Article Text

Abstract
Background Handover of patient information represents a critical time period during a patient's hospitalisation. While recent guidelines promote standardised communication during these patient care transitions, significant variability in structure and practice persists among hospitals and providers.
Methods The authors surveyed internal medicine residents regarding handover practices before and after introduction of a structured, web-based handover application. The handover application standardised patient data in a format suitable for both patient handovers and day-to-day patient management.
Results A total of 80 residents were surveyed prior to the intervention (80% response rate) and 161 residents during the intervention (average 68% response rate for all surveys distributed). At baseline, residents perceived deficits in handover practices related to the variability of information transferred and correlated that variability to near-miss events. After introduction of the handover application, 100% of handovers contained an updated problem list, active medications, and code status (compared to <55% at baseline, p<0.01); residents perceived approximately half as many near-miss events on call (31.5% vs 55%; p=0.0341) and were twice as likely to respond that they were confident or very confident in their patient handovers compared to traditional practices (93% vs 49%; p=0.01).
Conclusion Standardisation of information transmitted during patient handovers through the use of a structured, web-based application led to consistent transfer of vital patient information and was associated with improved resident confidence and fewer perceived near-miss events on call.
- Care transitions
- handoffs
- quality improvement
- graduate medical education
Statistics from Altmetric.com
Patient transitions of care, widely recognised as a vulnerable time during a hospitalisation, are associated with adverse events and near-misses.1–7 The patient handover is defined as the transfer of patient care and responsibility from one healthcare provider to another.8 ,9 Published literature describing handovers cites many synonymous terms such as hand-off, sign-out and sign-over; however, given recent language cited in the 2011 Accreditation Council of Graduate Medical Education (ACGME) resident core competencies, this manuscript utilises the term “handover” to describe this transition of care.10 Guidelines highlight the need for standardised communication during these patient care transitions.9 ,11 ,12 Since establishment of the Libby Law in 1989 and subsequent implementation of the 80 h resident work week, continuity of patient care has diminished and inhospital handovers have nearly doubled.13 ,14 The Institute of Medicine's recent recommendations to limit the intern workday to 16 h will nearly eliminate overnight intern call in effect; creating a greater number of patient handovers and continue to push transitions of care to the forefront of patient safety.11 Meanwhile, as patient handovers have become inevitable in the modern era of medicine, healthcare systems have not uniformly addressed measures to improve practice.15 ,16 Regulatory bodies, such as the Joint Commission and ACGME, have acted to raise awareness and promote greater competency to address this vulnerable period in patient care.10 ,12 Efforts to derive best-practice have exploded in recent years, with more than 70% of the literature focusing on handovers produced in the last decade.8
Evidence suggests that the manner in which residents hand over patients reflects institutional supports in which they work.15 Prior to this study, the J Willis Hurst Internal Medicine Residency program at Emory University—the largest in USA with 201 residents managing over 10 000 inpatient admissions and, very conservatively, more than 100 000 care transitions annually at an inner-city public hospital—had no predictable or standardised approach to patient handovers. Our objective was to evaluate resident perception of handover practice before and after introduction of a new, structured, web-based application designed to standardise information exchange and written communication during patient handovers.
Research design and methods
This study was approved by the Emory University Institutional Review Board. The web-based application used as the intervention could be accessed only by authorised users and was compliant with the Health Insurance Portability and Accountability Act. Resident surveys were voluntary and anonymous, and there were no consequences for those residents who chose not to participate. This study was implemented to provide initial data for future quality improvement studies surrounding handovers within Emory University's Internal Medicine residency program.
Preintervention
In order to assess practices within the residency program prior to any process change, residents were surveyed to assess the traditional methods of resident handovers, perceptions of handover practices that could potentially lead to patient harm, and the residents' willingness to adopt a new standardised method for handing over patient information. Resident responses were scored using a Likert scale.
Study design
Part 1: Prospective controlled comparison of handover intervention (figure 1)
We conducted a prospective study in a large inner-city hospital (Grady Memorial Hospital, Atlanta, Georgia, USA) between July and November 2009 that consisted of two phases: the first phase was a 1-month controlled trial of web-based sign-out (the “Intervention Group” teams) versus traditional sign-out (the ‘Control Group’ teams); the second phase was an additional 4 months of Intervention Group teams follow-up after the intervention was then applied to the entire cohort of teams.

Diagram of Methods Part 1: Prospective controlled comparison of handover intervention July–November 2009: perceptions of events on call. Phase 1: Control versus Intervention July 2009. Phase 2: Intervention applied to all teams August–November 2009. Part 2: Perceptions of Handover Content and Process October–November 2009.
The trial intervention was a web-based sign-out tool (WardManager) that standardised information provided at handover. WardManager was designed to function as a collaborative patient-list management and handover tool shared by all members of the care team. The application facilitates recording of structured patient information, including demographic data, the problem list, medication list, allergies, code status, details from the history of present illness, team to-do list and handover tasks. This tool was designed to function independently of the electronic medical record (EMR) and was accessible only by authorised users. Sample illustrations of the web application patient entry form and printed intervention overnight handover form are depicted in figures 2 and 3. The major differences between this web-based application handover form and traditional handover forms within our intervention hospital are that the traditional handover has no standardised required content, may not be accessible to all members of the team from any computer, and may not be secure or auditable.

Patient information entry dashboard on WardManager with included team census.
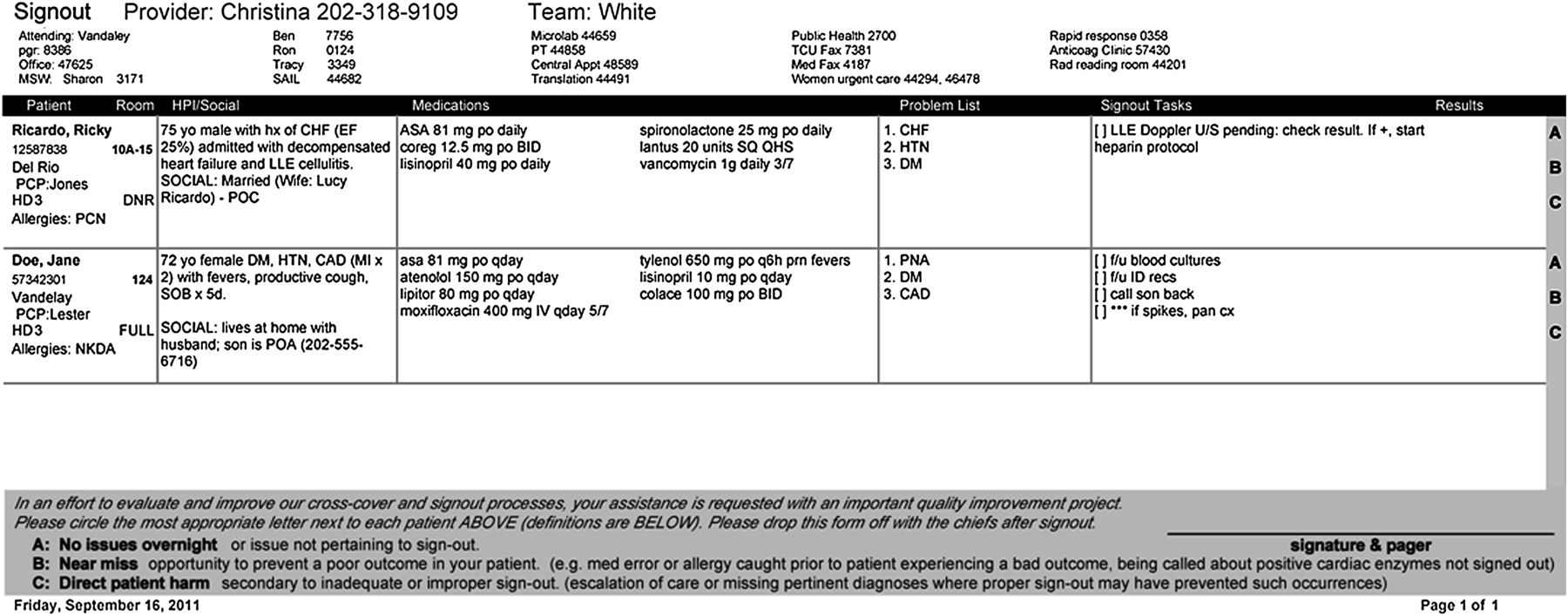
Example of printed intervention nightly handover form with survey.
During phase 1, four internal medicine teams were required to use WardManager to hand over patient information. The four teams required to use the web-based sign-out tool were chosen arbitrarily (one set of four teams, ie, teams 1–4) based on call structure. These four teams sign out to each other each night on call, thus making it imperative that each team within the set of four use the same tool. Concurrently, eight internal medicine teams (the other two sets of four teams, ie, teams 5–8 and teams 9–12) served as controls and continued their previous handover practices. During the second 4-month follow-up phase, WardManager was used by all 12 internal medicine teams, effectively dissolving the traditional handover process at Grady Memorial Hospital.
The typical on-call team at Grady Memorial Hospital consists of three postgraduate year 1 residents cross-covering a total of 12 internal medicine teams (four teams per resident), with an average cross-cover census of 35 patients (range, 15–48). Over the course of each month, 24 residents took 3–4 calls on average, roughly equivalent to one call every eighth night. Each of the residents taking call is on a specific team for that month and covers the same four teams each time s/he takes call. Example call structure functions in the following way: On Monday night, residents from teams 1, 5, and 9 take overnight call; on Tuesday, residents from teams 2, 6, and 10 take overnight call and so on, in a four night rotation. Each night, the same 4-day teams sign out to each other (1–4; 5–8; 9–12). In other words, for teams 1–4, one resident takes overnight call for all four teams and the individuals covering for those four teams rotate over the course of an 8 day cycle (ie, eight residents total take call for each group of four teams). Because of this system, no resident who took call from the WardManager group covered any patients in the ‘control’ group and vice versa.
Throughout both phases of the study, overnight residents covering all 12 internal medicine teams were surveyed each morning at handover to assess their perceptions about patient events related to the handover process, specifically focusing on inaccurate or missing information provided during the handover from the previous night and any related patient harm. Using a structured questionnaire for both the intervention and control teams, the residents were asked whether the previous night's handover led to any perceived patient ‘near-misses’ or ‘patient harm’ overnight. A ‘near-miss’ was defined as the opportunity to prevent a poor outcome in a patient (eg, a medication allergy caught prior to the patient experiencing a poor outcome; or being notified about positive cardiac enzymes that were not previously signed out). ‘Patient harm’ was defined as the escalation of care overnight or missing pertinent diagnoses where appropriate sign-out may have prevented such occurrences. These definitions were modified from previous similar ‘minor’ and ‘major’ patient harm definitions used in the handover literature.14 The questionnaire was incorporated into the WardManager handover printout (figure 3).
χ2 test of independence was used to compare the intervention and control groups based on the assumption that each call night was an independent event. This assumption was made because residents covered call every eighth night on average, so the likelihood that they cross-covered on the same set of patients was extremely low (given that the average length of stay for our facility's internal medicine patients is roughly 5 days). In addition, while the same patient was likely to be signed out on consecutive nights, the covering provider was different. Therefore their call night is independent of any of the previous call nights experienced by other providers. Likewise, although residents may have been surveyed up to four times a month, each call night and the sign-out received was independent of their previous call night. Finally, analysis of residents who may have repeated the ward month over the course of the 5-month period revealed that out of 124 residents who rotated at Grady Memorial Hospital, only 23 of these rotated twice (18.5%).
Part 2: Perceptions of handover content and process (figure 1)
The second part of the study took place over a 2-month period between October and November 2009. For this part, residents were separately surveyed once after their call night to determine their confidence in the quality of the handover they received and asked about handover content (inclusion of updated problem list, active medication list, and code status). This survey was separate from the survey and methods described in Part 1 as it was a one-time questionnaire specifically asking about handover content and confidence, not about perceived events on call. As WardManager was being used throughout Grady Memorial Hospital during these months, resident perceptions of handovers at Grady Memorial Hospital (Intervention Hospital) were compared to resident perceptions at two separate sister teaching hospitals (Emory University Hospital and Emory University Midtown Hospital, Atlanta, Georgia, USA) where our residents rotate but where no standardised handover tool was available (non-intervention hospitals) at the time of this study. Residents surveyed at Grady Memorial Hospital (intervention hospital) did not take call at the separate sister teaching hospitals, and vice versa. χ2 test of independence was used for comparison of these two groups.
Results
Baseline handover practices and perceptions: June 2009
At baseline a total of 80 residents (post-graduate years 2 and 3) were surveyed with a response rate of 85%. Residents identified four different electronic platforms used for patient-lists and daily handovers (Microsoft Word, Microsoft Excel, Google documents, and printouts of the EMR patient screens). Table 1 shows baseline resident perceptions regarding traditional handover practices. The preintervention survey showed that residents felt that traditional handover practices were incomplete and often led to patient safety issues, and that residents were willing to adopt a standardised method to handover their patients.
Baseline (preintervention) resident perceptions of nightly handover; N=68
Part 1: Perceptions of near-miss events
A total of 184 overnight surveys of perceived harm were collected from 124 residents rotating over 5 months (July–November). Table 2 illustrates the distribution of perceived near-miss and direct harm data collected over 5 months as well as summary data. For resident event reporting for overnight perceived events, the response rate in July for the intervention group was 86% (n=13) and the response rate for the control group in July was 73% (n=22). Over the next 4 months, August–November, the response rate was 63% (table 2).
Handover survey response rate, number of patients cross-covered, and perceived events
The perception of near-miss events was 55% (n=12) in the July control group, and the perception of near-miss events in the July intervention group was 23% (n=3) (p=0.0693). During the second phase (months August–November), when the intervention was applied to all subjects, the rates of perceived near-miss events was 31.5%; consistent with the July intervention period, and significantly less compared to the July control group; p=0.0341 (figure 4). Analysis of the perceived near-miss events revealed that none of the patients flagged by the cross-cover resident as a perceived near-miss or direct harm was flagged on subsequent call nights.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of perceived events (harm or near-miss) related to handovers in traditional handover group compared to standardised handover group over 5 months; N=184 surveys collected.
Part 2: Perceptions of handover content and process
In a separate one-time post-call questionnaire from months 4 and 5, a total of 92 surveys were collected. Residents of the 12 medicine teams in the WardManager (intervention) hospital (n= 41; 85% response rate) recorded inclusion of key patient information more often compared to residents of the non-intervention hospitals (n=51; 85% response rate): code status (100% vs 55%, p<0.01); problem list (100% vs 48%, p<0.01); and medication lists (100% vs 11%, p<0.01). Residents using the web-based application to standardise handovers (intervention hospital) also reported greater confidence in the information provided at handover (compared to non-intervention hospitals): 93% confident or very confident in intervention hospital versus 49% in non-intervention hospitals (p=0.01).
Discussion
Communication failures have been well-reported as root causes of sentinel events.11 ,12 Despite current mandates from regulatory agencies such as the Joint Commission,12 variability in handover practices persists within residency programs. One study of adverse event reporting by residents revealed that 15% of trainees perceived inadequate communication at handoff as the cause of their most recent error.17 Within another residency, suboptimal sign-out (omission of content such as active problem lists, medications and code status) was found by critical incident analysis of handoff communication failures to lead to uncertainty in decisions related to patient care.2 Our study indicates that omissions in critical information such as problem lists, medication lists, and code status may occur in more than 50% of traditional handovers.
We hypothesised that communication failures, particularly those resulting from omission and variability of content, could be addressed through the use of a standardised, web-based handover application. Although previous handover research has focused on the action portions of sign-outs (such as anticipatory guidance or ‘to-do’ lists), we chose to focus on standardising the process and transfer of basic patient information on the overnight sign-out. In this study, a structured web-based application designed to standardise basic patient information during handovers reduced handover content variability and represents a component of best-practice in nightly handovers. Compared to traditional, non-standardised handover methods, we found that a structured web-based handover tool was associated with a roughly 50% reduction in perceived near-miss events, perfect transfer of previously omitted vital patient information, and nearly a doubling of resident confidence in the nightly handover process.
In its 1999 report, To Err is Human, the Institute of Medicine asserted that ‘standardisation and simplification are two fundamentals of reliable organisations that are widely ignored in healthcare.’18 Standardisation probably assists verbal communication by making errors of omission more apparent and creating greater interprovider accountability at the time of handover. Other studies have suggested that standardisation of resident handovers leads to improved patient care.7 ,19–21 Despite this, a recent review of trainee and attending handovers concluded that insufficient evidence exists to support widespread standardisation of handover practices.22 While we agree that standardisation may be difficult to achieve on a national level, our study suggests that individual institutions and residency programs can improve patient care through the use of structured electronic handover tools to standardise minimum data sets transferred. To meet the handover goals put forth by the ACGME and the Joint Commission, hospitals and residency programs can begin to improve patient safety through the use of a technology aid to structure and standardise the content transmitted at handover.10 ,12
This study is one of several to date which assess the effectiveness of a computerised intervention on handover process and perceived outcomes.7 ,19 ,20 ,23 Meanwhile, residents have reported that technology to aid in handover data transmission is rare during medical residency.24 We purchased and implemented a web-based handover application precisely to address this weakness at the main teaching hospital in our residency program. This study served as an initial evaluation to determine the feasibility and effectiveness of standardising information transmitted at handover. Although the tool used to standardise handovers was not integrated with the EMR, residents still perceived this to be superior to prior practices of using multiple non-standardised programs to formulate the written handover. Previous research cites the danger of including non-EMR generated medication lists in a sign-out.5 Although medication lists generated by residents in this study did not appear to be a major source of error, this study did not examine the effectiveness of non-EMR generated medication lists on handover. The data generated in this study did prompt our institution to incorporate the same standardised handover format into the EMR generated handover tool within each of the four major hospitals of our residency training program.
The implications of this study may extend beyond residency programs to other hospital-based physician groups, as well as other types of care transitions within the hospital, such as change of clinical service, intrahospital transfers, and hospital discharges. Others have found that incomplete handovers during service changes can lead to uncertainty and potential patient harm.25 Additional information exchange strategies within high reliability organisations include face-to-face verbal discussion, ‘readbacks’ to enhance user understanding, and systematic and consistent communication protocols.26 Therefore, standardisation has the potential to expand beyond nightly handover templates and enhance the previously mentioned strategies to provide a consistent transfer of information within other areas of care transitions, such as intensive care unit to medical ward or hospital to outpatient clinic.
Our study has several obvious limitations. First, any survey-based design could introduce recall bias to influence results. We did attempt to mitigate that potential bias by surveying residents immediately following their overnight call episode. Second, selection bias could influence our results because residents at the intervention hospital take four overnight calls per month and may have rotated through wards during consecutive months (18% of residents rotated at the intervention hospital twice during the 5 months of the study). Since surveys were not tracked to individual residents, we were unable to limit this bias by tracking single responses. A third limitation may consider the lack of a robust and integrated EMR to support handovers. Our results therefore may not be generalisable to all medical settings. However, because many integrated EMRs likely allow for an integrated and standardised handover tool, our study demonstrates that standardising the handover process is possible even without an integrated EMR, as may be the case at many institutions. Finally, we report resident perceptions of near-miss events, but do not identify or quantify actual adverse events within the medical record. The difficulties in linking adverse events to specific handovers will remain a unique and perhaps non-ameliorable challenge for researchers interested in care transitions.8
In conclusion, we found that a structured web-based handover tool was associated with perception of significantly fewer near-misses, consistent inclusion of vital patient information, and greater resident confidence in the handover process. While hospitals are beginning to incorporate handover applications into their EMR, consensus is still lacking for how to measure and construct handover interventions.27 While standardisation is probably a fundamental step in reducing the variability of content transferred at handover, augmenting with other effective communication strategies should become a focus of handover training to improve patient safety during hospitalisation.
Acknowledgments
The authors thank Daniel Rosenthal, MD, MSc, MPH and Carlos del Rio, MD.
References
Footnotes
The authors have no financial or proprietary interest in any product mentioned herein. Data have been previously presented at the annual meetings of the Society of Hospital Medicine (SHM) and the American College of Physicians (ACP).
-
Competing interests None.
-
Ethics approval Emory University Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data available upon request from corresponding author.