Article Text

Abstract
OBJECTIVES The present study aimed at the analysis of release patterns of neurobiochemical markers of brain damage (neuron specific enolase (NSE) and protein S-100B) in patients with traumatic brain injury and their predictive value with respect to the short and long term neuropsychological outcome.
METHODS Serial NSE and S-100B concentrations were analysed in blood samples taken at the first, second, and third day after traumatic brain injury. In 69 patients who fulfilled the inclusion criteria (no history of neurological or psychiatric disorder or alcohol or drug dependency, blood sampling according to the scheduled time scale, aged between 16 and 65 years) standardised neurological examinations and qualitative and quantitative evaluation of CT were performed. Comprehensive neuropsychological assessment was performed in 39 subjects 2 weeks after admission and in 29 subjects at a 6 month follow up examination.
RESULTS Most patients presented with minor head injuries (GCS⩾13) at the time of admission. Six months later most patients were fully independent in activities of daily living. Two thirds of the patients, however, still had neuropsychological dysfunction. Patients with short and long term neuropsychological disorders had significantly higher NSE and S-100B serum concentrations and a significantly longer lasting release of both markers. A comparative analysis of the predictive value of clinical, neuroradiological, and biochemical data showed initial S-100B values above 140 ng/l to have the highest predictive power.
CONCLUSIONS The analysis of post-traumatic release patterns of neurobiochemical markers of brain damage might help to identify patients with traumatic brain injury who run a risk of long term neuropsychological dysfunction.
- traumatic brain injury
- neuron-specific enolase
- protein S-100B
- neuropsychology
- outcome
Statistics from Altmetric.com
Traumatic brain injury is one of the major causes of persisting neurobehavioural disorders1 and even in minor head injuries—generally associated with good outcome—a substantial number of patients complain about long term neuropsychological deficits or postconcussional symptoms.2 Much effort has been made to evaluate the recovery potential at an early stage after traumatic brain injury and to identify patients under risk of developing long term neurobehavioural disorders. Especially in mild to moderate head injury there is only a weak association between clinical neurological signs and intracranial abnormalities in CT and subtle long term neurobehavioural disorders.3 During the past decade neurobiochemical markers of brain damage have gained increasing interest both in experimental4 and clinical5neurotraumatology. Whereas structural proteins of astroglial (glial fibrillary acidic protein) or neuronal (neurofilament protein) brain tissue were mostly used in experimental settings, neuron specific enolase (NSE) and protein S-100B were those markers which—due to commercial availability and detectability in serum samples—have attained growing attraction in clinical research. The cytoplasmatic enzyme NSE is predominantly found in the cytoplasm of neurons and in cells with neuroendocrine differentiation.6 Increased concentrations of NSE can be measured in CSF and in peripheral blood after neuronal damage. Protein S-100B forms part of a family of diverse Ca2+ binding proteins, the cellular synthesis of which has predominantly been localised in astroglial and Schwann cells.7 8
Recent studies showed an association between clinical outcome and CSF or serum concentrations of protein S-100B and NSE in patients with severe traumatic brain injury.9-11 Raabeet al 12 showed that excessive secondary increase in S-100B serum concentration relates to severe brain damage associated with a fatal outcome. The same group reported a significant correlation between early S-100B values and the volume of cerebral contusions in patients with severe traumatic brain injury but no association between NSE concentration and the size of contusions whereas Skogseid et al 9 found a significant correlation between maximum NSE concentrations and contusion volume. On the other hand, Woertgen et al 11 reported neither NSE nor S-100B to be associated with the severity of intracranial pathology as defined by the Traumatic Coma Data Bank (TCDB) CT classification13 in patients with severe traumatic brain injury. Recent studies by Ingebrigtsen et al gave evidence that early protein S-100B serum concentrations provide information on diffuse brain damage14 and seem to be associated with neuropsychological outcome2 even in minor head injury.
In previous studies we showed that the severity of traumatic brain injury is associated with the early post-traumatic release of protein S-100B and NSE15 and that the early kinetics of neurobiochemical markers of brain damage after traumatic brain injury do reflect a different type of intracranial pathology as demonstrated in cranial CT.16 The aim of the present study was (1) to analyze the association between release patterns of NSE and S-100B and the short and long term neuropsychological outcome after traumatic brain injury and (2) to compare the predictive value of neurobiochemical markers of brain damage, focal neurological deficits, and intracranial pathology as demonstrated in serial CT imaging with respect to the short and long term neuropsychological outcome.
Methods and patients
METHODS
Neurobiochemical assessment
Venous blood samples were taken at the first (median: 27 hours after trauma), second (median: 49.5 hours), and third (median: 80.0 hours) day after admission to the Department of Neurosurgery. Blood was allowed to clot and were centrifuged (1000 rpm for 10 minutes) within 30 minutes after sampling. Serum was frozen at −78°C and stored for later analysis. Protein S-100B and NSE were analyzed using immunoluminometric assays (Sangtec 100). This assay measures the β subunit of protein S-100 as defined by three monoclonal antibodies (SMST 12, SMSK 25, and SMSK 28). The detection limit of the kit is 0.020 μg/l and S-100B serum values range below 0.120 μg/l in 95% of healthy subjects. Analysis of NSE is based on monoclonal antibodies which bind to the γ subunit of the enzyme. The sensitivity of the assay is reported to be below 1.0 μg/l and the upper limit of the reference range is 12.5 μg/l in 95% of healthy subjects. All biochemical analyses were performed on a fully automated LIA-mat System 300 by a member of our study group who was blind to clinical and neuroradiological data of the patients.
Neuroradiological assessment
In all patients cranial CT was obtained at admission and at several follow up examinations depending on the clinical course. Brain CT evaluation was based on planar and volumetric measurements using the public domain NIH image program (developed at the US National Institutes of Health and available on the Internet athttp://rsb.info.nih.gov/nih-image/). All scans were evaluated by an experienced and trained neuroradiologist (SJ) who was blind to the clinical and neurobiochemical data. Evaluation of CT followed the criteria given by Gentry et al 17 and included haemorrhagic and non-haemorrhagic intra-axial lesions, extra-axial haematomas, diffuse haemorrhage, and signs of intracranial pressure (displacement of midline structures, compressed cisterns, sulcal effacement). Additionally, all CT was analyzed according to the TCDB classification scheme.13
Neurological assessment
Standardised neurological examination was performed on admission, on the 4th day after admission, and 14 days later. Glasgow coma scale (GCS18) scores were obtained at the site of accident, during the first 3 days after admission, and 10 days after traumatic brain injury.
Neuropsychological assessment
Neuropsychological assessment 2 weeks and 6 months after head injury was based on tests covering the following cognitive domains:
(1) Global cognitive and behavioural screening (neurobehavioural rating scale (NBRS19), mini mental state examination (MMSE20), frontal lobe score (FLS21)
(2) Memory/learning (digit and visual spans,22 selective reminding23)
(3)Language (token test24)
(4) Visuoperception/construction (block design25)
(5) Executive functions (semantic26 and phonological fluency,27 distractibility, and interference (Stroop test28), concept formation29)
(6) Attentional performance (computerised test battery for attentional performance (TAP,30 subtests “alertness” and “go-no go”)
(7) Psychomotor speed (finger tapping31).
Patients were classified as presenting neuropsychological disorders if they performed less than 1 SD below (age adjusted) normal data in at least three cognitive domains.
STATISTICAL ANALYSIS
Due to small sample sizes and ordinal scaled data statistical analysis was mainly performed with non-parametric procedures (χ2-Fisher's exact tests, Mann-WhitneyU tests, Spearman's rank correlation coefficients). All levels of significance reported in the result section are two tailed. Receiver operating characteristic (ROC) curve analyses were used to identify the positive likelihood ratio of post-traumatic NSE and S-100B serum concentrations with respect to the neuropsychological outcome.
The study was approved by the local ethics committee and informed and written consent was obtained by all patients.
PATIENTS
From a consecutive series of patients admitted to the Department of Neurosurgery after traumatic brain injury we included all patients into the study who fulfilled the following selection criteria:
(1) No history of neurological or psychiatric disorder or alcohol or drug dependency
(2) Age between 16 and 65 years
(3) Blood sampling according to the scheduled time scale
(4) Informed and written consent to participate in the study.
During an 18 month study period 69 patients fulfilled the selection criteria. From this group 39 patients were able and agreed to perform a comprehensive neuropsychological examination 2 weeks after head injury and 29 patients could be reevaluated 6 months later. Main reasons for drop out were early transfer to other clinics, missing or haemolytic blood samples, missing informed and written consent, or severe disorders of attention which prevented patients from completing a comprehensive neuropsychological examination 2 weeks after injury. Table 1 shows the sociodemographic, clinical, and neuroradiological data of all patients. Scores on the GCS at the time of admission showed a bimodal distribution with either severe (GCS⩽8, 31 patients) or mild head injury (GCS ⩾13, 32 patients). Patients with neuropsychological assessment represent a subgroup of patients with minor head injury (median GCS score at the site of accident=15) when compared with patients who were not able to complete a neuropsychological assessment 2 weeks after traumatic brain injury (median GCS score=6; Mann-Whitney U test: z=−2.4, p=0.016). The patient group with neuropsychological follow up examination did not differ significantly from the patients examined 2 weeks after traumatic brain injury for sex, age, initial GCS score, type of intracranial pathology, or post-traumatic S-100B or NSE release. According to the TCDB classification criteria1336 patients showed diffuse injury I (no visible intracranial pathological change), 17 patients diffuse injury II (cisterns were present with shift 0 to 5 mm and/or lesion densities present but no high or mixed density lesion>25 ml), six patients diffuse injury IV (cisterns compressed or absent with shift>5 mm; no high or mixed density lesion>25 ml) and 10 patients showed a non-evacuated mass lesion in serial CT.
Sociodemographic, clinical, and neuroradiological data
Results
NEUROBIOCHEMICAL MARKERS AND SEVERITY OF TRAUMATIC BRAIN INJURY
We found numerically high and significant intercorrelations between NSE and S-100B serum concentrations both at and between the sampling points (all p<0.0001). Both protein S-100B and NSE were highly and significantly correlated with GCS scores. The numerically highest correlations were found between S-100B concentrations and GCS scores at the first (r=0.57, p<0.0001) and NSE concentrations and GCS scores at the second day (r=0.74, p<0.0001). Figure 1 shows the release patterns of S-100B ) and NSE of all patients clustered into 24 hour intervals after TBI. There was a significant decrease of both S-100B (Friedman two way ANOVA: χ2= 30.3, df=2, p<0.0001) and NSE (χ2=36.6, df=2, p<0.0001) post-traumatic serum concentrations. We did not find significant differences in S-100B or NSE concentrations between patients with and without focal neurological deficits. Subjects with signs of intracranial pathology exhibited numerically higher S-100B and NSE concentrations, statistical significance was only reached for S-100B values at the second (Mann-Whitney Utest: z=−2.2, p=0.030) and third day (z=−2.6, p=0.010). To consider release patterns and kinetics of both proteins we calculated the area under curve values (AUCs) adjusted for the exact time interval between sampling points. Patients with moderate to severe head injury (GCS<13) exhibited significantly higher AUC values when compared with patients with mild head injury (GCS 13–15, NSEAUC:z=−3.9, p<0.001; S-100BAUC:z=−2.7, p=0.006).

Post-traumatic release patterns (means(SEM)) of protein S-100B (light bars, left axis) and NSE (dark bars, right axis) clustered into 24 hour intervals after traumatic brain injury (numbers in parentheses indicate the mean sampling time (SD)).
Neuropsychological outcome
According to the criteria defined in the method section, 74% of all patients investigated 2 weeks after traumatic brain injury showed neuropsychological dysfunction mostly marked in disorders of attentional performance (reaction times and selective attention, 88%), executive functions (planning, concept formation, fluency, increased interference susceptibility, and reduced error control, 46%-74%), and memory performance (30%). At the follow up examination 6 months after traumatic brain injury we found a significant improvement in nearly all neuropsychological test results but 69% of all patients still displayed neuropsychological disorders. The profile of deficits was the same as shown in the first examination except for significantly more memory dysfunction (50%). Only 48% of the patients in the follow up examination were in competitive, transitional, or supported work 6 months after traumatic brain injury. A median score of 126 (range 114–126) in the functional independence measure (FIM32) indicated that nearly all patients were fully independent for activities of daily living.
Neurobiochemical markers and neuropsychological outcome
Subjects with neuropsychological deficits at the first examination 2 weeks after traumatic brain injury had a significantly longer lasting and higher S-100B release (S-100BAUC: Mann-WhitneyU Test: z=−2.7, p=0.005). Serum concentrations of NSE were also higher in patients with neuropsychological deficits but this did not reach significance (z=−1.9, p=0.056). Differences were mostly marked in the first blood sample for S-100B (z=−3.1, p=0.001) and in the second blood sample for NSE (z=−2.0, p=0.050). Patients who still had neuropsychological dysfunction at the follow up examination 6 months after trauma had significantly longer lasting and higher S-100B serum concentrations compared with patients without deficits (S-100BAUC: z=−2.2, p=0.023, S-100B1: z=−2.0, p=0.040, S-100B2: z=−2.0, p=0.044). For NSE serum values we found no significant differences between patients with and without persisting neuropsychological deficits. Figure 2 shows the distribution of early S-100B values in patients with and without neuropsychological disorders at 2 weeks and 6 months after brain injury.

S-100B values in the first blood samples taken after TBI in patients with (positive) and without (negative) neuropsychological disorders at 2 weeks and 6 months after brain injury. p Values are from Mann-Whitney U tests.
Protein S-100B was found to have the highest predictive value for short and long term neuropsychological outcome after traumatic brain injury. Table 2 shows a comparison of sensitivity, specificity, and positive likelihood ratio (+LR) of protein S-100B, NSE, focal neurological deficits, and intracranial pathology in CT imaging. The +LR of patients with initial S-100B serum values above 140 ng/l was calculated as 6.9 for the first neuropsychological examination; sensitivity of this cut off value was 69% and specificity was calculated as 90%. For neuropsychological deficits 6 months after traumatic brain injury the positive likelihood ratio decreased to 5.9, sensitivity of the 140 ng/l cut off value was 65%, and specificity was 89%. The table clearly shows the high predictive value of protein S-100B release for both the early and late neuropsychological outcome.
Comparative analysis of sensitivity, specificity, and positive likelihood ratio (+LR) based on initial protein S-100B and NSE serum concentrations, clinical signs of focal neurological deficits, and signs of intracranial pathology in CT imaging
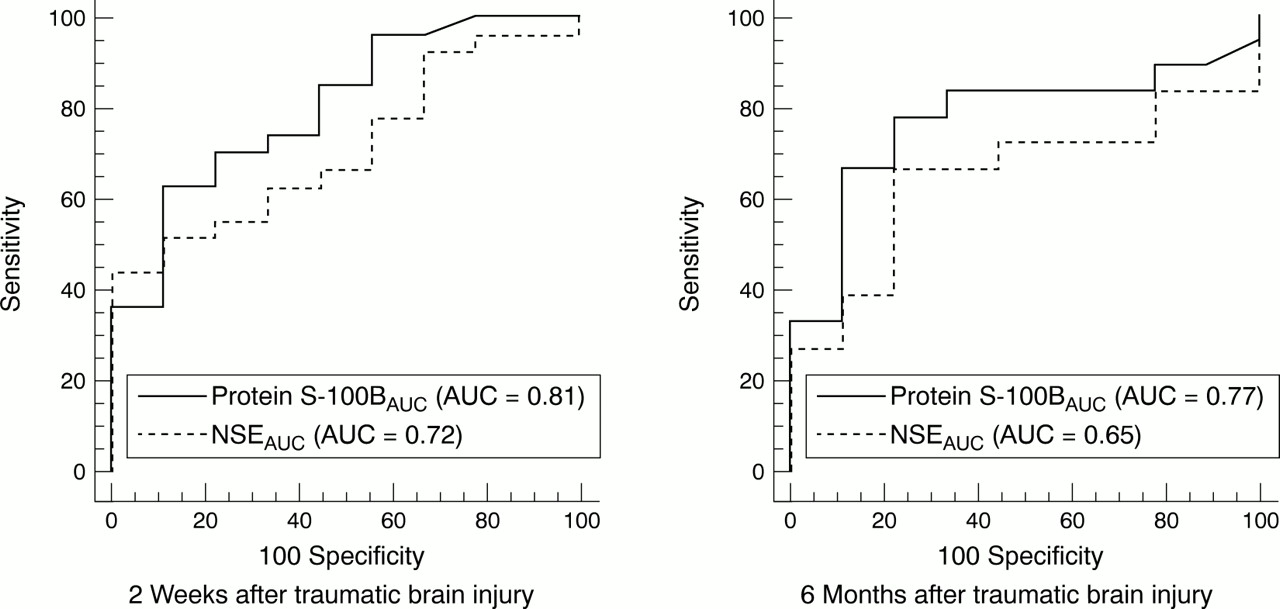
To compare the different values of protein S-100B and NSE for the prediction of neuropsychological deficits we calculated receiver operating characteristic (ROC) curves of the release (AUC) of both biochemical markers. Figure 3 shows a comparison of the ROC curves both for the 2 weeks and 6 months follow up investigation. When compared with NSE, the diagnostic potential (area under ROC curve) of protein S-100B was calculated as higher for both the 2 week (p=0.108) and 6 month (p=0.301) neuropsychological performance. The difference, however, did not reach significance.

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves of S-100B and NSE release (area under curve) for the 2 week and 6 month neuropsychological outcome.
Discussion
Post-traumatic serum concentrations of NSE and S-100B were found to be highly increased in a series of patients with traumatic brain injury. The initial rise in serum concentration was followed by a significant decrease in the course of the next 3 days. Moderate to severe brain injury was associated with a significantly higher and longer lasting release for both neuron specific and astrocyte specific biochemical markers of brain injury. From the second day after traumatic brain injury signs of intracranial pathology as shown in serial CT evaluations resulted in significantly higher S-100B values. Patients with and without signs of focal neurological deficits did not differ in release patterns of both proteins. Our data corroborate the findings of recent studies which showed that post-traumatic release of NSE9 10 and protein S-100B5 12 15 33 are useful markers of the severity of brain damage after traumatic brain injury. Differences between studies as pointed out in the introduction have to be attributed to the use of different study designs and different approaches to the analysis of biochemical markers (luminescence immunometric assay (LIA), radioimmunoassay (RIA), or enzyme linked immunosorbent (ELISA) tests), the specificity and sensitivity of which are not comparable.
The present data show that post-traumatic serum concentrations of NSE and S-100B not only reflect the overall severity of brain trauma as defined by GCS scores but also relate to subtle neuropsychological dysfunction. Neuropsychological disorders 2 weeks after onset of head trauma were associated with a significantly higher and longer lasting release of both brain proteins. Six months after traumatic brain injury the neuropsychological status of a group predominantly consisting of patients with minor head trauma was reassessed. Most of these patients were fully independent in activities of daily living and had significantly improved their neuropsychological performance. Patients with neuropsychological disorders 6 months after head trauma, however, also exhibited significantly higher NSE and S-100B serum concentrations during the first 3 days after traumatic brain injury. These results are in accordance with the findings of a Scandinavian group2 14 which showed in a small series of patients that early post-traumatic S-100B concentrations were correlated with long term neuropsychological disorders.
A comparative analysis of the predictive value of the neurological status, CT data, and NSE and S-100B serum concentrations showed the initial protein S-100B concentration to be the best predictor of long term neuropsychological disorders. In the present study, however, we only considered information derived from serial CT. Advanced MRI techniques such as quantitative MRI analysis34 35 or diffusion weighted or magnetisation transfer imaging36allow for the detection of diffuse white matter brain damage or axonal brain injury with a greater accuracy than conventional CT procedures, which probably would result in a higher predictive value. Due to general availability and rapid access in unstable and intubated patients CT imaging will remain the imaging technique used in most acute care settings for patients with traumatic brain injury and we, therefore, decided to use only information depicted from CT. The predictive value of post-traumatic protein S-100B concentration exceeded the information derived from NSE release when judged by the long term neuropsychological outcome. This finding might be attributed to the different biological function of both proteins. Protein NSE is predominantly found in the cytoplasm of neurons.6 The protein is not secreted into the extracellular fluid by intact neurons but is set free by cell destruction. Protein S-100B forms part of a large family of Ca2+ binding proteins and its cellular synthesis has been localised primarily in astrocytes.8Although the release mechanism and the intracellular function of S-100B are not definitely identified, studies on cell cultures gave increasing evidence that S-100B regulates Ca2+ dependent cellular information processing by means of different concentrations. It has been shown that overexpression of S-100B induces neuronal cell death and apoptosis in astrocyte-neuron cocultures.37 On the other hand, astrocyte S-100B expression is also upregulated during lesion induced collateral sprouting and reactive synaptogenesis.38 These data indicate that protein S-100B might have both a detrimental and beneficial role,39dependent on concentration and time elapsed since brain trauma. In a recent study16 we showed that the post-traumatic release patterns of NSE and S-100B reflect different types of pathophysiological changes after traumatic brain injury. Release patterns of S-100B and NSE differed significantly in patients with primary cortical contusions, diffuse axonal injury, and signs of cerebral oedema without space occupying lesions. These findings indicate that the kinetics of both neurobiochemical markers of brain injury may mirror complex neuronal-glial interactions. Increased S-100B concentration in peripheral blood is also considered as a marker for dysfunction of the blood-brain barrier and protein S-100B release in peripheral blood may indicate functional brain dysfunction without visible pathology in CT imaging. Protein S-100B, therefore, might have a higher predictive potential with respect to long term neurobehavioural disorders after minor traumatic brain injury compared with NSE concentrations.
In this study we focused on a patient group who was able to perform a comprehensive neuropsychological examination soon after traumatic brain injury. These patients represent only a subgroup with minor head injury. Therefore, generalisability of the present results is restricted by small sample sizes and the study needs to be replicated in larger trials. The present data, however, clearly indicate that the analysis of post-traumatic release patterns of neurobiochemical markers of brain damage might help to identify patients with traumatic brain injury who run a risk of long term neuropsychological dysfunction. It has to be evaluated whether low post-traumatic NSE or S-100B serum concentrations might lead to early discharge from hospital, thereby reducing in hospital boarding costs.
Finally, analysis of post-traumatic serum concentrations of brain proteins might also have medicolegal implications. In a substantial number of patients with neuropsychological dysfunction 6 months after minor traumatic brain injury we found raised S-100B serum concentrations but no signs of intracranial pathology, EEG abnormality, or focal neurological deficits. In these patients post-traumatic serum concentrations of S-100B might help to clarify the likelihood of a causal relation between long term neuropsychological deficits and the initial head trauma.
Acknowledgments
This study was partially supported by a grant from the BMBF research program on neurotraumatology and neuropsychological rehabilitation (grant No 01 KO 9513/8), the State of Saxony-Anhalt, and the Research Commission of the Faculty of Medicine at Magdeburg University. Kits for the analysis of protein S-100B and NSE were provided by Byk-Sangtec Diagnostica, Dietzenbach, Germany. We thank Dr Wunderlich for technical assistance and Dr Wallesch for helpful advice during study design.