


Abstract
Background Injuries are common and make a significant contribution to sickness absence, but little is known about problems experienced by injured people on return to work (RTW).
Aim To quantify work problems on RTW and explore predictors of such problems.
Design & setting Multicentre longitudinal study in four UK hospitals.
Method Prospective study of injured participants aged 16–65 years who were employed or self-employed prior to the injury and had RTW at 1 or 4 months post injury.
Results At 1 month, most (59%) had only made a partial RTW. By 4 months, 80% had fully RTW. Those who had partially RTW had problems related to physical tasks (work limited for median of 25% of time at 1 month, 18% at 4 months), time management (10% at 1 month, 20% at 4 months) and output demands (10% at 1 month, 15% at 4 months). Productivity losses were significantly greater among those with partial than full RTW at 1 month (median 3.3% versus 0.9%, P<0.001) and 4 months (median 4.6% versus 1.1% P = 0.03). Moderate/severe injuries (relative risk [RR] 1.93, 95% confidence interval [CI] = 1.35 to 2.77) and sports injuries (RR 1.73, 95% CI = 1.12 to 2.67) were associated with significantly greater productivity losses at 1 month while pre-existing long-term illnesses (RR 2.12, 95% CI = 1.38 to 3.27) and upper limb injuries (RR 1.64, 95% CI = 1.06 to 2.53) were at 4 months.
Conclusion Injuries impact on successful RTW for at least 4 months. Those who have only partially RTW experience the most problems and GPs should pay particular attention to identifying work problems in this group and ways of minimising such problems.
INTRODUCTION
Injuries to working-age adults are common, accounting for more than 400 000 hospital admissions annually in England1 and 2.8 million emergency department (ED) attendances in the UK.2 More than 10% of all GP sick notes are issued for injuries3 and injuries account for approximately 5% of incapacity benefit claimants.3 As there is evidence that work has a positive impact on health,4 facilitating return to work (RTW) following illness or injury is central to the government’s strategy for the health and wellbeing of working-age adults.5 GPs have a key role in helping people RTW, but often feel ill-equipped to offer advice in this area.3 Consequently national training on this issue is being provided for GPs.6
A range of workplace interventions are effective in facilitating RTW and reducing the costs of sickness absence in those with injuries, although most studies relate to musculoskeletal and work-related injuries.7-10 While getting back to work is important, it is making a successful RTW that is vital:
‘A timely, well-planned and well-executed return to work process will have substantial positive benefits for an employees’ well-being and rehabilitation …’.10
However, little is known about the problems injured people experience on their RTW. Only one UK study of road traffic injured ED attenders was found. This reported that 17% of participants reported minor, and 6% reported major work problems 1 year after their injury but did not describe the types of problems experienced.11
The role of the GP and primary healthcare team in facilitating RTW has received recent attention.3 GPs need to understand the problems people are likely to experience on RTW, and who is most likely to experience these problems, so that they can work effectively with patients, employers, and other healthcare professionals to ensure a successful RTW. This aim of this article is to describe and quantify work problems experienced by people following injury and investigate predictors of such problems.
How this fits in
Injuries limit ability to perform a range of tasks after returning to work for at least 4 months, especially among those who have only partially RTW, those with more severe injuries, sports injuries, those with pre-existing long-term illness and with upper limb injuries. Problems are most common with physical, time management, and output aspects of work. Primary care consultations should explore the full range of potential work-related problems, use fit notes to recommend evidence-based interventions to employers, and refer patients to specific RTW or occupational health services where these exist.
METHOD
This paper presents a secondary analysis of data on work problems after RTW among a subset of participants from a longitudinal prospective study of people aged ≥5 years with a wide range of injuries attending an ED in four centres in the UK (Swansea, Nottingham, Bristol, and Guildford [Surrey]). Participants were recruited between September 2005 and April 2007. The protocol for the study has been published elsewhere.12 In brief, self-completed questionnaire data were collected at recruitment and by post at 1, 4 and 12 months post injury. Once participants reported complete recovery, no further questionnaires were sent. Baseline data comprised details about the injury, sociodemographic information, long-term illness, and general health (EQ5D) and employment status prior to injury. Follow-up questionnaires collected data on recovery, use of health and social services, time off work in the preceding month, work problems for those who had RTW, and general health (EQ5D).
The analyses presented here focus on those aged 16–65 years who were working prior to the injury and who had RTW at 1 or 4 months post injury. The degree to which health problems interfered with ability to perform the job was assessed using the 25-item Work Limitations Questionnaire (WLQ).13 This includes 25 specific job tasks across four domains; time management, physical, mental-interpersonal and output demands as described in Table 2. Domain scores represent the percentage of time in the preceding 2 weeks that work was limited. A productivity loss score combines scores across all domains and represents the percentage reduction in output between those with and without work limitations (D Lerner, WH Rogers, H Chang, personal communication, 2009). Full RTW was defined as the injury had not prevented working during the last month and partial RTW was defined as the injury had prevented working for between 1 and 19 days in the last month. Those whose injury had prevented them for working for ≥20 days in the last month were assumed not to have RTW and were excluded from the analysis. Where participants did not answer this question but reported they had returned to normal activities on other questions, it was assumed they had fully RTW.
Work limitations among those who had fully or partially returned to work 1 month post injury
Statistical analysis
It was hypothesised that those with a partial RTW would experience more problems than those with a full RTW. Individual tasks of the WLQ were categorised into those reporting difficulties for less than 50% or at least 50% of the time and comparisons by RTW status (that is, partial or full RTW) at 1 and 4 months were made using χ2 tests. Domain scores and the productivity loss score were compared by RTW status at 1 and 4 months using Wilcoxon tests.
It was also hypothesised that factors previously found to be associated with RTW may also predict work problems and explored predictors of productivity loss at 1 and 4 months. The productivity loss score was highly skewed, so it was dichotomised it at the median at each time point. Poisson regression, with a robust variance estimator was used to estimate relative risks.14 Age was categorised into three groups; deprivation15 score was categorised into tertiles; injury type into upper limb, lower limb, and other injuries; and injury severity (measured using the Abbreviated Injury Scale16) was categorised into minor and moderate/severe. This study presents results from backward stepwise regression models, forcing study centre into the model, and only retaining other variables if the Wald test for their removal was significant (P<0.05). Observations with missing data were excluded and model assumptions were checked.
RESULTS
A total of 1517 participants were recruited into the prospective study of which 664 were aged 16–65 years and were working prior to the injury and were therefore eligible for these analyses.
The flow of participants through the study is shown in Figures 1 and 2. At 1 month, 53% of responders had RTW, but 59% of these had only partially RTW. At 4 months, 71% of responders had RTW, and 80% of these had now fully RTW.
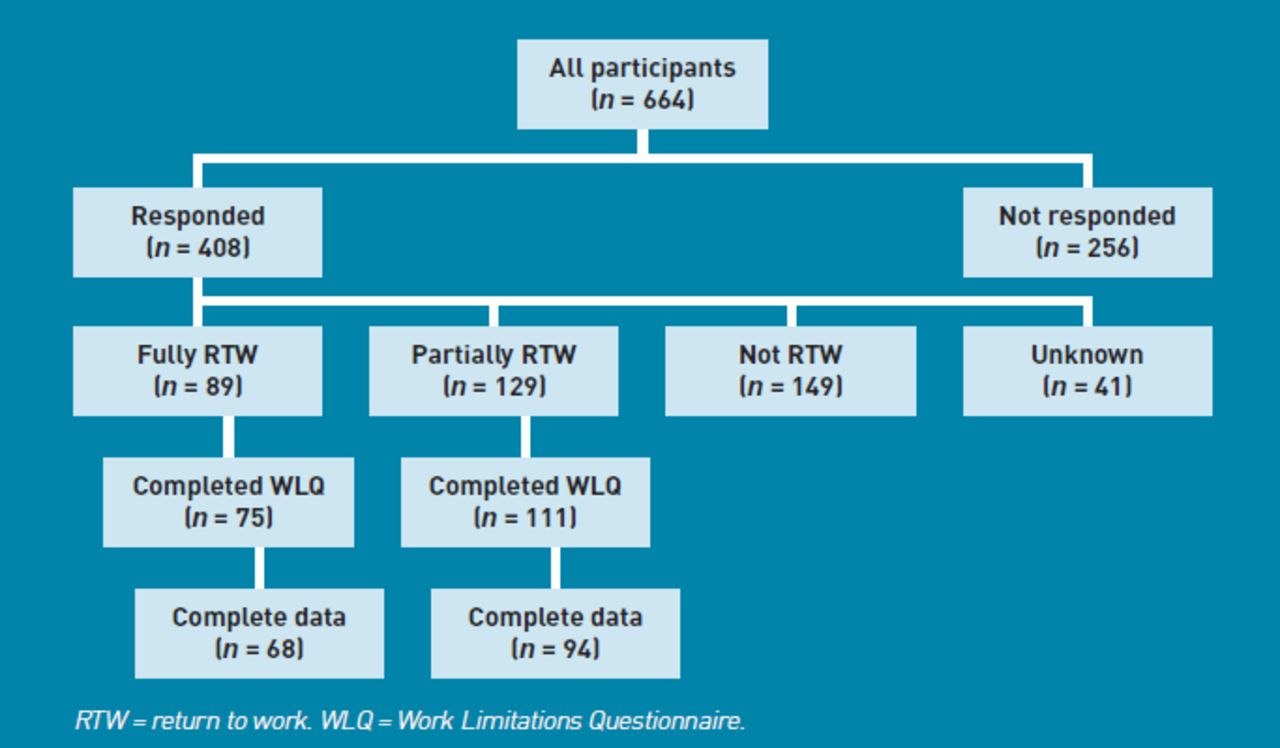
Responders and non-responders to the 1 month questionnaire.

{kind=link}
{kind=link}
Responders and non-responders to the 4 month questionnaire.
Table 1 shows baseline characteristics of those that had RTW at 1 and 4 months. At 1 month post injury, just over half (58%) were male and just under half (43%) were aged 36–55 years. Most injuries had occurred at home (26%), and fewest had occurred at work (15%). Lower limb (31%) and other injuries (41%, comprising superficial injuries or open wounds [20%], facial [5%], spine [5%], burns [5%], and other injuries [6%]) were most common and 47% of these were moderate or severe injuries. Similarly, of those who had RTW at 4 months, 56% were male, 48% aged 36–55 years and 18% had their injury at home and 12% at work. Lower limb injuries (41%) were the most common and 68% were moderate or severe injuries. Very few participants at either time point had suffered intentional injuries (for example, assault, self-harm).
Baseline characteristics of study participants who had fully or partially returned to work at 1 and 4 months post injury
Tables 2 and 3 shows that at both time points those who had partially RTW experienced work limitations for significantly more time for all domains than those who had fully RTW. Among those who had partially RTW, most time was limited by physical demands (work was limited for a median of 25% of time at 1 month and 18% at 4 months) and time management demands (work was limited for a median of 10% of time at 1 month and 20% at 4 months), with problems due to physical demands becoming less common and those due to time management demands becoming more common at 4 months. Less time was limited by output demands (10% of time at 1 month and 15% at 4 months) and mental demands (6% at 1 month and 3% at 4 months), and problems with output demands were slightly more common at 4 months than at 1 month. Those who had only partially RTW were significantly less productive at work at 1 month (partial RTW: median productivity loss score 3.3% (interquartile range [IQR] 0.9–7.1); full RTW: median productivity loss score 0.9% (IQR 0.0–4.4, P<0.001) and at 4 months (partial RTW: median productivity loss score 4.6% (IQR 0.7–7.4); full RTW: median productivity loss score 1.1% (IQR 0.0–4.6, P = 0.028).
Work limitations among those who had fully or partially returned to work 4 months post injury
Table 4 shows that at 1 month post injury those with moderate or severe injuries were significantly less productive at work (relative risk [RR] of above median productivity loss score 1.93, 95% confidence interval [CI] = 1.35 to 2.77 compared with minor injuries), as were those whose injuries occurred at sports grounds (RR of above median productivity loss score 1.73, 95% CI = 1.12 to 2.67 compared with home injuries). Table 5 shows that at 4 months post injury those with a pre-existing long-term illness (RR of above median productivity loss score 2.12, 95% CI = 1.38 to 3.27 compared with no long-term illness) and those with upper limb injuries (RR of above median productivity loss score 1.64, 95% CI = 1.06 to 2.53 compared with other injuries) were significantly less productive at work.
Factors associated with productivity loss at 1 month post injury and unadjusted and adjusted relative risks
Factors associated with productivity loss at 4 months post injury and unadjusted and adjusted relative risks
DISCUSSION
Summary
One month post injury only two-fifths of those who had RTW had made a full return. By 4 months four-fifths had fully RTW. Work was limited in terms of physical, time management, and output demands at both 1 and 4 months particularly among those who had only partially RTW. Fewer people experienced limitations in terms of physical demands as time progressed, but more experienced problems with time management and output demands. Partial RTW was also associated with significantly poorer productivity at work. Those with more severe injuries and with injuries occurring at sports grounds were significantly less productive at work 1 month after injury, and those with pre-existing long-term illness and upper limb injuries were significantly less productive 4 months after injury.
Strengths and limitations
This is the largest UK study quantifying RTW problems in adults following a range of injuries. This study’s response rates are similar to the only comparable UK study reporting response rates over time,17 and are reasonable at 1 month post injury, but substantially lower at 4 months post injury. This will have resulted in limited power to detect associations between some factors and productivity loss. Characteristics of responders and non-responders at 1 and 4 months are available from the authors on request. At 1 month responders were more likely to be female, older, live in a less deprived area, have a more severe injury, and come from the Nottingham study centre. At 4 months the same factors were associated with response except deprivation was no longer significant. As more severe injuries were associated with greater productivity losses at 1 month, it is possible that this study’s 1-month estimates may possibly overestimate the ‘true’ productivity loss in the population. Some reassurance is provided in the main analysis of this longitudinal study where multiple imputation was used, based on factors associated with response, to impute health status data (EQ-5D utility index scores) and found only a small impact on health status scores at 1 or 4 months, suggesting major response bias is unlikely to have occurred.18
RTW is a complex process and this study’s definition of full and partial RTW is a crude measure of this. Therefore some of those with a phased RTW may have been misclassified as fully RTW and part-time workers as partially RTW. If such misclassification has occurred it is likely to underestimate the strength of relationships between work limitations and full or partial RTW.
While this study begins to describe work problems among the injured, many factors, other than those measured in the current study may be important predictors of problems on RTW. A significant proportion of people suffer depression, anxiety, 6 months following injury,19 and mental health problems are a common cause of reduced productivity.3 It was not possible to explore relationships between injury, mental health, and productivity loss in this study, but it is possible that problems with time management and output demands reflect, at least in part, injury-related mental health problems.
Comparisons with existing literature
The authors were unable to find any published UK work using the WLQ in people with a range of injuries with which to compare this study’s findings. One UK study of road traffic injured ED attenders found 17% of responders reported minor, and 6% reported major work problems 1 year following injury,11 but these were not reported in any more detail than this. The current study’s participants’ work was limited for a smaller amount of time for all types of work demands than Canadian workers with musculoskeletal disorders secondary to workplace injuries20 and Canadian workers with upper extremity work injuries.21 Workplace injuries may result in greater limitations than injuries occurring elsewhere because the injury may be related to particular work tasks such as lifting. In addition, seeking compensation and litigation may be more prevalent among those with workplace injuries and these may impact on RTW22-24 and problems after RTW.
This study’s participants’ work was limited in terms of physical demands for a similar amount of time as US employees with osteoarthritis25 and rheumatoid arthritis26 and appeared to be limited for a shorter period of time for other domains. Productivity loss scores were only slightly lower than those for US employees who were survivors of brain tumours with a range of survival times (mean 5.6, standard deviation [SD] 4.4),27 UK employees with asthma (mean 5.8, SD 6.6)28 and US employees with rheumatoid arthritis (mean 5.9 (SD 6.6).26 They were considerably lower than UK employees with depression and anxiety (mean 11.8, SD 6.1).28
Those with pre-existing long-term illness were significantly more likely to experience problems on RTW 4 months post injury. The authors have been unable to find any studies that have explored comorbidities in relation to work problems following injury, but they have been found to be associated with delayed RTW.29 Although the current findings are consistent with these, it is possible that productivity loss may be related, at least in part, to the pre-existing condition as opposed to the injury. In addition, the current findings are based on a very small number of participants. Further work is required to explore the impact of injury on work related problems in those with pre-existing conditions.
This study’s finding that those whose injuries occurred at sports or leisure facilities had greater productivity loss at 1 month is interesting. One study of time off work after life-threatening accidents found those with sports injuries returned to work more quickly and judged their coping abilities as higher than those with other injury types.30 Presenteeism, or working while ill, is a well-documented cause of productivity loss and is associated with personality and attitudes towards work.31 Presenteeism may at least partly explain the greater productivity losses among those with sports injuries. In this study partial RTW includes those very recently RTW, those with a phased RTW who are working fewer days than usual, and those who have RTW but had some sickness absence in the last 4 weeks. Thus, it is unsurprising that partial RTW is associated with more work-related problems and reduced productivity than full RTW, but presenteeism may also be important in explaining this difference.
Implications for practice and research
Injuries limit work, in terms of physical demands and lost productivity to a similar degree to osteoarthritis, rheumatoid arthritis and brain tumours. They limit time management and output demands to a lesser extent, and appear to have a smaller impact on mental-interpersonal demands. Work limitations change over time, with problems with physical demands decreasing and those with time management and output demands increasing. Those partially RTW, with more severe injuries, upper limb injuries, sports injuries and long-term illnesses are particularly at risk of work-related problems.
GPs are uniquely positioned to assess the potential impact of injuries on a patient’s ability to work, coordinate therapeutic interventions and assist in decision making about the employee’s readiness to RTW.32 Evidence-based interventions include modified work, contact between healthcare provider and the workplace, ergonomic workplace visits, early contact between workplace and worker and the use of RTW co-coordinators.7,8,33 GPs can use the fit note34 to facilitate such interventions by providing appropriate information to employers and consider referral to specific RTW services or occupational health services, where these exist. Such services maybe especially helpful where it is difficult for GPs to assess the hazards of the post, the risks these pose, how they could be controlled, and the interface of this with the presenting injury.
GPs should pay particular attention to identifying work problems in those partially RTW and ways of minimising such problems. The GP’s role is however, more complex, balancing the benefits of RTW with awareness that presenteeism could exacerbate injury-related disability, reduce quality of life at work, and perceptions of ineffectiveness can have a negative impact on both employer and employee.31 As the profile of work problems changes over time, GPs also need to repeatedly assess for work problems. Problems associated with time management, output demands, and lower productivity should alert the GP to consider possible mental health problems and to screen for these.
Further research is required to explore the wider range of factors potentially associated with problems on RTW. These include occupational factors such as the nature and specific demands of the work; organisational factors such as employer attitudes, willingness, and ability to adapt the workplace, duties, or time spent working; employer–employee relationships and organisational culture; and individual factors such as the nature of the injury, other physical and mental health conditions, recovery expectations, attitudes towards symptoms and towards work, litigation, and compensation. Large studies will be needed to enable differentiation between injury types and potential response bias needs to be considered in both their design and analysis. Further work is also required to explore the extent of presenteeism following injury and its correlates among those with different types of injuries.
Acknowledgments
The authors would like to thank all patients who participated in the study and staff at the four participating hospitals for facilitating the conduct of the study. The UK Burden of Injuries Study Group are: S Brophy, A Evans, RA Lyons, S Macey, I Pallister, School of Medicine, Swansea University, UK. B Carter, EL Towner, Centre for Child and Adolescent Health, University of the West of England, Bristol. N Christie, Centre for Transport Studies, Department of Civil, Environmental and Geomatic Engineering, University College London, London. J Sleney, Postgraduate Medical School, University of Surrey, Guilford. C Coupland, L Groom, D Kendrick, C Mulvaney, S Smith, Division of Primary Care, University of Nottingham, Nottingham. F Coffey, Emergency Department, Nottingham University Hospitals NHS Trust, Nottingham.
Notes
Funding
This work is based on independent research commissioned and funded by the Policy Research Programme in the Department of Health (reference number 0010009). The views expressed are not necessarily those of the department.
Ethical approval
Dyfed Powys Local Ethics Committee (Number: 05/WMW01/23).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received August 9, 2011.
- Revision received October 31, 2011.
- Accepted December 16, 2011.
- © British Journal of General Practice 2012
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

