


Abstract
Background Current evidence-based guidelines for low back pain (LBP) recommend multiple diverse approaches to treatment and suggest considering patient preferences when formulating a treatment plan.
Aim To explore patient preferences and to identify patients’ beliefs about LBP treatments.
Design and setting Qualitative study using focus groups in primary care in South-West England.
Method Thirteen focus groups were organised with a purposive sample of 75 adults with LBP. Group discussions of LBP treatments were facilitated, audiorecorded, and the verbatim transcripts thematically analysed.
Results Eight themes were identified, four related to treatment beliefs and four to seeking treatment. Treatment beliefs comprised participants’ expectations and appraisals of specific treatments, which were underpinned by four distinct dimensions: credibility, effectiveness, concerns and individual fit. Treatment beliefs were expressed in the broader context of treatment seeking: participants’ primary concern was to obtain a clear explanation of their LBP which went beyond a diagnostic label and provided an understanding of the cause(s) of their LBP. They described engaging in self-management activities and claimed they were willing to try anything if it might help them. Participants wanted an empathic and expert practitioner who could deliver a suitable treatment (or refer them on to someone else) and help them to negotiate the challenges of the healthcare system.
Conclusion These findings highlight the importance of helping patients develop coherent illness representations about their LBP before trying to engage them in treatment-decisions, uptake, or adherence. Addressing patients’ illness and treatment perceptions in clinical practice could improve shared decision making and patient outcomes.
- back pain
- health knowledge, attitudes, practice
- illness behaviour
- patient preference
- primary health care
- qualitative research
INTRODUCTION
Low back pain (LBP) is experienced by up to 84% of the population and is often accompanied by substantial personal, social, and economic consequences.1–3 No single treatment is universally effective; the challenge for patients and clinicians is to identify the optimum treatment for the individual. This is reflected in current evidence-based recommendations for LBP management which incorporate not only medical and psychological approaches but also physical treatments, exercise, and complementary and alternative medicines (CAMs).4–7
Recent models of stratified primary care based on risk of poor prognosis offer new approaches to matching patients to suitable treatments.8 Another approach is to consider patient preferences, in line with increasing awareness of the need to promote shared decision making in health care.9 Qualitative methods are ideally suited to patients’ perspectives in an open and non-directive manner.10 Prior qualitative research in LBP has focused on patients’ lived experiences, including desires for clear diagnosis, adequate explanations, instructions and pain relief, access to a range of diagnostic and treatment services, and partnerships with clinicians.11–15 Others have highlighted the psychological burden of LBP and struggles for understanding and legitimisation.16–20 Few have focused on patients’ perspectives on treatment. A qualitative study was conducted to explore patients’ beliefs about LBP treatments.
METHOD
Design
Focus groups were used to collect qualitative data because they: efficiently elicit qualitative data from multiple participants; produce data that reflect socially acceptable experiences, beliefs, and language; allow researchers to observe interactions between participants and thus reflect participants’ own understandings.21,22
The topic guide (Appendix 1) elicited discussion of multiple LBP treatments, with a focus on those named in the current UK clinical guidelines (medication, exercise, manual therapy, acupuncture, combined psychological and physical treatment programmes, and spinal surgery4); these overlap with other international guidelines.5–7
Participants
The inclusion criteria were: adult (≥ 18 years), conversant in English, history of LBP at least 6 weeks, not caused by fracture, infection, inflammatory disorder, cancer, or nerve root compression. Participants best placed to help explore beliefs about and experiences of LBP treatments were purposively sampled.23 As there was interest in how patients go about evaluating different treatments (not whether a treatment is evaluated positively or negatively), some participants who had and some who had not experienced each treatment, and some who had and had not found each treatment helpful were sampled. Diversity was also ensured in sex, age, and location.
How this fits in
Low back pain is prevalent in primary care where current evidence-based guidelines recommend taking into account patients’ preferences when choosing between medical approaches, psychological approaches, physical treatments, exercise, and complementary and alternative therapies. Previous qualitative studies have illustrated the psychosocial impact of low back pain and the challenges faced by sufferers. This study shows that patients’ beliefs about diverse treatments for low back pain are organised around four key dimensions (credibility, effectiveness, concerns, and individual fit). Clinicians should help patients to develop a coherent understanding of their back pain as a prerequisite to engaging them in treatment-related decision making.
Potential participants across South-West England were identified from a) lists of patients who had recently consulted their family doctor or CAM practitioner because of LBP and b) members of a chronic pain patient support group. They were informed about the study and invited to participate. Seventy-five responders participated in 13 focus groups. Participants were between 29 and 85 years old (median = 62 years), 64% were female, and approximately two-thirds had pain for more than 3 years (Table 1). Each focus group included 4–10 participants (median = 6) and lasted 70–90 minutes (mean/median 80). Groups were held during 2011 at doctors’ premises and were audiorecorded (with prior written informed consent), transcribed verbatim, and anonymised. Data analysis and collection proceeded iteratively; focus groups were stopped when participants with diverse experiences and characteristics had been sampled, when no new themes were apparent, and when existing themes were well-elaborated.24
Participants’ characteristics (N = 75)
Data analysis
Thematic analysis25 was conducted and NVivo (version 9) was used for data management and coding. After repeated reading of transcripts and listening to audiorecordings, participants’ talk was analysed at the level of meaning unit (a statement that expresses a single meaning). First, talk was deductively categorised as related to a recommended treatment (medication, exercise, manual therapy, acupuncture, combined psychological and physical treatment programmes, or spinal surgery), to other treatments, or to clinical management of LBP. Then, an inductive approach was taken to identify dimensions underlying participants’ perceptions of particular treatments (treatment beliefs) and themes related to the clinical management of LBP (collectively labelled treatment seeking). Strategies to enhance analytic rigour included constant comparison of categories, themes, and talk between and within focus groups and about the same and different treatments,24 coding led by one researcher reviewed by a second, and discussion of the emerging analysis by the research team (Appendix 2). Illustrative quotes presented below were selected from the coded transcripts for typicality and eloquence in illustrating the themes.
RESULTS
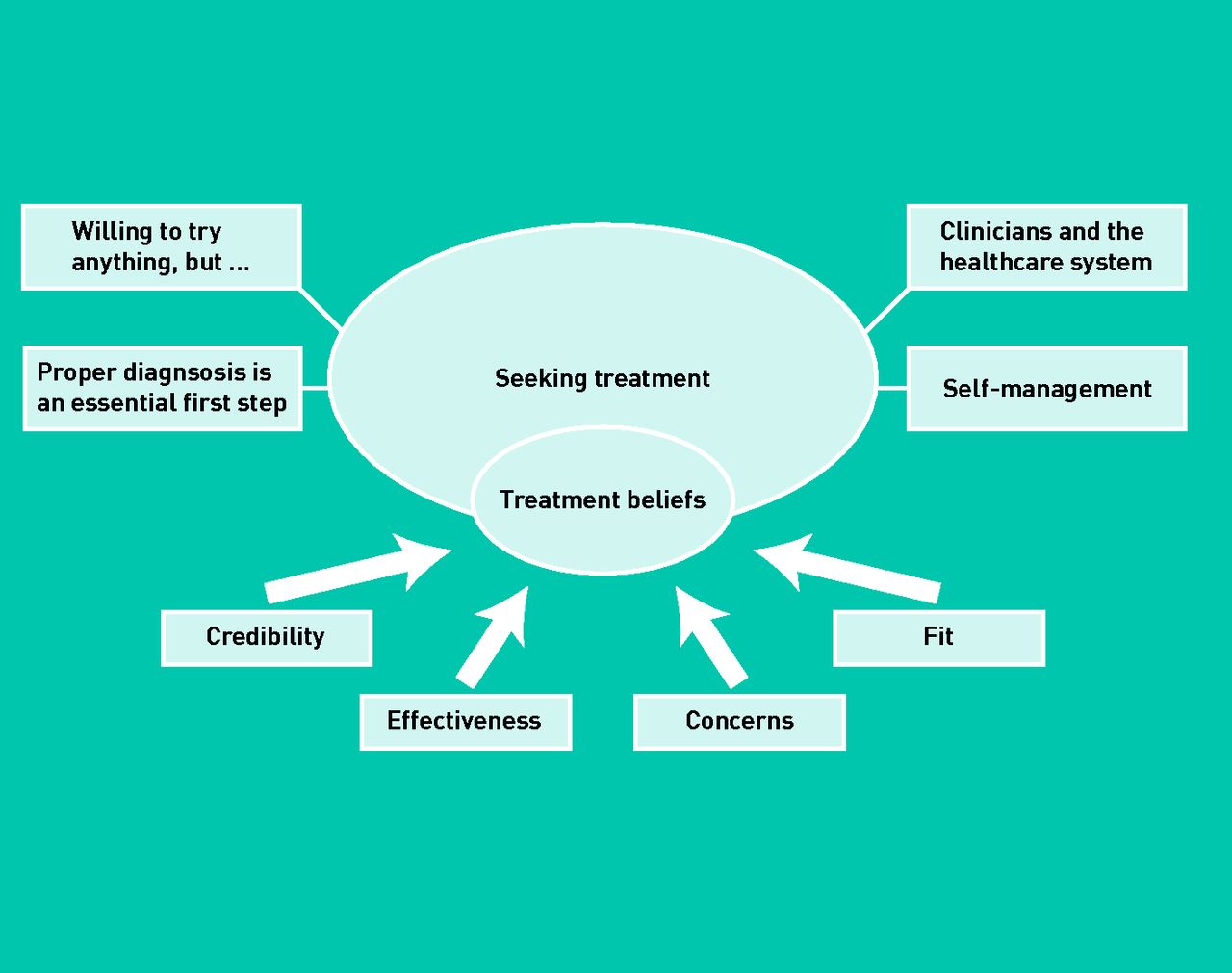
Figure 1 illustrates the main themes and their inter-relations.

{kind=link}
Thematic map showing themes related to treatment beliefs and seeking treatment.
Treatment beliefs
Participants evaluated treatments holistically across four dimensions of credibility, effectiveness, concerns, and individual fit; they balanced different considerations but prioritised effectiveness. Treatments moved in and out of favour contingent on factors such as personal experience and the other treatment options considered. Each dimension of treatment beliefs is described briefly; Table 2 summarises how these dimensions were expressed for each recommended treatment.
How treatment beliefs were expressed in relation to specific treatments
Credibility
According to participants, a treatment should be credible (a ‘proper treatment’), should ‘make sense’ (have a believable mechanism of action), and should be delivered by ‘the right practitioner’. Some participants argued that a treatment should match the perceived location and cause of their condition, for example, massage was credible for muscle problems. Table 3 illustrates strategies participants used for assessing credibility in the absence of personal experience. Credibility was often evaluated by comparing treatments, and a treatment perceived as lacking credibility could be considered for a trial period to assess its effectiveness and safety, or could become a preferred option if more credible treatments were tried and found ineffective.
Strategies participants used for assessing treatment and practitioner credibility in the absence of personal experience
Effectiveness
There was clear consensus that treatments should have proven effectiveness for LBP. Three treatments were discussed as potential cures which might enable a patient to regain prior good health (exercise, acupuncture, and manual therapy) but these treatments were also described by other participants as providing only temporary relief or preventing symptoms worsening. Medications were perceived as providing temporary relief, an ‘easy fix’ to avoid but not address the underlying problem. However, temporary relief could itself be a valued outcome if it enabled participants to retain or regain valued life activities or enable self-management. Some participants acknowledged that hoping for a permanent cure was unrealistic.
Concerns
Participants expressed concerns about the treatment costs (such as financial, time, and travel) and safety (such as longer-term side effects, risk of damage, and painful treatments). The specific content varied across treatments (Table 2), but generally concerns deterred participants from trying or led them to adjust or discontinue recommended treatments. For example, participants were deterred from trying acupuncture because of concerns over needles. They adjusted or stopped medication because of concerns about addiction, drug desensitisation, and the potential to cause further damage by masking pain.
When perceived effectiveness was high this could help participants overcome concerns:
‘You’ve got no chance of stopping it if it’s going to go wrong, so I think that the chiro[practor] from my own personal viewpoint would be I’ve got to see some positive results from others before I go for it myself‘.
(Male, FG11)
Individual fit
Participants discussed how, ideally, a treatment should fit the patient’s individual circumstances and characteristics (such as age, injury, and lifestyle) and get to the root cause of their LBP. An appropriate exercise programme would provide individualised recommendations (not standardised exercise print-outs) and supervision to ensure correct, safe, and effective exercise. While a good fit for the individual was seen as an important precursor for effective individual treatment, this was assessed independently of general treatment effectiveness:
‘Whenever they were doing any kind of massage or anything into my back, they were never hitting the spots ever, but I don’t think it’s down to them I think it’s whatever they do isn’t right for me’.
(Female, FG7)
Seeking treatment
Participants’ treatment beliefs were expressed and should be understood in the context of their broader treatment-seeking experiences.
‘Proper’ diagnosis is an essential first step
Receiving a diagnosis came as a relief for some participants, particularly those with concerns about possible sinister causes of LBP. However, diagnosis in its various forms was also experienced as insufficient, confusing, worrying, or dismissive. ‘Low back pain’ and similar labels were deemed insufficient generic diagnoses. Instead, participants wanted individualised explanations of the causal factors responsible for their pain:
‘We’ve all got pain and got different reasons for causing it I should think’ (Male, FG12).
Typically, physiological or anatomical explanations were sought and valued:
‘What helped me a lot […] was trying to understand what’s going on, you know, how the back works and what it looks like and what the muscles are and, you know, where the nerves are’
(Male, FG4).
Consistent with this perspective, participants argued that accurate diagnosis could only be achieved through detailed examination (assessment through physical touch) and/or tests (X-rays and MRI scans), although some limitations and risks of tests were acknowledged.
Without a clear diagnosis (identifying the cause of pain), participants did not see how an appropriate treatment could be selected (to resolve the cause of pain); treatment decisions in these circumstances were seen as unsystematic ‘hit-and-miss’ or ‘trial-and-error’, and treatments themselves were seen as potentially harmful, unlikely to help, and a waste of time and resources:
‘Certainly, at the moment, I don’t believe anything that I’ve been told is going to cure whatever I’ve got because I don’t know what I’ve got. So it’s a bit up in the air but can you see where I’m coming from; I need to know, so that I know what they are doing to me is going to help me.’
(Female, FG1)
Willing to try anything, but ..
Participants expressed willingness to experience different treatments (‘I’ll try anything’; Female, FG8), but usually qualified this by considering effectiveness (‘anything that would actually help and you know would help’; Male, FG12), or credibility (‘if a doctor said to me you need this done’; Female, FG8). Willingness to try different treatments was also contingent on their emerging effectiveness; participants talked about assessing effectiveness during ‘trial periods’. Opinions differed regarding the length of trial periods:
‘You know if it didn’t work the first time for me I would probably think that’s not for me, but you did try it three times so you know’
(Female, FG8).
Participants valued a systematic active approach to monitoring and evaluating initial effectiveness of individualised treatment within the context of an on-going therapeutic relationship:
‘I’d like an action plan so that after a certain time — so if he said to me, you know, let’s give it 3 months, I’ll give you all these exercises, I’ll give you this to do, I’ll give you that to do, come back in 3 months and let’s see where you are in 3 months’ time.’
(Female, FG2)
Clinicians and the healthcare system
Participants wanted clinicians to be knowledgeable, conscientious, empathic, respectful, and trustworthy; to acknowledge and believe individual’s experiences of pain; and to provide adequate treatment (according to the above dimensions). Participants were concerned not to be seen as malingerers or hypochondriacs; some described this as a reason for avoiding seeking care despite wanting treatment. Those who sought care found it distressing to feel disrespected or disbelieved by a practitioner. They discussed feeling ‘fobbed off’, ‘dumped’ and ‘dismissed’ when told to live with pain and that it had no physical cause or was a natural consequence of aging:
‘When you’re told ‘live with it’, it’s the most awful feeling, you know and sometimes you’re just reduced to tears because you think if they won’t help, what can you do?’
(Male, FG2).
Using the healthcare system was described as a challenging process of negotiating referrals, tests and treatments. Participants were concerned to maximise their chances of obtaining good quality care and to minimise demands on their personal resources (such as private sector financial costs, travel costs, timing of appointments, and waiting lists). Some participants greatly valued the advocacy role that family doctors can play in helping them to negotiate the system. As participants shared their experiences with each other during the focus groups a collaborative process of trying to understand how the system operates was observed. This encompassed discussions of procedures for obtaining appointments and referrals, allocation of resources, key decision-makers, and local availability of treatments (Table 4).
Excerpts from focus groups to illustrate participants sharing experiences about treatment seeking
Self-management
Recommended treatments were considered and used alongside self-management techniques, such as: changing postural habits and ergonomics; goal-setting and pacing; sleep behaviours and postures; emotion regulation and distraction. Techniques were seen as prohibitively difficult; as strategies that complement and/or supplement clinician-delivered treatment; and as valuable ways to take personal control of LBP. Participants who were unwilling to change their habits or lifestyle typically were not confident in their ability to self-manage or to make decisions; they preferred doctors to choose treatments for them (Table 4). Participants who primarily self-managed their LBP typically preferred to choose for themselves which clinicians to consult and/or which treatments to trial to supplement their daily self-management (for example, during flare-ups).
DISCUSSION
Summary
Four core dimensions underpinned patients’ beliefs about LBP therapies: credibility, effectiveness, concerns and individual fit. These beliefs were expressed in the broader context of self-management, clinicians, and health care systems. The participants’ primary concern was to obtain a clear explanation of their LBP that went beyond a diagnostic label to help them to understand the cause(s) of their pain. This appears to be an essential prerequisite for meaningful engagement with treatment decision making.
Strengths and limitations
Not all patients’ views of all LBP treatments were considered but many commonly recommended treatments have been covered. Participants had persistent, chronic, or recurrent LBP; they might have better-elaborated and more entrenched views about treatments than patients with acute LBP. Participants were recruited from South-West England; the findings will reflect local health services. Focus groups allowed the study to observe patients learning from each other, but participants who had experienced a particular treatment tended to contribute more to discussions of that treatment than those with less experience.
Comparison with existing literature
This study’s findings can be interpreted in relation to Leventhal’s commonsense model of illness behaviour, according to which patients form illness representations26 and treatment beliefs27 which inform the iterative selection and appraisal of coping strategies including healthcare utilisation.28–30 In the current study, patients wanted a clear explanation of their pain which provided not only a diagnostic label but, more importantly, an individualised causal understanding; that is, they were striving to develop a realistic illness representation. This was an essential prerequisite for engaging with treatment decisions: uncertain and poorly elaborated understandings of LBP appeared to have a dramatic impact, driving reluctance to engage with decision making and/or recommended treatments. Others have similarly described the impact of illness uncertainty (and lack of legitimisation) on psychosocial adjustment15,18,19,31 and patients’ often-frustrated desires for clear explanations for pain.11,12,14,16 The current study extends this literature by demonstrating the potential consequences of illness uncertainty for treatment beliefs and decisions in patients with chronic LBP.
Four core dimensions underpinning treatment beliefs about diverse therapeutic approaches were identified: a treatment should have a credible mechanism of action and be delivered by a credible clinician, should have proven effectiveness in attaining a relevant short- or long-term goal, should prompt few concerns about safety and accessibility, and should be a good individual fit for the person’s diagnosis and life circumstances. These constructs partially overlap with dimensions underpinning beliefs about medicines (necessity and concerns)32,33 and constructs from psychotherapy (credibility and expectancy).34 Patients’ beliefs about LBP treatments cannot fully be understood with these existing constructs, as individualised fit is essential in this context.
Implications for practice and research
Quantitative studies are needed to test hypotheses concerning the correlates and impact of patients’ treatment beliefs. A questionnaire to measure the range of LBP treatment beliefs identified here is being validated; this will enable future studies to compare treatment beliefs between different groups of patients (for example acute/chronic LBP; males/females; treatment experienced/naive) and to test the impact of treatment beliefs on treatment-related decisions, behaviours, and outcomes.
Many clinicians struggle with communicating a clear explanation or specific diagnosis for patients with LBP35–37 and guidelines consistently recommend a focused history and physical examination but no routine imaging.4–7 Indeed achieving reliable and valid, specific, diagnoses for most patients with LBP is neither possible nor desirable.38 This study’s participants’ desire for causal explanations suggests greater educational efforts are needed to explain to the general public why diagnostic tests such as X-rays are not routinely recommended. This would usefully assist clinicians’ efforts in addressing diagnostic expectations of individual patients.
Offering information about treatments in a standardised, non-interactive, format (such as a leaflet) is likely to be of limited value, since LBP patients tend to prefer an individualised approach and differ in their information needs. Stiggelbout and colleagues9 recommend a strategy to achieve patient-centred decision making in consultations; this study suggests adjustments to this process for patients with LBP. These are summarised in Table 5. This approach could be further developed to support clinicians in helping their patients to develop illness representations that are coherent and pragmatic (that is, perceived as useful for guiding action). Clinicians could use the common-sense model to guide discussion around the core dimensions of illness perception: identity (symptoms and diagnostic label), causal factors (heavily emphasised by this study’s participants), timeline, consequences, and controllability (probing the specific dimensions of treatment beliefs identified above).39 Developing and testing such a theory-driven, consultation-based, communication strategy to improve proximal (such as treatment uptake, adherence) and distal (such as function) health outcomes may be helpful.
Patient-centred decision making processes
Acknowledgments
We thank the participants for sharing their experiences and the Primary Care Research Network and all the clinicians who helped to recruit the participants.
Appendix 1. Focus group topic guide
Generate a list of treatments that participants:
○ Have tried in the past
○ Would like to try
○ Do not want to try
Open discussion of each treatment, including:
○ Personal experiences
○ Advantages
○ Disadvantages
○ Reasons for use/not use
Open discussion of experiences of seeking care for low back pain
Generate a wish-list of desired approach and treatments for low back pain in primary care
Appendix 2. The influence of the researchers on the qualitative analysis
A critical realist approach to this work was taken. The ontological assumption is that while participants’ experiences cannot be objectively observed by attending to their accounts, their accounts can be treated as a representation of their experiences. Epistemologically, it can be assumed that the act of research (in this case the focus group) has an unavoidable role in shaping the participants’ talk and that the analyst similarly brings existing theories and knowledge to bear when interpreting the data. It is possible to reduce the inappropriate influences of the researchers in the production of what is necessarily culturally-bound knowledge. By describing the background here it is hoped to render transparent the theories and knowledge that were drew on when interpreting the data.
The analysis was led by Alexandra Dima, who also organised the focus groups. She is a post-doctoral researcher in health psychology interested in how patients manage chronic conditions, including their perceptions of illness and treatments, their health behaviours and their communication with the healthcare providers. Her doctoral thesis focused on patient’s adjustment to chronic pain conditions, including low back pain. She is familiar with various theoretical models of heath behaviour and pain perception and coping. Felicity L Bishop had detailed input into the coding and interpretation. She is lecturer in health psychology at the University of Southampton with particular research interests in how and why patients use complementary and alternative medicines and prior familiarity with Leventhal’s common sense model as well as other health psychological models and frameworks related to illness behaviour.
All other authors contributed to data interpretation.
Nadine E Foster is a physiotherapist whose research involves testing treatments and services for patients with common musculoskeletal problems, including low back pain, in primary care. Her research has identified that patients perceptions about their back pain at the time of consultation predict their clinical outcome in the short and long term, and that using a range of key predictors of outcome, in one brief index of risk, to match back pain patients to treatments, provides clinical and cost benefits for patients and health services. Rona Moss-Morris has carried out research in LBP including studies investigating 1) cognitive processes of change across a multidisciplinary pain management programme and 2) Patients’ expectations of a pain management programme. She has just started a new study investigating pain in MS. George T Lewith is professor of health research at the University of Southampton and leader of the Integrated Medicine research group; he has a long-standing research interest in acupuncture and has used it in his own clinical practice. Paul Little is professor of primary care research at the University of Southampton who has research interests in low back pain (in particular the Alexander technique) and doctor–patient communication in primary care.
Overall, working in a multidisciplinary team enabled us to avoid drawing premature conclusions and helped sensitise us to diverse interpretations of the data.
Notes
Funding
This article presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. This study was funded by the NIHR School for Primary Care Research (Project Number 75). Felicity L Bishop’s post was funded by Arthritis Research UK (Career Development Fellowship 18099). George T Lewith’s post is supported by a grant from the Rufford Maurice Laing Foundation. Nadine E Foster’s post is supported by a NIHR Research Professorship.
Ethical approval
Obtained ethics approval from Southampton and South West Hampshire REC B (10/H0504/78).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received November 23, 2012.
- Revision received December 20, 2012.
- Accepted April 26, 2013.
- © British Journal of General Practice 2013
This article is Open Access: CC BY-NC 3.0 license (http://creativecommons.org/licenses/by-nc/3.0/).
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

