


Abstract
Background Care navigation is an avenue to link patients to activities or organisations that can help address non-medical needs affecting health and wellbeing. An understanding of how care navigation is being implemented across primary care is lacking.
Aim To determine how ‘care navigation’ is interpreted and currently implemented by clinical commissioning groups (CCGs).
Design and setting A cross-sectional study involving CCGs in England.
Method A questionnaire was sent to all CCGs inviting them to comment on who provided care navigation, the type of patients for whom care navigation was provided, how individuals were referred, and whether services were being evaluated. Responses were summarised using descriptive statistics.
Results The authors received usable responses from 83% of CCGs (n = 162), and of these >90% (n = 147) had some form of care navigation running in their area. A total of 75 different titles were used to describe the role. Most services were open to all adult patients, though particular groups may have been targeted; for example, people who are older and those with long-term conditions. Referrals tended to be made by a professional, or people were identified by a receptionist when they presented to a surgery. Evaluation of care navigation services was limited.
Conclusion There is a policy steer to engaging patients in social prescribing, using some form of care navigator to help with this. Results from this study highlight that, although this type of role is being provided, its implementation is heterogeneous. This could make comparison and the pooling of data on care navigation difficult. It may also leave patients unsure about what care navigation is about and how it could help them.
INTRODUCTION
Significant challenges are facing the long-term sustainability of NHS general practice. New models of care are proposed to help manage a rising workload while attending safely to patients’ problems.1 Social prescribing has received significant publicity in recent months as a means of addressing the non-medical issues that bring patients to general practice. It is one of the high-impact actions from NHS England for reducing GP workload,2 and in the NHS Long Term Plan it forms part of the drive to deliver personalised care.3 Social prescribing recognises that medical treatment alone may not be enough to enable people to overcome problems affecting how they feel in their body and mind. This reflects the World Health Organization’s definition of health as ‘... a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.’.4
To bolster delivery of social prescribing, the NHS has announced that it will train 1000 ‘link workers’ by the end of 2020/2021.3 ‘Care navigator’ is another term that has been used to describe this role,5 which is already being implemented in some parts of England. People providing care navigation connect patients to local groups and support services to address their non-medical needs. Health Education England has published a core competencies framework for care navigators, which includes abilities such as good communication and interpersonal skills, problem solving, and acting as a bridge between community, health, and social services.5
Within primary care, provision of care navigators has been advocated because health professionals are not necessarily aware of all local options available and struggle to keep abreast of the changing landscape within the voluntary and community sectors.6–7 These roles may be implemented in different ways. In some primary care settings, care navigation may be an additional element of a receptionist’s existing job, whereby they signpost patients to alternatives to medical care.8 In other cases, dedicated employees have time to spend with patients, co-producing an individual action plan with them and identifying ‘... suitable schemes using local knowledge and access to directories.’.9
Despite being a priority NHS policy, an understanding of how care navigation works, identifying which patients are most likely to benefit, and under which circumstances is lacking. Furthermore, there has been no systematic assessment to compare and contrast how the role is being implemented in England. To address these knowledge gaps, the authors are conducting a programme of work that includes a realist synthesis on the topic.10 After reading relevant literature for this review, the authors hypothesised that care navigation would be implemented in a range of ways across NHS clinical commissioning groups (CCGs). To explore this proposition, the authors surveyed all CCGs in England. Findings from this survey and the authors’ realist synthesis will help service users, providers, and commissioners to better understand the role of care navigators within NHS primary care and contribute to an evidence base to support NHS policy. The present survey aimed to explore how ‘care navigation’ is interpreted and currently implemented by CCGs in England. This focus came from discussion with members of the public consulted while undertaking the authors’ realist synthesis; they commented on a need for some degree of standardisation in terminology and who could be seen so that patients were aware of the role and what to expect when referred to a care navigator.
| Social prescribing is a high priority for the NHS, as reflected in its 2019 Long Term Plan and its commitment to funding ‘link workers’ (or ‘care navigators’) to facilitate its operation. However, there are several knowledge gaps in the understanding of this role, including how care navigation is interpreted and implemented by clinical commissioning groups (CCGs). This study’s survey of all CCGs in England highlights the heterogeneous manner in which care navigation is currently being rolled out across the country. Findings can inform policymaking and delivery of care navigation by advancing an understanding of differing provisions across England. |
How this fits in
METHOD
Design
This study was a cross-sectional survey examining the implementation of care navigation across CCGs in England.
Participants and procedure
A Freedom of Information request was sent to all 195 CCGs listed on NHS England’s website in October 2018. Requests were emailed in November and December 2018. Data collection ceased at the end of January 2019. The questionnaire included items that the authors wished to explore following consultation with key stakeholders as part of their realist synthesis; this included talking to providers of care navigation and members of the public. The questionnaire’s content was piloted and refined based on feedback from colleagues. It centred on the following:
whether the CCG offered care navigation (and reasons for not doing so);
determining who provided this support to patients and the term used for this role;
determining who the service was open to and how they were referred to; and
whether the service had been evaluated.
The questionnaire included the introduction in Box 1 and was sent as a Word document. CCGs had the opportunity to respond with as much or as little information as they wished. If a link to a webpage was provided within a CCG’s response, the authors also looked at this information. Full details of the questionnaire are available from the authors on request.
| ‘We are seeking to understand how care navigators (or equivalents) are being implemented across CCGs. “Care navigators” have been loosely described as someone who helps identify non-medical needs of patients, and supports and signposts them to available services in the community. Other terms may be used for this role, including social prescriber, link worker, or community connector. We would be extremely grateful if you could advise us on such services in your CCG by answering these very brief questions.’ |
CCG = clinical commissioning group.
Introduction to the questionnaire
Data management and analysis
Data were entered into Excel for analysis by the first author; 10% of data entry points were cross-checked by another member of the research team, who agreed with the way this information had been entered onto the database. When information provided to a question by a CCG was ambiguous, this response was coded as ‘unclear’. Descriptive statistics were computed within Excel.
RESULTS
Overall, 99% (n = 193) of CCGs responded to the survey, but not all supplied usable data (Figure 1). Depth of responses varied considerably across CCGs: some gave one word answers or succinct sentences. Others offered extensive feedback, stretching over several pages. No clear pattern was evident in the amount of information provided and number of care navigation services offered in an area covered by the CCG.

Responses to the questionnaire.
CCG = clinical commissioning group.
As shown in Figure 1, of the CCGs providing usable data (83%, n = 162), >90% (n = 147) had some form of care navigation in their area; 15 did not currently do so. Fourteen of these CCGs planned to do so in the near future and were in the process of developing a type of care navigation service. One CCG reported that it was not planning to offer care navigation because of a lack of finances. The remaining article focuses on responses from the 147 CCGs that did report currently offering some form of care navigation, 44 of which cited >1 care navigation service in their area; so in some responses >1 service is reflected within a single CCG. In the following results, per cent is used when showing findings for each CCG and numbers (n) when results are for all services across CCGs.
Types of people who provided care navigation, for example, receptionists, practice managers, paid care navigator, or volunteers
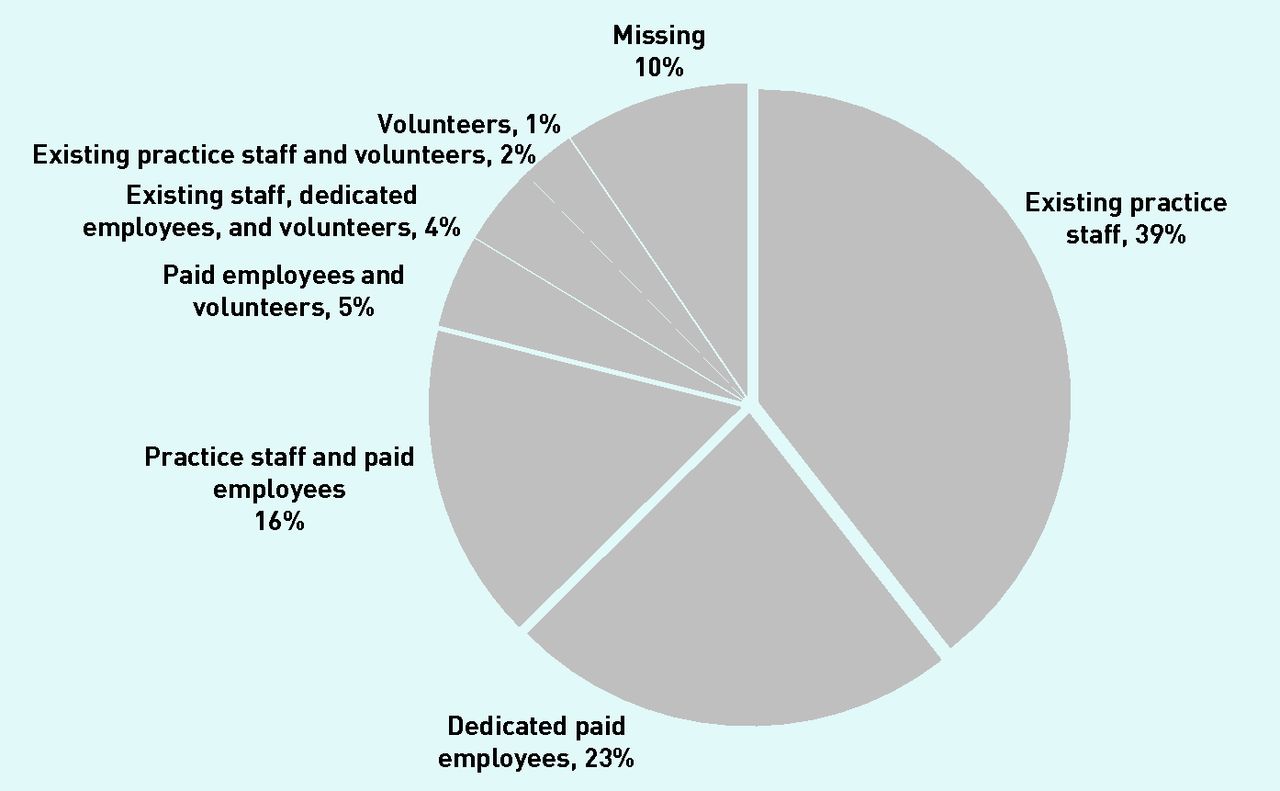
The most common provider of care navigation was an upskilled existing member of staff at a surgery, usually a receptionist, followed by people employed to work in a dedicated service (Figure 2); 16% of CCGs had a service run by dedicated workers as well as in-house provision delivered by existing staff from a surgery. Only one CCG mentioned a service run solely by volunteers.
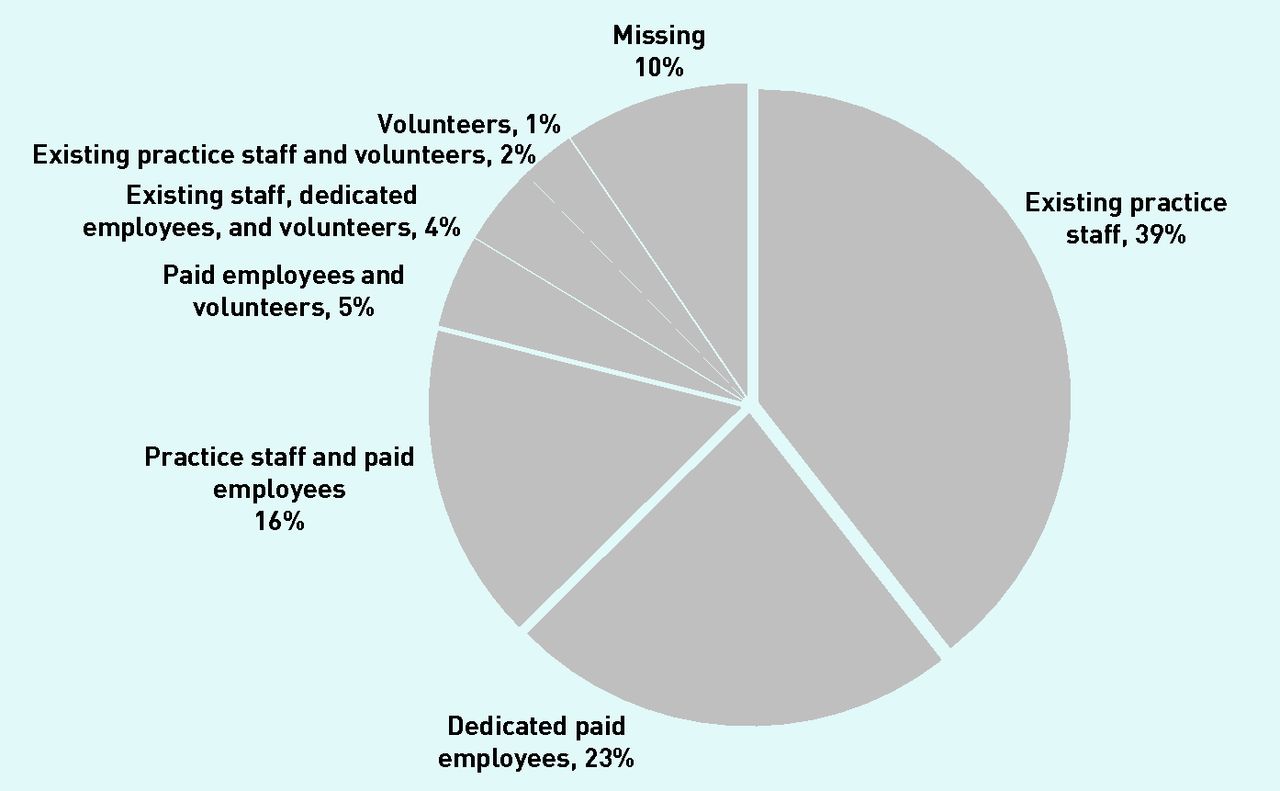
Types of people delivering care navigation for 147 clinical commissioning groups.
Term used to describe people undertaking this role, such as, care navigator, link worker, or community connector
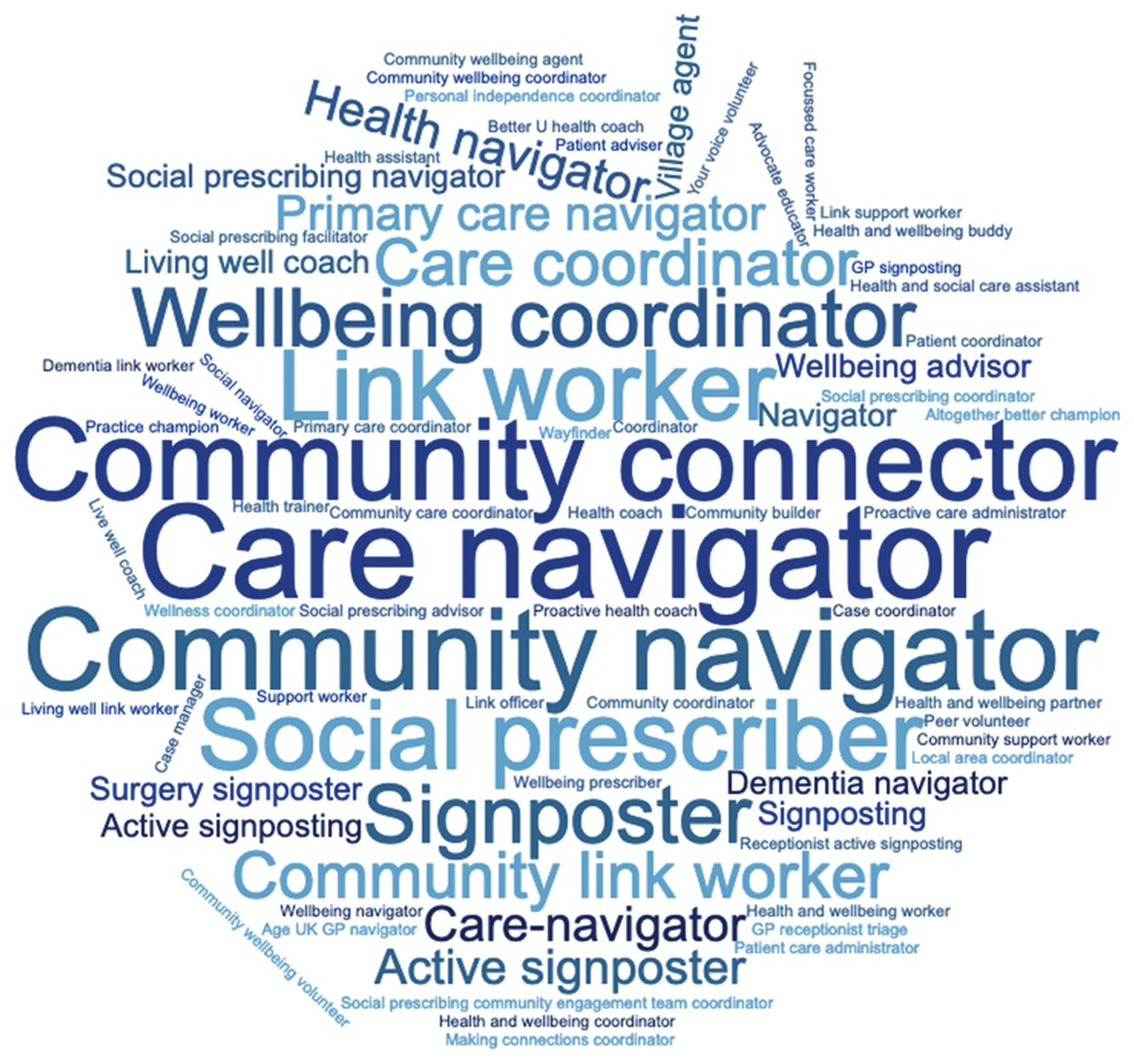
Overall, 75 different titles were mentioned by CCGs currently offering care navigation. Sometimes up to five different terms were used within the same CCG if several such services were run in an area. As shown in Figure 3, ‘care navigator’ or a derivative, for example, ‘primary care navigator’, was the most common term (referred to in responses from 86 CCGs), followed by ‘link worker’, including derivatives such as ‘community link worker’ (referred to by 14 CCGs), ‘social prescriber’ (referred to by 13 CCGs), or ‘signposter’/’signposting’ (referred to by 12 CCGs).

Word cloud illustrating range of terms used across 147 clinical commissioning groups for care navigator roles.
Type of people for whom the service is available, such as all patients or specific groups
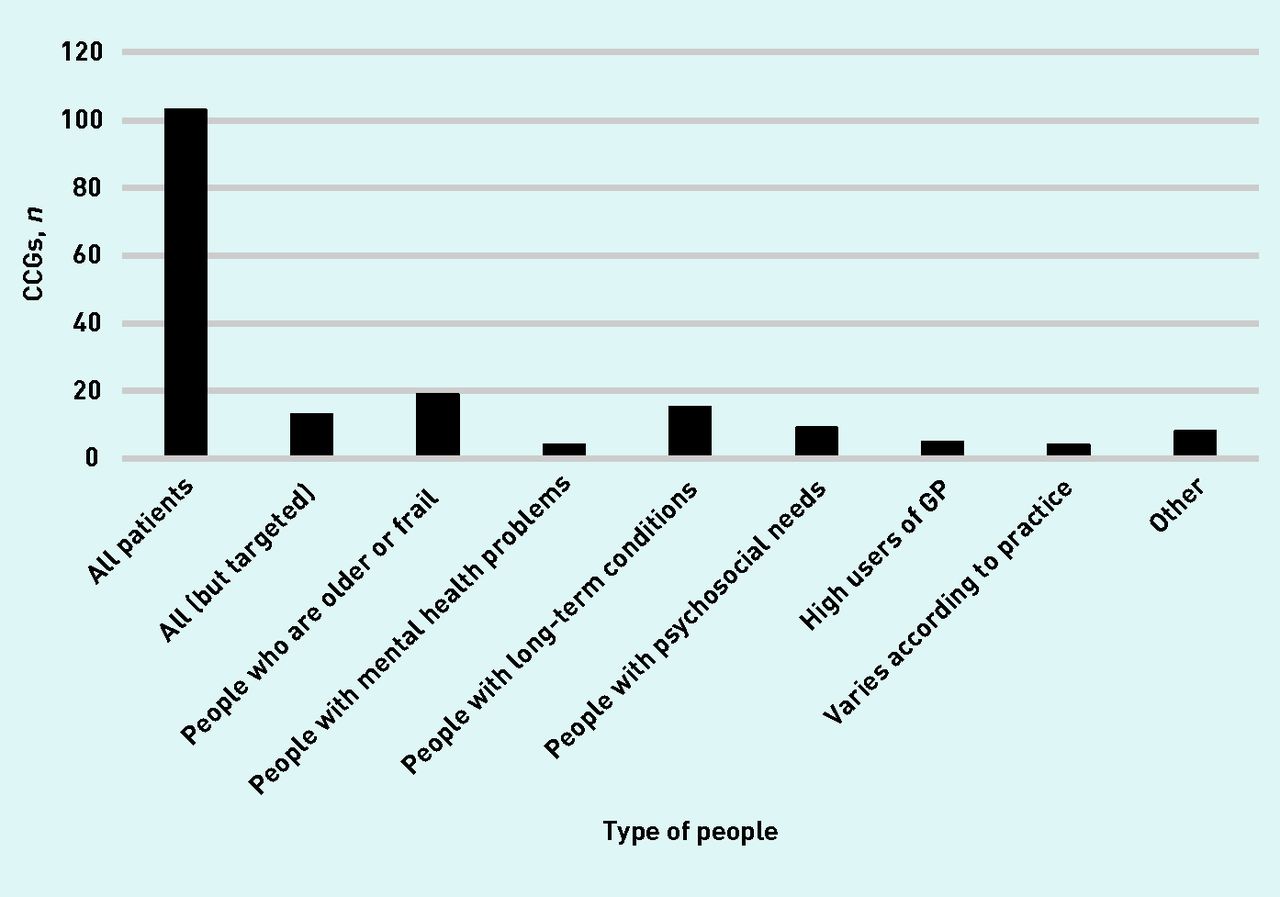
Most care navigation services were open to all adult patients, as shown in Figure 4; this tended to be the case when delivered by receptionists or other existing members of a practice. However, some CCGs (n = 13) made the caveat that, though accessible to all, particular groups were targeted, for example people who were older, those who were socially isolated, or high users of a surgery; this is shown as a separate category to those services available to all (Figure 4). Certain care navigation services were only for individuals meeting specific criteria; for example, people who were older or frail (n = 19), or those with a long-term condition (n = 15). Three CCGs mentioned using a risk stratification tool to identify patients who would be eligible. The ‘other’ category in Figure 4 refers to carers, people with dementia, or those receiving end-of-life care. The psychosocial needs category in Figure 4 includes services aimed at people experiencing isolation, loneliness, or anxiety (n = 9). Four of the 147 CCGs did not provide information for this question.

Type of people for whom the care navigator service is available. CCGs often provide more than one care navigation service, so in the same area one service may be open to all (often when delivered by receptionists), whereas another is more targeted.
CCG = clinical commissioning group.
Method of referral, or contact, with the service, for example, by a professional, or self-referral
When undertaken by a receptionist, care navigation commenced as a patient made contact with the surgery; for example, by phone or in person to arrange an appointment. Responses mentioned that these existing members of staff were trained to identify patients who may benefit from care navigation at this point of entry. In other cases, referral was made by a health or social care professional (under ‘community or primary care professional’, Figure 5). Two-thirds of CCGs providing this information had at least one service accepting referrals from primary or community professionals, which was sometimes alongside self-referral; GPs were often listed as the person making this referral. There were examples of wider referral routes; the ‘other’ category in Figure 5 included multidisciplinary team meetings, police, the fire brigade, libraries, pop-up clinics in supermarkets, ambulance services, rehabilitation teams, dementia team, carers/family, and mental health teams. Of the 147 CCGs, 11 did not provide information for this question.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Method of referral, or contact, with the care navigator service. A&E = accident and emergency. CCG = care commissioning group.
Evaluation of care navigation services
Of the 147 CCGs currently offering some form of care navigation, 22% mentioned that at least one such service in its area had been evaluated. Reasons for not evaluating included the limited time a service had been running; evaluations were mentioned as being planned or in process by 18 CCGs that had not reported such work being completed in their area. Services that had been evaluated tended to be dedicated schemes, involving staff employed to undertake care navigation type work. Most services had not been evaluated, especially if delivered in-house by existing primary care staff.
DISCUSSION
Summary
The present results show that care navigation is being offered in some form within most CCGs in England. Yet implementation of this relatively new position is extremely heterogeneous; the type of people who deliver care navigation, the type of people who receive it, and how people are referred varies across and within CCGs. Differences in implementation could reflect diverging interpretations of the role and the contrasting settings in which care navigation is employed in terms of resources, staffing, and local needs. Results show care navigation is often delivered by existing staff at a surgery, though some services have dedicated workers. Referral can take a number of forms, including self-referral, from a health or social care professional, and when receptionists answer calls to a surgery.
Strengths and limitations
The response rate in this study was high and gave a good idea of care navigation at a set point in time in NHS primary care. However, the landscape associated with care navigation is in flux and is liable to change over coming years as more attention and political backing is given to the widespread availability of social prescribing and the linking of patients to non-clinical support. Data received in this research sometimes required interpretation to be distilled into an Excel spreadsheet, especially when CCGs gave very extensive responses. Therefore, data entry was cross-checked for accuracy of summaries reported in Excel. There did not appear to be any pattern in terms of amount of information provided by a CCG and complexity of care navigation services in its locality. The authors may have received more standardised responses if they had used tick-box responses on the questionnaire, but this would have curtailed their understanding and the richness of comments collected. It should also be noted that there may have been services in an area of which a CCG was unaware, for example if offered outside the NHS; therefore, the number of services reported above may be an underestimation of what was on offer. However, the focus of the present study was on the interpretation and implementation of care navigation from the perspective of CCGs. The authors had asked CCGs for information on who provided their care navigation service (questions sent to CCGs are available from the authors on request). However, the indistinct and sometimes opaque nature of responses did not allow the authors to make clear interpretations of these data.
Comparison with existing literature
Heterogeneity was illustrated in the diversity of terms reported by CCGs for care navigation. Use of these differing titles may cause confusion among healthcare professionals and patients, possibly affecting referral and uptake; previous studies show that if people are uncertain about what the service is called, what it is for, and how it might help, they may have unrealistic expectations and/or feel sceptical about its usefulness to them.11–13 For care navigation to be accepted, a shift in thinking among professionals as well as patients may be required, from a medical model approach to one in which a broader array of solutions to people’s problems are considered.14–15 This has also been suggested by the Social Prescribing Network:
‘Managing expectations of what social prescribing can deliver is critical — for prescribers, commissioners and participants. The purpose of a social prescribing intervention is not necessarily to get a problem fixed, but rather to building a network that enables individuals to feel confident and empowered to address problems for themselves. Equally, the patient may have an expectation of receiving a medical prescription; a non-medical solution may take time for patients to adjust to.’16
Evaluating services is important for gauging how far care navigation meets local needs and improves patient wellbeing. However, the present results demonstrate there is little assessment of how well it is working and for whom. This paucity of evidence has been reported by others;17 nevertheless, provision of care navigators or link workers to support social prescribing has gathered momentum.3
Implications for research and practice
Results presented here have shown a trend for existing members of staff, such as receptionists or practice managers, to provide care navigation. This may allow for temporary diversion of patients from the GP. However, if patients are unhappy with the suggestions they receive, or feel that their difficulties remain, there is a chance they will return to the GP. Therefore, communication about the role of care navigators should be clear, so patients do not feel they are simply being blocked from seeing their GP.12 Furthermore, signposting in this way may not be suitable for patients lacking self-assurance, who have to be encouraged to try new activities. They may require more intensive interaction and support to engage with voluntary and community sector organisations.18–19 Appropriate training should be offered to these non-clinical members of staff if they are offering care navigation, to ensure they are working with patients who might benefit and do not overlook cases that actually require medical assistance.20
Provision of care navigation from a dedicated employee is likely to be a different experience for patients, as these workers have more time to spend with individuals, to uncover their needs and how to address these through available local assets; this includes having the opportunity to develop, with patients, and ways to overcome potential barriers, such as travel and childcare.18,21 However, caution is needed to ensure that patients do not become dependent on the care navigator,22 which would negate care navigation’s aim to empower and enable patients to take more control of their life and health.5
Heterogeneity in how care navigation is implemented means that aggregating data on its effectiveness, for example as part of a meta-analysis, will be difficult. It does make it a suitable area of focus for a realist approach, which seeks to answer questions about what works, for whom, why, and in what circumstances,23 by drawing on data from a diverse range of sources;24 the authors are aiming to uncover answers to these questions through their realist synthesis that is in progress.10 Future research could also explore who care navigators refer on to in order to understand whether there is a difference in the types of onward services used by those already based in a practice, such as receptionists, compared with those employed solely as care navigators. This would also highlight the range of voluntary and community sector organisations recognised and referred on to by care navigators. The survey in this study was not designed to explore differences in CCGs that offered more than one care navigation service; future research could consider this issue.
Acknowledgments
The authors would like to thank all CCGs providing data used in this article.
Notes
Funding
This project did not receive specific funding, but all authors’ salaries are partly supported by the Evidence Synthesis Working Group of the National Institute for Health Research School for Primary Care Research (NIHR SPCR) (project reference number 390).
Ethical approval
As this was an evaluation of current practice, ethical approval was not deemed to be required.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received March 5, 2019.
- Revision requested April 23, 2019.
- Accepted May 10, 2019.
- © British Journal of General Practice 2019
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

