Article Text

Abstract
OBJECTIVES To determine whether interference between postural control and mental task performance in patients with balance system impairment and healthy subjects is due to general capacity limitations, motor control interference, competition for spatial processing resources, or a combination of these.
METHOD Postural stability was assessed in 48 patients with vestibular disorder and 24 healthy controls while they were standing with eyes closed on (a) a stable and (b) a moving platform. Mental task performance was measured by accuracy and reaction time on mental tasks, comprising high and low load, spatial and non-spatial tasks. Interference between balancing and performing mental tasks was assessed by comparing baseline (single task) levels of sway and mental task performance with levels while concurrently balancing and carrying out mental tasks.
RESULTS As the balancing task increased in difficulty, reaction times on both low load mental tasks grew progressively longer and accuracy on both high load tasks declined in patients and controls. Postural sway was essentially unaffected by mental activity in patients and controls.
CONCLUSIONS It is unlikely that dual task interference between balancing and mental activity is due to competition for spatial processing resources, as levels of interference were similar in patients with vestibular disorder and healthy controls, and were also similar for spatial and non-spatial tasks. Moreover, the finding that accuracy declined on the high load tasks when balancing cannot be attributed to motor control interference, as no motor control processing is involved in maintaining accuracy of responses. Therefore, interference between mental activity and postural control can be attributed principally to general capacity limitations, and is hence proportional to the attentional demands of both tasks.
- posture
- attention
- vestibular
Statistics from Altmetric.com
Evidence that postural control demands attention under certain circumstances has been provided by recent studies showing dual task interference between the activity of maintaining balance and the performance of mental tasks—that is, postural stability, mental task performance, or both deteriorate when subjects are required to simultaneously balance and carry out mental tasks.1-9 Further research is necessary to clarify the attentional processes involved in postural control, and to identify which patients are susceptible to attention related instability, and which activities are likely to cause difficulties.
Dual task interference may occur if finite general attentional capacity limits are exceeded.10 This could occur if attentional capacity limits are reduced (for example, by aging or brain damage), or if postural control demands more attention because balancing is difficult, whether because of balance system impairment or because the balance task is difficult.4 11 Older adults are particularly susceptible to dual task interference,6 8but it is not known whether this is due to their relatively poor balance or their relatively impaired attentional processing. However, preliminary evidence that instability can reduce spare attentional capacity in those with no central impairment is provided by studies showing decrement in mental task performance in young, healthy subjects performing difficult balancing tasks.1 3 4
An alternative explanation for dual task interference is that concurrent tasks may compete for specific processing resources.12 Interference between postural control and performance of mental tasks could be due to the competing motor control requirements of maintaining balance and producing a response. For example, a recent study of healthy subjects13 found that simply repeating a number aloud resulted in greater decrement in postural control than did silently performing difficult arithmetical calculations. Another form of specific resource competition could occur at the stage of sensory processing.14 If this is the case, then the greatest interference would be seen with mental tasks which make demands on spatial processing resources, as the use of sensory feedback for postural control involves processing of spatial information. Support for this hypothesis is provided by studies which have found greater interference from balancing on spatial than non-spatial tasks both in healthy young and older adults.3 6 15 In addition, patients with impaired sensory processing, such as those with vestibular disorder, might be especially vulnerable.
Patients with peripheral vestibular disorder have intact attentional processing but often exhibit increased postural instability. Moreover, dizzy patients often complain of difficulty concentrating, clumsiness, and fatigue16—symptoms which could indicate mental exhaustion or overload. In a previous study of dizzy patients at a neuro-otology clinic,1 performance of patients and healthy controls on a spatial mental task deteriorated to a similar extent when balancing on a moving platform. However, the failure to find any difference in performance between patients and controls may have been due to the relative insensitivity of the measure of mental performance, the heterogeneity of the patient sample, and the difficulty of the balance task (which was challenging even to healthy subjects). In a small series of vestibular patients,17 using reaction time as a measure of mental task performance, greater dual task interference was found in patients than in healthy controls.
The present study investigated dual task performance on non-verbal reaction time tasks in patients with vestibular disorder and healthy controls. By comparing the pattern of decrement on spatial and non-spatial tasks with low and high attentional load, under easy and difficult balancing conditions, we sought to determine whether interference between postural control and mental task performance in patients with balance system impairment and healthy subjects is due to general capacity limitations, motor control interference, competition for spatial processing resources, or a mixture of these.
Methods
SUBJECTS
A total of 48 patients and 24 healthy controls participated. The patients were 16 males and 32 females with a mean age of 46.65 years (SD 13.87), who were attending the specialist neuro-otological clinic where the study was conducted on account of a current complaint of dizziness or unsteadiness. Vestibular disorder was established in all patients on the basis of clinical history, examination, and neuro-otological testing, which comprised audiogram, caloric, and positional tests, with (as necessary) auditory evoked responses, electronystagmographic recording of saccades, pursuit, and optokinetic and rotatory nystagmus, computed dynamic posturography, and other specialist tests. Because this study was conducted in a tertiary referral clinic, all patients had complaints of at least several months' duration, typically associated with poor compensation. Twenty five patients had peripheral vestibular imbalance (uncompensated vestibular neuronitis, middle ear disease, idiopathic bilateral vestibular failure, labyrinthine concussion, benign paroxysmal positional vertigo, and diffuse vascular disease), 10 patients had evidence of peripheral vestibular imbalance but also central disorders (migraine, head injury, previous brain stem dysfunction, ischaemia, Sjogren's syndrome), six patients had a central diagnosis (migraine, Behçet's disease, lateral medullary syndrome, ischaemia), and in the remaining seven patients a precise diagnosis could not be confirmed.
The controls were 11 males and 13 females with a mean age of 44.25 years (SD 15.03), who had no medical history of dysfunction of the balance system and no current complaint of dizziness or unsteadiness.
DESIGN AND MEASURES
Postural control
Postural stability was assessed under two conditions: (a) standing with eyes closed on a stable platform; (b) standing with eyes closed on a destabilised, “sway referenced” platform. During sway referencing, continuous measurements of the spontaneous postural sway of the subject are used to trigger an equivalent motion of the platform on which the subject is standing. Thus when subjects sway backwards or forwards the platform on which they are standing tilts synchronously with them. Consequently, subjects are deprived of the proprioceptive feedback which is normally derived from changes in the angle of the ankle during sway motion, and (with eyes closed) must rely chiefly on the vestibular system for information about self motion and orientation.
Postural stability was assessed by computerised dynamic posturography,18 using the “equilibrium score”, which is calculated from the maximum amplitude of sway in the anterior-posterior direction during one 20 second trial, expressed as a percentage, with 100% representing perfect stability. Mean velocity of movement of the centre of pressure and root mean square (RMS) amplitude displacement of the centre of pressure from its mean position (in two dimensions) were also calculated from the raw data, for the 51 participants who did not fall on any trial.
Mental tasks
The mental tasks were designed to permit comparison of (a) “low load” tasks with “high load” tasks (these tasks differed in terms of the total attentional resources required); (b) “spatial” tasks with “non-spatial” tasks (these tasks differed in the extent to which specific spatial processing resources were required).
The low load tasks were simple speeded auditory discrimination tasks. In the spatial version, subjects pressed the upper button on a hand held pad if a tone was presented to their left ear, and the lower button if a tone was presented to their right ear. In the non-spatial version, subjects pressed the lower button if a tone was presented bilaterally, and the upper button if a buzz was presented bilaterally.
The high load tasks required a more complex categorisation of a numerical stimulus. In both conditions the stimulus consisted of auditory bilateral presentation of two numbers equivalent to a time on a digital clock (for example, 10 42). In the spatial condition the subject was required to press the upper response button if the two numbers represented a time at which both hands of an analogue clock would be on the same side of the clock face, and the lower if they would not. For the non-spatial condition subjects pressed the upper button if the two numbers were both either even or odd numbers, and the lower button if they were not.
There were two measures of mental task performance: firstly, the number of correct responses under each condition; secondly, reaction time, expressed as the time (ms) between presentation of the stimulus and the moment when the subject pressed the response button.
Equipment and procedure
Ethical approval was obtained from the relevant hospital and university ethics committees and subjects gave informed consent before participation. Subjects were required to abstain from taking antivertiginous or psychoactive medication for 48 hours before testing, and were advised to eat and drink little on the day of testing.
Postural sway was measured using the EquiTestTMsystem.18 During each mental task trial, eight auditory stimuli were presented through headphones. Stimuli were controlled and responses recorded by a personal computer, which was connected to the headphones and response box. Subjects held the response box at about their midline, and positioned their right thumb on the “higher” response button (more distal from their bodies) and their left thumb on the “lower” button (more proximal to them). An arbitrary stimulus-response mapping was utilised whereby responses to lateralised tones were made on vertically aligned buttons, so as to prevent automatic processing of the spatial relation between stimulus and response.
For the low load mental tasks, subjects were required to make accurate and rapid discrimination responses to stimuli of 500 ms duration, consisting of either a 1000 Hz pure tone or narrow band noise centred on 1000 Hz (the buzz). For the high load tasks subjects were required to make accurate and rapid button press responses to numerical stimuli presented bilaterally. The stimuli are described under mental tasks above; the numbers 6, 12, 00, and 60 were excluded because they could not be classified spatially, and the numbers 01 to 09 were excluded owing to the lower level of processing demands associated with single digits. No subject received the same stimulus twice. For both tasks the interval between a response (or the termination of an opportunity to respond) and the next stimulus was 1000 ms. A failure to respond was coded for any stimulus for which no response occurred within 3000 ms of stimulus onset, and incorrect responses resulted in auditory presentation of the word “wrong”.
There were two trials under each condition, resulting in a total of 28 trials as follows:
(a) Four baseline trials of postural sway (with no mental task); two on a stable platform, and two with the platform destabilised.
(b) Eight baseline trials of the mental tasks (while sitting down), comprising four high load and four low load trials, of which two involved spatial and two non-spatial tasks.
(c) Sixteen dual task trials, comprising the eight mental task trials while standing on the stable platform, and eight when standing on the destabilised platform.
To minimise order effects the order of the postural and mental task conditions was counterbalanced across subjects, a minimum of one single task baseline balancing trial was discarded as a practice trial, and subjects were permitted to sit between trials if they felt fatigued.
STATISTICAL ANALYSIS
Repeated measures analysis of variance (ANOVA) was used to determine the effects of balance on reaction time and accuracy, and the effects of the mental tasks on balance. As 18 patients were unable to complete the trials on the destabilised platform, all analyses were carried out twice; once with the data from all subjects for the sitting and standing on stable platform trials only (omitting the destabilised platform trials), and once using data from the subset of subjects who also completed the destabilised platform trials (including all the trials). Any differences in the results of the two analyses are highlighted below. Owing to temporary technical problems, postural sway data are missing for two control subjects, the baseline standing data are missing for one patient, and the accuracy data for one test condition are missing for one patient. Velocity and RMS data were log transformed before analysis to eliminate between subject differences in variability.
Results
EFFECT OF BALANCING ON MENTAL TASK PERFORMANCE
Low load tasks
Responses on the low load tasks were extremely accurate in all trials (table 1); inaccurate responses were not sufficiently numerous to permit reliable statistical analysis.
Mean (SD) distribution of correct responses on low and high load tasks, under each postural control condition. The maximum number of correct responses possible was 16
The effects of standing and destabilisation on reaction times for those subjects completing all trials are shown in figure 1. There was a significant effect of balancing condition (sittingv standing vdestabilised: F(2,106)=6.16, p=0.003), task type (spatial v non-spatial:F(1,53)=89.06, p<0.001), and subject group (patient v control:F(1,53)=6.80, p=0.012), but no interactions. Figure 1 shows that the controls responded more quickly than patients, that both patients and controls responded more quickly to the spatial task than the non-spatial stimuli, and that both groups responded more slowly when standing than when sitting, particularly when destabilised. A similar pattern of results was found for the data for all subjects, omitting the destabilised trials; there were significant main effects of task type (F(1,70)=96.26, p<0.001) and subject group (F(1,70)=8.10, p=0.006), but without the destabilised condition the effect of balancing condition did not quite reach significance (F(1,70)=3.03, p=0.086).
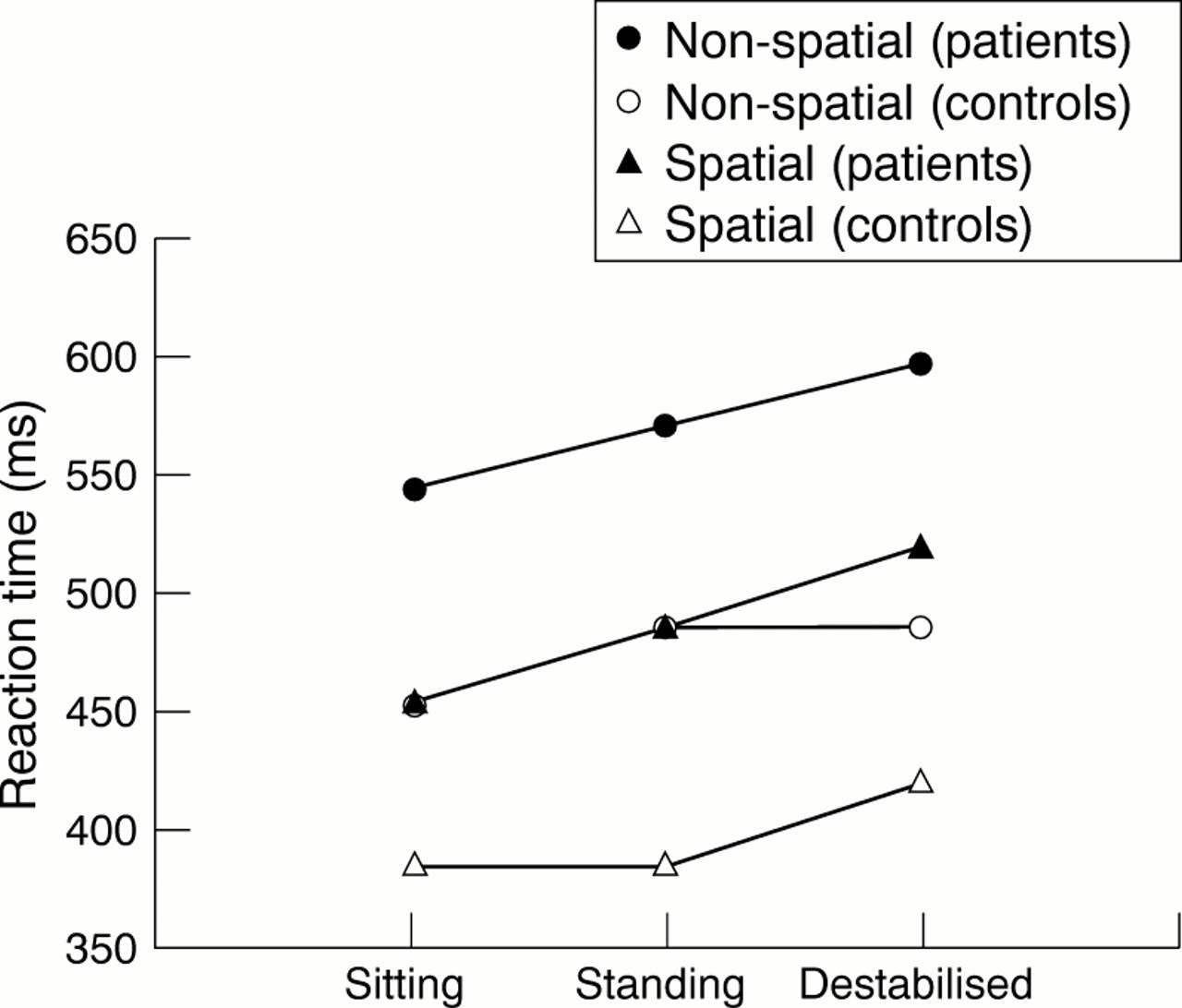
Mean reaction times of patients and controls on the low load mental tasks.
High load tasks
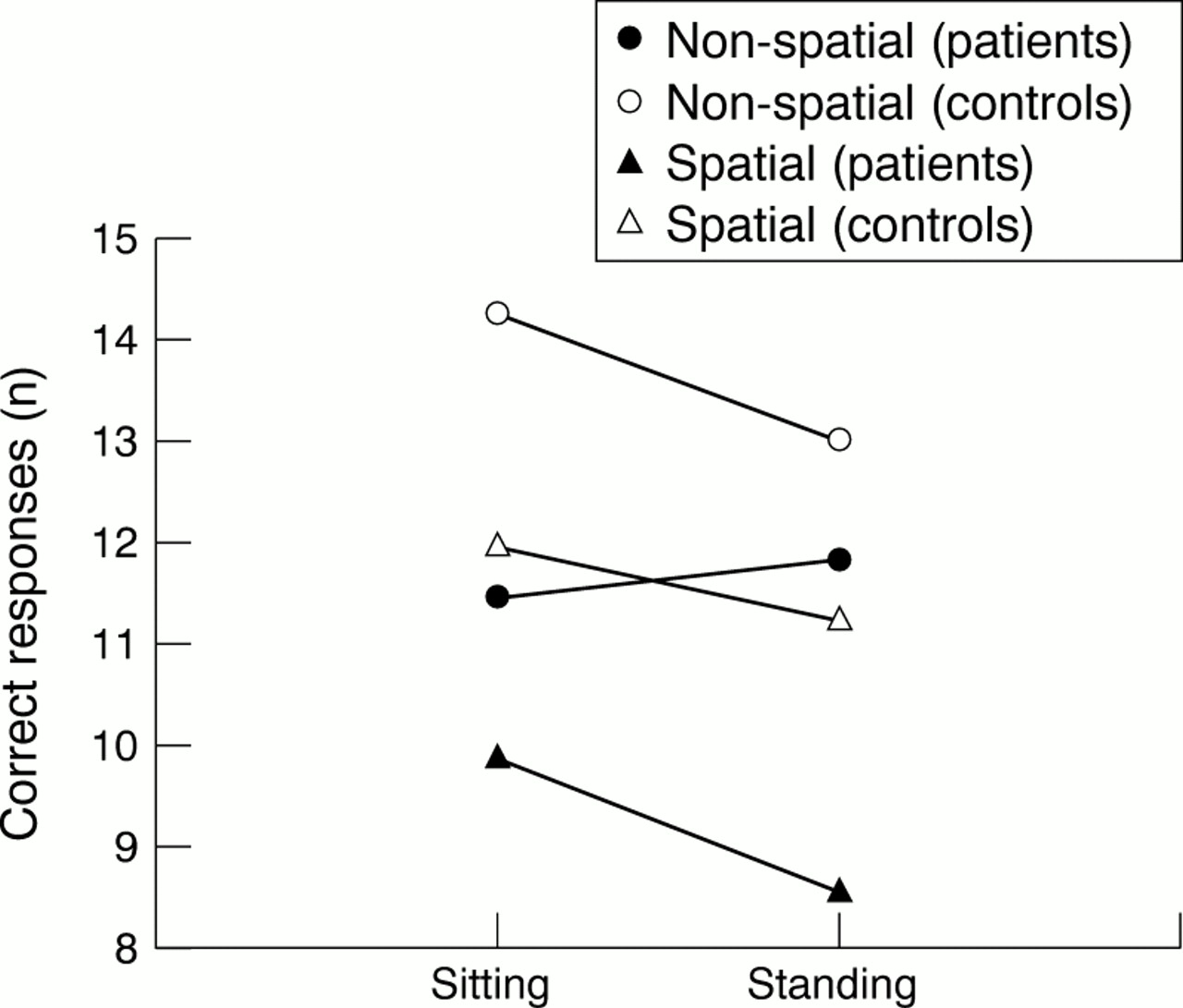
Responses on the high load tasks varied greatly in accuracy (table1), and so accuracy could be employed as a measure of high load task performance. The effects of balancing on accuracy for all subjects on the sitting and standing trials are shown in figure 2. There was a significant effect of balancing (F(1,69)=6.52, p=0.013), task type (F(1,69)=62.16, p<0.001), and subject group (F(1,69)=12.69, p<0.001). There was also a three way interaction between subject group, task type, and balancing (F(1,69)=5.42, p=0.023). Figure 2 shows that the controls were more accurate than the patients, and that both groups were more accurate on the non-spatial than the spatial task. However, whereas the controls' performance declined when standing to a similar extent on the spatial and non-spatial tasks, the patients' accuracy deteriorated when standing only on the spatial task. When the data for the destabilised trials were included in the analysis, the same pattern of main effects, and more importantly the three way interaction (F(2,102)=4.39, p=0.015), was seen.
{kind=link}
{kind=link}
Mean number of correct responses on the high load mental tasks in patients and controls (sitting and standing conditions only).
Table 2 shows the effects of balancing on reaction times on the high load tasks, for those subjects completing all trials. The only significant main effect reflected the longer reaction times on the spatial compared with the non-spatial task (F(1,51)=35.73, p<0.001), and there were no interactions. The same pattern of results was found in the data from all subjects, omitting the destabilisation trials.
Mean (SD) reaction time (ms) of patients and controls on high load mental tasks under each postural control condition
EFFECT OF MENTAL TASKS ON SWAY
As expected, patients had significantly lower equilibrium scores than controls both when standing on the stable platform (F(1,67)=4.69, p=0.03) and on the destabilised platform (F(1,49)=5.45, p=0.02). There was a significant main effect of the mental tasks on equilibrium scores when standing on the stable platform (F(2,134)=5.96, p=0.007). Unexpectedly, this was due to an increase in scores when performing mental tasks (table3), but this isolated finding was not corroborated by any significant effect of mental tasks on velocity (F(2,98)=0.23, p>0.1) or RMS (F(2,98)=0.06, p>0.1). When standing on the destabilised platform there was no significant effect of mental tasks on equilibrium scores (F(2,98)=1.11, p>0.1), nor on velocity or RMS.
Mean (SD) postural sway at baseline and when performing low and high low load mental tasks
Discussion
As the balancing task increased in difficulty, reaction times on a low load mental task grew progressively longer. Although our task employed a manual response, the pattern of findings was very similar to that obtained previously with a verbal response.4 These results could be interpreted as an indication of either motor control interference or limitations in general attentional capacity. However, the finding that accuracy also declined on the high load task when balancing cannot be attributed to motor control interference, as no processing of motor control is involved in maintaining accuracy of responses, and hence provides evidence for decrement due to general capacity limitations.
The lowest accuracy levels were seen in patients with vestibular disorders when performing the high load spatial task while balancing. This significant interaction between patient group and task type might be taken as evidence for interference at the level of spatial processing. However, accuracy in the control group also declined significantly on the non-spatial task when balancing, which again suggests that decrease in accuracy is more likely to have been due to general capacity limitations than specific interference with spatial processing.
Performance of the mental tasks did not consistently induce additional instability in either patients or controls. The absence of any increase is consistent with many previous studies, which have found dual task decrement only on the mental task rather than also affecting balance, presumably because balancing is usually prioritised when unstable.3-5 Those studies which have found effects of mental tasks on postural control may have been able to persuade participants to devote attention to the mental task even if this led to instability—for example, by permitting a relatively stable stance.6 Moreover, most studies which have found an effect of mental tasks on sway employed verbal responses,2 5-7which may involve respiratory perturbation of posture,13or tested postural control with the eyes open.6 7 As many mental tasks (including spatial and numerical tasks) are facilitated by mental imagery and involve covert visuospatial attention or even overt eye movement,19 20 it seems plausible that such tasks may interfere with visual control of posture, resulting in an increase in sway with eyes open but not with eyes closed.
The results of this study may have been influenced by methodological limitations. A minority of patients were unable to undergo testing on the moving platform. Although results on the stable and destabilised platform did not differ, this could have been because of selective drop out of those patients who would have been most destabilised by dual task interference, which might have masked a difference between patients and controls. Moreover, the patient population was limited to cases of chronic, mild, partially compensated vestibular disturbance. Disruption of central spatial processing after vestibular nerve section has been shown to return to normal within a month of surgery,21 which suggests that greater dual task interference, or disruption of spatial processing,or both might be found in patients with acute, severe vestibular imbalance. In addition, baseline mental task performance differed in patients and controls (although the pattern of dual task effects seemed to be essentially independent of baseline task performance), and both patients and controls apparently maximised reaction times on the high load mental task by sacrificing accuracy, thus rendering comparison of response times on the low and high load tasks meaningless.
To summarise, levels of dual task interference between balancing and mental activity are similar in patients with vestibular disorder and healthy controls, and can be attributed principally to general capacity limitations, albeit possibly supplemented by a degree of motor control and spatial processing interference. The clinical implications are that those most vulnerable to interference between mental activity and postural control will be patients with central processing deficits, such as older people and those with brain damage—a conclusion which is supported by evidence for strong dual task effects in these patient populations.5-9 Finally, it seems that the degree of interference between postural control and mental activity is proportional to the difficulty (attentional demands) of the mental and balancing tasks undertaken, and is less influenced by the extent to which the task and response require specific spatial processing resources.
Acknowledgments
This research was supported by grant number 048013 from the Wellcome Trust. We are grateful to Sarah Crawford for assistance with testing patients and controls.