 43 which defined as modified Barthel Index (mBI) <15. ICD, International Classification of Diseases; ICH, intracerebral haemorrhage; RR, risk ratio.
Outcome: recurrent ICH
One randomised and two observational studies of statins in patients with previous ICH reporting the outcome recurrent ICH were included (n=23 695).34 44 47 There was no difference in recurrent ICH between patients on statin and control (RR 1.04, 95% CI 0.86 to 1.25, p=0.70). Two additional studies providing HRs were both concordant with this neutral result.33 37 Sensitivity analysis of study design demonstrated that although there was no significant difference between the randomised and observational studies, the observational studies had a noteworthy lower pooled relative risk than the randomised SPARCL subgroup (RR 1.02, 95% CI 0.89 to 1.16 vs RR 3.73, 95% CI 0.83 to 17.0; see figure 1, online supplementary etable 5).
Outcome:ischaemic stroke
One substudy of statins in patients with previous ICH (n=93) reported a non-significant increase in incident ischaemic stroke (RR 1.60, 95% CI 0.28 to 9.14).47
Outcome: any stroke
One substudy of statins in patients with previous ICH (n=93) reported a non-significant increase in any stroke (RR 2.67, 95% CI 0.90 to 7.90, p=0.08).47
Outcome: all-cause mortality
In 15 studies with previous ICH (n=89 976) there was a significant reduction in all-cause mortality with statins versus control (RR 0.49, 95% CI 0.36 to 0.67, p<0.001) but with significant heterogeneity (I2=91.7%, p<0.001).6 11 17 34–36 38–41 43 48 Two additional studies reporting HRs were consistent with this finding.33 42 Sensitivity analysis of study design demonstrated that observational studies had a lower pooled relative risk than the randomised analyses (RR 0.46, 95% CI 0.33 to 0.63 vs RR 1.03, 95% CI 0.47 to 2.49; see online supplementary etable 5).
We performed an exploratory metaregression of the impact of differences in key baseline characteristics on all-cause mortality between statin and control patients. This analysis demonstrated that the mortality of benefit of statins was diminished when the statin group was composed of a smaller proportion of men than the control cohort (p=0.003; online supplementary etable 5). Additionally a greater mortality benefit with statins was associated with a more recent year of publication (p=0.01).
Outcome: poor functional outcome
Seven studies of patients with previous ICH reported functional outcome (n=9113), demonstrating a significant reduction in poor functional outcome among statin users compared with control (RR 0.71, 95% CI 0.67 to 0.75, p<0.001).11 17 36 40–43
Population: previous ischaemic stroke
Twenty-nine studies of patients with previous ischaemic stroke were suitable for meta-analysis (n=128 579; table 2; figure 3).13–15 17–32 45 46 49–56

{kind=link}
{kind=link}
{kind=link}
Forest plot of studies on association between statins and clinical outcomes in patients with previous ischaemic stroke. The diamond represents the pooled difference using a random effects model. I2 is the percentage of total variation across studies due to heterogeneity. Egger’s test of small-study effects: ICH p=0.78; ischaemic stroke p=0.30; any stroke p=0.52; all-cause mortality p=0.54; poor functional outcome p=0.69. Poor functional outcome was defined as modified Rankin Scale (mRS) >2 by all studies, except those by Alvarez-Sabin et al 14 and Song et al 30 which defined as being dependent, and Leker et al 24 as mRS >3. CEA, carotid endarterectomy; RR, risk ratio; TIA, transient ischaemic attack; tPA, tissue plasminogen activator.
Outcome: ICH
Eleven studies of statins in patients with prior ischaemic stroke reporting ICH were included (n=103 525).15 18–21 23 26 29 45 51 52 There was a non-significant increase in ICH with statins compared with control (RR 1.36, 95% CI 0.96 to 1.91; p=0.08) but with substantial heterogeneity (I2=79.3; p<0.001). In studies that enrolled only patients with an ischaemic stroke undergoing thrombolysis for ischaemic stroke there was a non-significant increase in ICH with statins (RR 1.61, 95% CI 0.77 to 3.34; p=0.20) compared with the remaining six studies without thrombolysis (RR 1.21, 95% CI 0.83 to 1.76; p=0.33).15 18 19 29 45 Sensitivity analysis of study design demonstrated that observational studies had a lower pooled relative risk than the randomised trials (RR 1.73, 95% CI 1.20 to 2.49 vs RR 1.28, 95% CI 0.85 to 1.93; see online supplementary etable 5).
An exploratory metaregression of the effect of study-level bias demonstrated that studies with lower bias reported a greater association of statins with ICH (p=0.017; online supplementary efigure 2). This was supported by a sensitivity analysis of study design, where the pooled two randomised trials reported a significant increase in ICH (RR 1.73, 95% CI 1.20 to 2.49; p=0.004), while the nine observational studies reported a neutral association (RR 1.28, 95% CI 0.85 to 1.93; p=0.23). Metaregression was used to explore the impact of differences in key baseline characteristics between statin and control patients on ICH. This revealed that studies with a similar incidence of hyperlipidaemia in both the statin and control groups were associated with increased ICH with statins (p=0.002). Conversely, studies where patients had a higher incidence of hyperlipidaemia in the statin group compared with control were associated with reduced ICH with statins. Additionally, studies with larger proportion of men in the statin arm were more likely to report an increase in ICH with statins (p=0.025)
Outcome: recurrent ischaemic stroke
Three studies of patients with previous ischaemic stroke (n=53 162) revealed a reduction in recurrent ischaemic stroke with statins compared with control (RR 0.74, 95% CI 0.66 to 0.83; p<0.001).23 51 52 Two additional studies reporting HRs were both consistent with this outcome.21 60
Outcome: any stroke
Seven studies with previous ischaemic stroke were included (n=55 260).23 46 49–52 54 There was a borderline significant reduction in any stroke with statins compared with control (RR 0.82, 95% CI 0.67 to 0.99; p=0.04) but with significant heterogeneity (I2=72.9; p=0.001).
Outcome: all-cause mortality
In 13 studies pertaining to the prior ischaemic stroke cohort (n=74 648), there was a reduction in all-cause mortality with statins compared with control (RR 0.68, 95% CI 0.50 to 0.92, p=0.01)13 17 18 23 25 29 30 32 45 46 52 55 56 but with considerable heterogeneity (I2=86.5; p<0.001). Two additional analyses reporting HRs both demonstrated significant reductions in mortality.16 22 Sensitivity analysis of study design demonstrated that although there was a significant reduction in mortality in the pooled observational studies (RR 0.60, 95% CI 0.42 to 0.85) there was no statistical difference in the pooled randomised analyses (RR 1.04, 95% CI 0.87 to 1.24; online supplementary etable 5).
Outcome: poor functional outcome
Twenty-one analyses (n=34 700) in 19 studies of patients with prior ischaemic stroke reported functional outcome. Together these demonstrated that statin use was significantly associated with a reduction in poor functional outcome compared with control (RR 0.83, 95% CI 0.76 to 0.91, p<0.001) although with significant heterogeneity (I2=85.8; p<0.001).13 14 17–19 22 24–32 45 52 53 56
Discussion
In our comprehensive meta-analysis including a combined total of over 300 000 patient-years of follow-up we found that in patients with a previous ICH, statins were not associated with an increased risk of recurrent ICH. In patients with previous ischaemic stroke, we found a clear benefit of statins in reducing recurrent ischaemic stroke at the expense of a non-significant increase in ICH. Statins were associated with substantial and significant improvements in mortality and functional outcome irrespective of stroke subtype.
Previous ICH
Statins exert beneficial cardiovascular pleotropic effects on endothelial dysfunction through normalising vasomotion, increasing bioavailability of nitric oxide and supressing inflammatory responses.61 However, the antiplatelet and anticoagulant effects of statins have raised concerns that they may increase the risk of ICH. Statins have also been hypothesised to have potentially harmful consequences in acute ICH where their diverse pharmacological properties may contribute to haematoma expansion.62 In both the HPS and SPARCL trials, which enrolled patients with a previous stroke, statins were associated with increased ICH compared with placebo.7 52 Of these two trials, only SPARCL provided a subgroup analysis of patients with a previous haemorrhagic stroke, demonstrating a non-significantly increased risk of recurrent ICH.47 In contrast, four larger observational cohort studies all demonstrated a neutral effect of statins on recurrent ICH,33 34 37 44 consistent with our findings.
We found that in ICH survivors statins were associated with improved mortality and functional outcome with no significant effect on recurrent ICH. We were unable to meta-analyse the outcomes ischaemic stroke and any stroke type as the only data available were from the haemorrhagic stroke subgroup population of the SPARCL trial (n=93).47 These results do not support withholding statins after ICH, but large RCTs are still needed to consolidate these findings.
Most ICHs are due to cerebral small vessel disease hypertensive arteriopathy (arteriolosclerosis), which affects deep perforating vessels, and cerebral amyloid angiopathy (CAA), which affects superficial cortical and leptomeningeal vessels. Thus, while hypertension is the strongest risk factor for deep ICH, a substantial proportion of lobar ICH is due to CAA. CAA has a high recurrence risk (7.4% per year) in a pooled analysis of cohort studies63 so has caused the strongest concerns regarding statin use. Observational and randomised data suggest that recurrent ICH can be reduced by antihypertensive therapy64; however, CAA currently lacks any specific preventative therapy. A retrospective analysis found that statins in patients with ICH were associated with microbleeds on MRI, particularly of cortico-subcortical distribution, commonly observed in CAA.65 Thus, although our findings are reassuring, we were unable to stratify by ICH location or presumed cause, so decisions in ICH survivors require an individualised patient assessment of indication, comorbidity and the goal of statin therapy. Unsurprisingly, among stroke physicians the use of statins in patients following ICH remains contentious. American guidelines recommend statins in patients with ICH due to insufficient data to advise restriction (class IIb; level C) while European guidelines do not address the issue.1 2 Unfortunately, the only double-blinded placebo controlled RCT of statins in patients with ICH (NCT00718328) terminated early due to poor recruitment.
Previous ischaemic stroke
In survivors of ischaemic stroke, statins were associated with substantial and significant improvements in mortality, functional outcome and ischaemic stroke, with a non-significant trend towards increased ICH. Although epidemiological data indicate a modest link between high serum low-density lipoprotein (LDL) and greater risk of ischaemic stroke, they have also pointed towards an association of low LDL and a heightened risk of ICH.66 By reducing serum cholesterol, statins may reduce the integrity of the vasculature leading to arterial necrosis and microaneurysm formation.67 A previous meta-analysis of randomised trials of statins for primary and secondary prevention of stroke demonstrated significant reductions in LDL and ischaemic stroke risk in both primary and secondary prevention, but a significant increase in ICH was identified in secondary prevention trials.68 This finding was largely based on the only dedicated secondary prevention trial of stroke, SPARCL, which identified a significant reduction in recurrent ischaemic stroke but with a higher incidence of ICH.59 Similarly in the HPS trial previous stroke subgroup, there was a 91% increased risk in haemorrhagic stroke with statins.7 We found that when these trials are combined with observational studies and limited to secondary prevention, this ICH risk persists, although non-significantly.
Nevertheless, given the potentially increased risk of ICH with statin treatment, physicians should have caution in recommending statins to individuals with risk factors for ICH. Indeed, we found substantial heterogeneity in treatment effect indicating a ‘one size fits all’ approach to statins may be inappropriate. For example, while the effectiveness of statin therapy in patients with previous ischaemic stroke due to atherosclerotic disease is clear, in those due to atrial fibrillation (AF) the evidence is less obvious. Indeed patients with stroke and AF, who were excluded from SPARCL, often have higher bleeding risks due to concomitant anticoagulation.52 Another important concomitant therapy to consider is thrombolysis, which further adds to the haemorrhagic transformation risk.4 5 The results of our sensitivity analysis confirmed that statins increased the risk of ICH in patients with ischaemic stroke treated with thrombolysis. Age is another important component of bleeding risk. Unfortunately numerous statin trials excluded frail elders casting doubt on how results might translate to those over 80 years old. Only with careful patient selection can an optimal balance between efficacy and safety be achieved.
If statins are considered in stroke survivors, then further contentious questions arise, including: (1) which statin; (2) what dose; (3) when to initiate; (4) and when to withdraw. With regard to agent and dose, the ongoing Treat Stroke to Target trial (NCT01252875) will provide clarity on targeted LDL levels and vascular events among survivors of ischaemic stroke. Regarding timing, surrogate marker studies indicate a role of statins in the acute phase of ischaemic stroke through upregulation of nitric oxide, fibrinolytic and antithrombotic mechanisms; however, the major statin trials typically did not enrol patients until ~3 months after stroke.52 69 The only randomised trial to investigate timing per se demonstrated no improvement in neurological function at 90 days with early (<24 hours) versus delayed (7 days) therapy, although included patients had low stroke severity who may not have substantial disease substrate to benefit.70
As statins are often not prescribed until clinicians detect presence of cardiovascular disease risk factors, treatment with statins is likely to be influenced by the probability of ICH, creating ‘confounding by indication’. We have demonstrated differences in baseline characteristics between patients in statin and control groups in observational studies and exposed their impact on ICH through metaregression analysis. These differences may partly explain the conflicting results between randomised and observational studies,21 45 a problem not exclusive to stroke trials.71
Taking all studies into account, despite prescription biases the net effect of statin use appears clearly beneficial for mortality and functional outcome, even though an increased risk of ICH may partly offset these improvements. Our findings thus suggest that statins should continue to be considered in those with a previous stroke (including ICH) to reduce mortality and improve functional outcome, but caution should be taken in individuals at high risk for ICH (eg, older anticoagulated patients with poorly controlled hypertension or CAA). In these patients alternative approaches to manage hyperlipidaemia should be considered, for instance through upregulation of LDL receptors using the novel PCSK9 inhibitors.72
Limitations
Our review is based on published data of independent studies, performed in accordance with explicit, reproducible methodology. While meta-analysis of individual patient data is ideal, it is unrealistic with such large data groupings across a wide number of studies. We recognise a number of drawbacks of our study. First, there is a deficiency in sample sizes from both randomised and observational studies to generate adequately powered pooled effect estimates especially in the previous ICH cohort. There were insufficient data to perform meta-analysis of statin dose, statin type or the impact of location of ICH (lobar vs deep). Second, definitions of ICH and ischaemic stroke between studies differed with potential for miscategorisation. Although some studies precisely reported the stroke aetiology, type and severity, many did not. Third, due to expected disparities in study designs and populations, we prespecified a random effects model. Indeed, we noted substantial heterogeneity in treatment effect for many of the assessed outcomes. However, most of the heterogeneity was caused by the effect magnitude instead of the effect direction. Finally, although no signal of publication bias was identified, statistical assessments can be misrepresentative particularly with considerable heterogeneity.73
Conclusion
In patients with ICH, statins did not increase recurrent ICH. In survivors of ischaemic stroke, although statins substantially and significantly reduced recurrent ischaemic stroke, there was a non-significant increase in ICH. Nonetheless, statins show clear benefits in reducing mortality and improving functional outcome irrespective of stroke subtype. These results were predominantly based on observational data with insufficient randomised trial data available. Given that observational data are subject to inherent confounding, future randomised trials of statins in patients with cerebrovascular disease (especially ICH survivors) are required to clarify the safety of this therapy on future ICH risk.
Acknowledgments
We thank Kate Brunskill, Deputy Librarian at the Queens Square Library, UCL Institute of Neurology, for her expertise and guidance in finalising the search strategy.
References
Footnotes
Contributor OJZ developed the eligibility criteria, performed the primary literature search, contributed to data extraction and drafting of the manuscript. GB contributed to data extraction and critical revision of the manuscript. GA contributed to statistical analysis and critical revision of the manuscript. DJW designed the study concept, led the study group and critically revised the manuscript.
Funding This work was undertaken at the University College London Hospitals NHS Foundation Trust/University College London who received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centres funding scheme. OJZis funded by the National Institute of Health Research UK. GBreceived research support from the Rosetrees Trust. DJW receives research funding support from the British Heart Foundation and the Stroke Association (TSA BHF 2009/01; TSA PPA 2015/04; BHF CS/17/6/33361).
Competing interests OJZ, GB and GA have no relevant conflicts. DJW was UK chief investigator for A9951024 (Pfizer) and has received consultancy and lecture fees from Bayer.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.