Article Text

Abstract
Purpose Whether improving the efficiency of hospital care will worsen post-discharge outcomes is unclear. We designed this study to evaluate the General Internal Medicine (GIM) Care Transformation Initiative implemented at one of the seven teaching hospitals in the Canadian province of Alberta.
Methods Controlled before–after study of GIM patients hospitalised at the University of Alberta Hospital (UAH, intervention site, n=1896) or the six other teaching hospitals in Alberta—three in Edmonton (intra-regional controls (IRC), n=4550) and three in Calgary (extra-regional controls (ERC), n=4095). The primary effectiveness outcome was risk-adjusted length of stay (LOS) and the primary safety outcome was ‘mortality during index hospitalisation or all-cause readmission or death within 30-days of discharge’.
Results LOS for GIM patients decreased by 0.68 days at Alberta teaching hospitals between 2009 and 2012; GIM patients hospitalised at the UAH exhibited a further 20% relative decline in adjusted LOS (total reduction=1.43 days, 95% CI 0.94 to 1.92 days) from PRE to POST. Interrupted time series (ITS) confirmed that the 1.43 day reduction at the UAH was statistically significant (level change p=0.003), while the declines at the IRC (p=0.37) and ERC (p=0.45) were not. Our safety outcome did not change for UAH patients (18.4% PRE-intervention vs 17.8% POST-intervention, adjusted OR 1.02 (95%CI 0.80 to 1.31), p=0.42 on ITS), nor for those hospitalised at the IRC (p=0.33) or the ERC (p=0.73) sites.
Conclusions The Care Transformation Initiative was associated with substantial reductions in LOS without increasing post-discharge events commonly quoted as proxies for quality.
- Healthcare quality improvement
- Hospital medicine
- Implementation science
Statistics from Altmetric.com
Hospitalisations are the largest single category of healthcare expenditure and improving the efficiency of hospital care is seen as a priority in both Canada and the USA. However, many clinicians fear that reducing acute care lengths of stay (LOSs) may result in premature discharges leading to unintentional harm and increased costs in the form of increased presentations to emergency rooms and readmissions to hospital after discharge.1 ,2 Indeed, 30-day readmission rates already account for 11% of total hospitalisation costs3 ,4 and are commonly used as an indicator of suboptimal inpatient care and/or suboptimal transitions back to the community.5 ,6
In the fall of 2010, Alberta Health Services (the single health authority for the province of Alberta) implemented the General Internal Medicine (GIM) Care Transformation Initiative at one of the seven teaching hospitals in the province—the University of Alberta Hospital (UAH)—with the goal of reducing LOS for inpatients. This Initiative arose from a series of meetings with decision makers, GIM physicians, nurses, allied health professionals and patient representatives to comprehensively catalogue GIM care processes for hospitalised patients, review best practices7 and develop a multipronged intervention targeting the various barriers to optimal care. This intervention addressed four key domains of improvement: (1) demand capacity realignment, (2) team integration and culture change, (3) best practice implementation and (4) transition optimisations. A fuller description of the intervention is provided in box 1 or from AC (senior author) upon request.
Description of General Internal Medicine (GIM) Care Transformation Initiative implemented at the University of Alberta Hospital
-
Demand capacity realignment: The optimal service bed base for GIM was defined through Canadian Institute of Health Information (CIHI) benchmarking (expected and average lengths of stay (LOSs)), and the most appropriate blend of care spaces was developed by adding a four-bed intermediate care space (for sicker patients), cohabiting all GIM patients on three contiguous wards (GIM patients were previously scattered across 11 different hospital wards on three floors of the hospital) and establishment of a 16-bed subacute ward (for patients no longer requiring acute medical care but requiring additional rehabilitation and convalescence prior to return to their former living arrangement).
-
Team integration and culture change: Clinical documentation was revised to permit and promote interprofessional collaboration (all healthcare providers charted in the same sections of hospital charts), daily rapid rounds were established to bring together the medical, nursing and paramedical teams to establish (and then monitor) the daily integrated care plan for each patient on each unit and a bed coordinator position (with links to various community resources) was added to coordinate discharge planning for all GIM patients.
-
Implementation of best practices: Processes were created to embed clinical practice guidelines (eg, care maps for pneumonia) and accreditation standards (eg, pre–intra–post-hospital medication reconciliation, venous thromboembolism prophylaxis, insulin protocols) into the ward care processes using preprinted admission order sheets and care maps and also to bring evidence-based resources to the point of care (using a GIM desktop on all ward computers which included evidence-based resources such as Evidence-Based Medicine, Dynamed, Critically Appraised Topics for common GIM diagnoses and clinical decision support tools).
-
Transition optimisations: Interprofessional teams were involved with each patient to define the optimal blend of services required to support safe, quality transitions back to each patient's prior living arrangements. In particular, the GIM Care Transformation Initiative focused on improving the medication reconciliation process at discharge, with involvement of a pharmacist and an emphasis on prompt communication of medication changes to outpatient physicians and pharmacists for each patient (via fax at time of hospital discharge of a Best Possible Medication Discharge List which included all discharge medications as well as the explicit rationale for changes from that patient's pre-discharge medication regimen).
The GIM Care Transformation Initiative was implemented at the UAH, but not the six other teaching hospitals in the Canadian province of Alberta, starting in October 2010 with completion by 31 March 2011. We took advantage of this natural experiment to evaluate the impact of the GIM Care Transformation Initiative on the efficiency of care (LOS)—the primary target of the Initiative. However, to assess safety of the system changes that were implemented and to measure any unintended consequences we also examined the quality of care delivered (using a composite proxy measure of ‘inpatient mortality during index hospitalisation or all-cause readmission/death within 30 days of discharge’ advocated in the Patient Protection and Affordable Care Act).
Methods
Setting and data sources
The Canadian province of Alberta has a single health authority and a vertically integrated government-funded healthcare delivery system that provides universal coverage to over 3.7 million people. All seven teaching hospitals in the province are located in the two large urban centres (four in Edmonton and three in Calgary). This study was approved by the Health Research Ethics Board at the University of Alberta and the need for patient-level informed consent was waived. De-identified linked data from the Alberta Health Discharge Abstract Database were collected for all acute care hospitalisations in Alberta, including the admission date, discharge date, hospital ward and attending physician, most responsible diagnosis (as specified by the hospital attending physician) and up to 24 other diagnoses. We also used data from the Alberta Health Care Insurance Plan Registry and the Ambulatory Care Database that capture emergency department (ED) visits.
Study cohort
We identified all adults with an acute care hospitalisation on the GIM services at the seven Alberta teaching hospitals between 1 October 2009 and 30 September 2010 (the 12 months before the GIM Care Transformation was implemented or PRE phase) and between 1 April 2011 and 31 March 2012 (the 12 months after the GIM transformation or POST phase). Patients from out of province or transferred from/to another inpatient service (eg, the intensive care unit, a different service in the same hospital (such as surgery), another acute care hospital or rehabilitation hospital) or with LOSs greater than 30 days were excluded and we only collected data for the first hospitalisation for any patient anywhere in Alberta during the study period (figure 1).
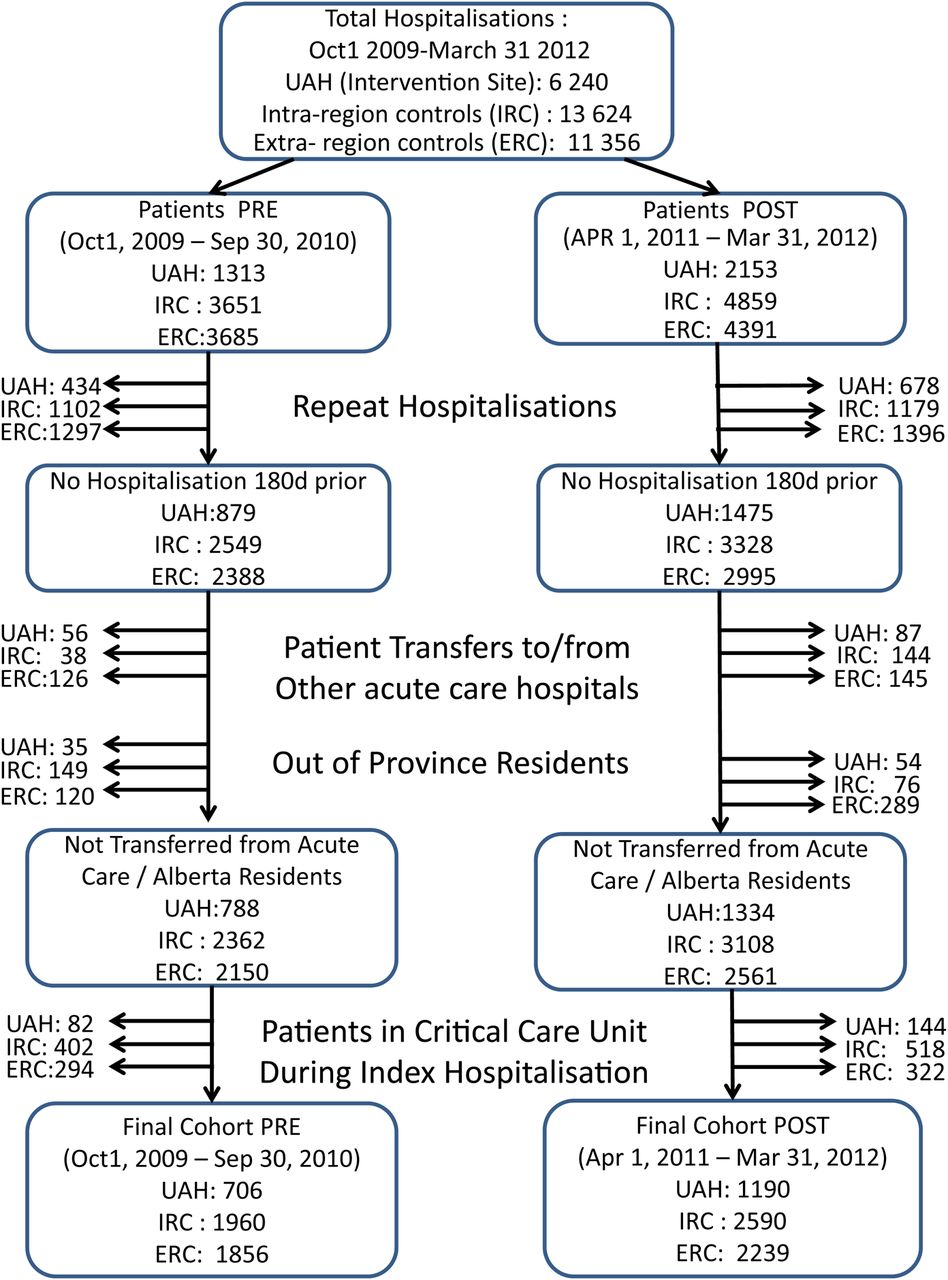
Derivation of study cohorts.
Design
We conducted a before–after study with concurrent controls using three mutually exclusive cohorts: patients hospitalised on the GIM service at the UAH (intervention site), patients hospitalised on GIM services at the other three teaching hospitals in Edmonton which did not implement the GIM Care Transformation Initiative (intra-regional controls, IRC) and patients hospitalised on the GIM services at the three teaching hospitals in Calgary which did not implement the GIM Care Transformation Initiative (extra-regional controls, ERC). The GIM services at all seven teaching hospitals in Edmonton and Calgary are structured similarly to each other (with Canadian Royal College of Physicians approved clinical teaching units run by attending staff and that include learners at multiple levels of training) and admit undifferentiated medical patients from the ED not requiring critical care or surgical interventions.
Covariates
Patient comorbidities were identified using International Classification of Disease (ICD)-9 and ICD-10 codes from the index and all other hospitalisations, ED visits or ambulatory care visits in the 12 months prior to their index admission, the accuracy of which have been previously validated in Alberta databases.8 ,9 We derived Charlson Comorbidity Index scores and also calculated the LACE score for each patient at the time of discharge from their index hospitalisation. LACE is a four-item score derived10 in a prospective cohort study in Ontario and subsequently validated in Alberta11 that incorporates LOS for the index hospitalisation (L), acuity of admission (A), Charlson comorbidity score (C) and emergency room utilisation in the prior 6 months (E) and can be used for risk adjusting outcomes in the first 30 days after hospital discharge.
Outcomes
As the GIM Care Transformation Initiative was designed to reduce LOS, our primary effectiveness outcome was LOS for the index hospitalisation (note that LOS included time spent on the subacute ward at the UAH for those who transitioned home via that unit). We also explored changes in LOS by using a difference-of-differences approach looking at the ratio between the observed LOS and the expected LOS for each patient over the study period (expected LOS was generated for each patient independently of our study using validated Canadian Institute for Health Information estimates which take into account case mix group, age and inpatient resource intensity weights—see http://www.cihi.ca). Expected LOS are data-driven estimates based on the most current 2 years of patient LOS information available in the Canadian Institute for Health Information Discharge Abstract Database for all acute hospitals in Canada.
Given that the Initiative targeted care during the index hospitalisation, we defined our main safety endpoint as the composite of ‘death during the index hospitalisation OR death/readmission within 30 days after discharge’. This composite endpoint was designed to deal with competing risks and broadly capture unintended consequences or harms related to the Initiative and can be risk adjusted using the LACE score.10 ,11 We also examined a number of secondary safety outcomes, including rate of mortality and/or readmission within 30 days of discharge after index hospitalisation in those who survived index hospitalisation, index hospitalisation death rates, discharge disposition after index hospitalisation and emergency room visits within 30 days post-discharge from index hospitalisation.
Analyses
We evaluated the impact of the GIM Care Transformation Initiative in a series of pre–post comparisons for patients hospitalised on GIM wards pre versus post the system changes at the UAH (intervention) versus six control sites. This essentially captures the difference-of-differences in changes of adjusted LOS over time and across sites. As multiple changes were made in rapid succession between October 2010 and March 2011, we were not able to evaluate the impact of particular elements of the GIM Care Transformation system redesign; in the parlance of time series, analyses were ‘interrupted’ during this period of rapid transitions. Specifically, we compared the outcomes in the cohort of patients hospitalised between 1 April 2011 and 31 March 2012 (defined as ‘POST-Initiative’) with those from the baseline (1 October 2009 to 30 September 2010) cohort (defined as ‘PRE-Initiative’) in multivariate hierarchical linear regression models (adjusting for covariates (see table 1) and controlling for site as a fixed effect). For dichotomous endpoints, we used the analogous approach in logistic regression.
Study cohort characteristics
Because time series with a control series constitutes one of the strongest designs available short of a randomised trial to evaluate health system changes, we also examined monthly event rates for the GIM wards at the UAH and the control hospitals from October 2009 to March 2012 and performed interrupted time series (ITS) analyses using autoregressive integrated moving average (ARIMA) models to account for temporal trends and to determine whether there were changes in outcomes at the UAH compared with the control sites associated with implementation of the GIM Care Transformation Initiative. Autocorrelation, partial autocorrelation and inverse autocorrelation functions were assessed for model parameter appropriateness and seasonality. Stationarity was assessed using the autocorrelation function and the augmented Dickey–Fuller test. The presence of ‘white noise’ was assessed by examining the autocorrelations at various lags, using the Ljung–Box χ2 statistic.
We undertook three preplanned sensitivity analyses. First, we reran all analyses after excluding those individuals admitted from or discharged to long-term care facilities. Second, in an attempt to create similar patient cohorts between hospitals, we examined the impact of the GIM Care Transformation Initiative in only those patients hospitalised with one of the five most common discharge diagnoses from GIM wards in Alberta. Third, we restricted our analysis to only those individuals admitted for ambulatory care-sensitive conditions (asthma, emphysema, chronic obstructive pulmonary disease (COPD), DM, epilepsy, heart disease or hypertension) as the most responsible diagnosis. All statistical analyses were done using SAS V.9.3 (Cary, North Carolina, USA) and R V.2.15.1 (Vienna, Austria).
Results
Between 1 October 2009 and 30 September 2010 (PRE-Initiative), 706 patients were hospitalised at least once on GIM wards at the UAH, 1960 on GIM wards at the other three Edmonton teaching hospitals at least once and 1856 at the three Calgary teaching hospitals. Between 1 April 2011 and 31 March 2012 (POST-Initiative), 1190 patients were hospitalised at least once on GIM wards at the UAH, 2590 at the other three Edmonton teaching hospitals and 2239 at the three Calgary teaching hospitals (figure 1). GIM patients at the UAH and the IRC hospitals were comparable in terms of age, sex, comorbidity and resource intensity weights (table 1). However, patients hospitalised on GIM wards at the ERC hospitals were younger and had significantly less comorbidity and lower resource intensity weights than the UAH and the IRC (table 1). The most common responsible diagnoses in the GIM wards of all seven Alberta teaching hospitals were COPD, pneumonia, heart failure, urinary tract infections and venous thromboembolism (table 1).
Changes in LOS (effectiveness)
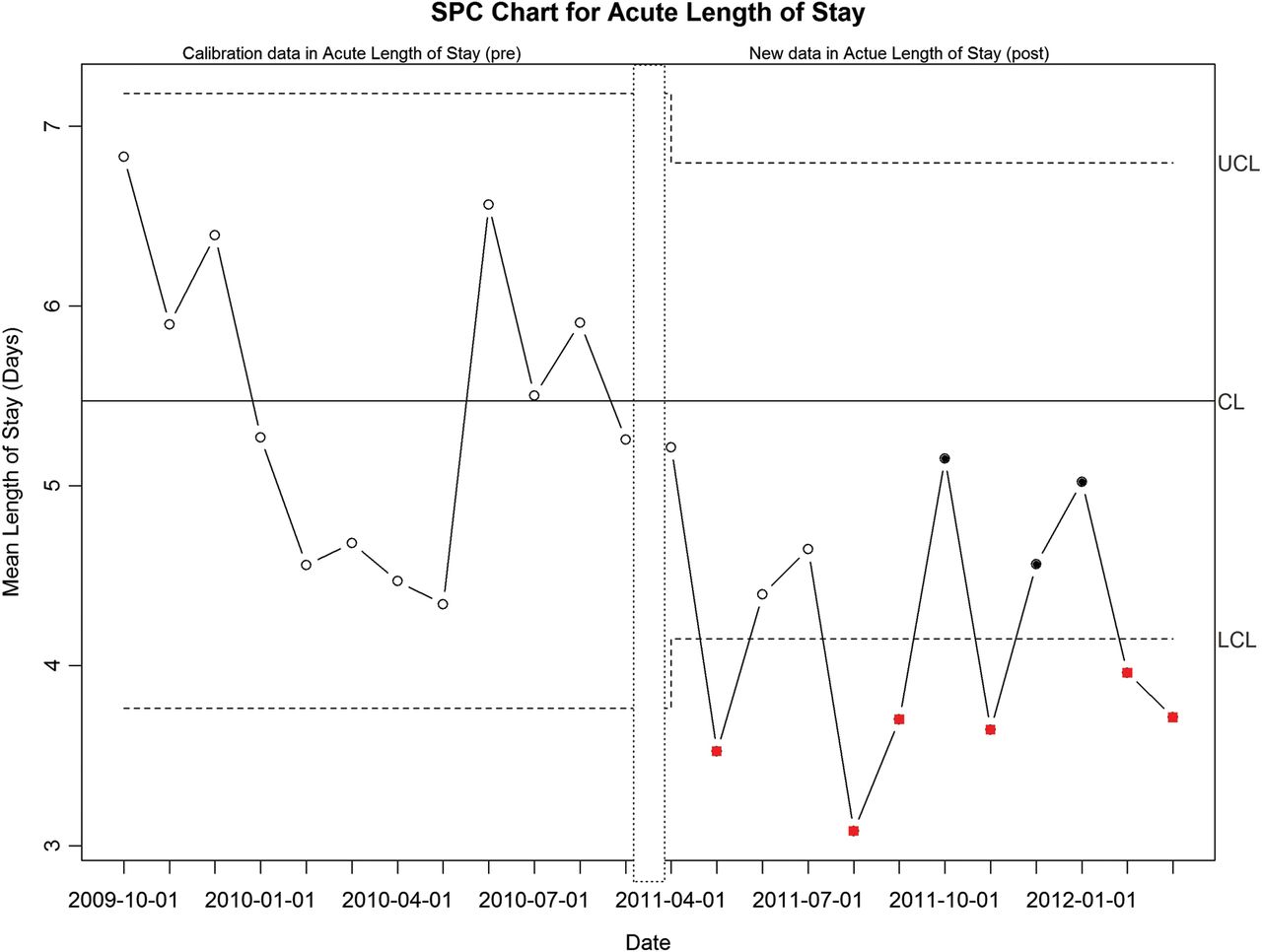
Before the Initiative, the mean-adjusted LOSs for patients hospitalised on GIM wards were 7.04 (95% CI 6.65 to 7.43) days at the UAH, 9.30 (95% CI 9.10 to 9.50) days at the IRC and 7.17 (95% CI 6.97 to 7.38) days at the ERC (figure 2). Crude, adjusted and observed versus expected ratios for LOS decreased over time in all seven teaching hospitals (figure 2, table 2)—as a result, the number of patients occupying the bed base was greater in the POST period than the PRE period. Over and above these secular trends (on average a 0.68 (95% CI 0.45 to 0.91) day decline in Alberta GIM Teaching hospitals), implementation of the GIM Care Transformation Initiative at the UAH was associated with an additional decline in adjusted LOS of 0.75 (95% CI 0.28 to 1.29) days which was statistically significant (p=0.003 for level change on ITS)—this represents a 20% relative reduction in LOS at the UAH after implementation of the GIM Care Transformation (adjusted LOS declined by 1.43 (95% CI 0.94 to 1.92) days POST-intervention vs PRE-intervention). Statistical process control charting confirmed that the changes in LOS at the UAH were statistically significantly greater than expected given the secular trends seen in the pre-intervention phase (figure 3). There was no level change in the adjusted LOS for the IRC (p=0.37) or the ERC (p=0.45) between the POST-intervention versus PRE-intervention time frames. Furthermore, while the ratio of observed:expected LOS fell in all three comparison groups POST-intervention versus PRE-intervention, the ratios remained significantly above 1.0 in both the IRC and ERC while it declined significantly below the expected LOS only at the UAH intervention site (table 2).
Outcomes during the index hospitalisation and in first 30 days after discharge
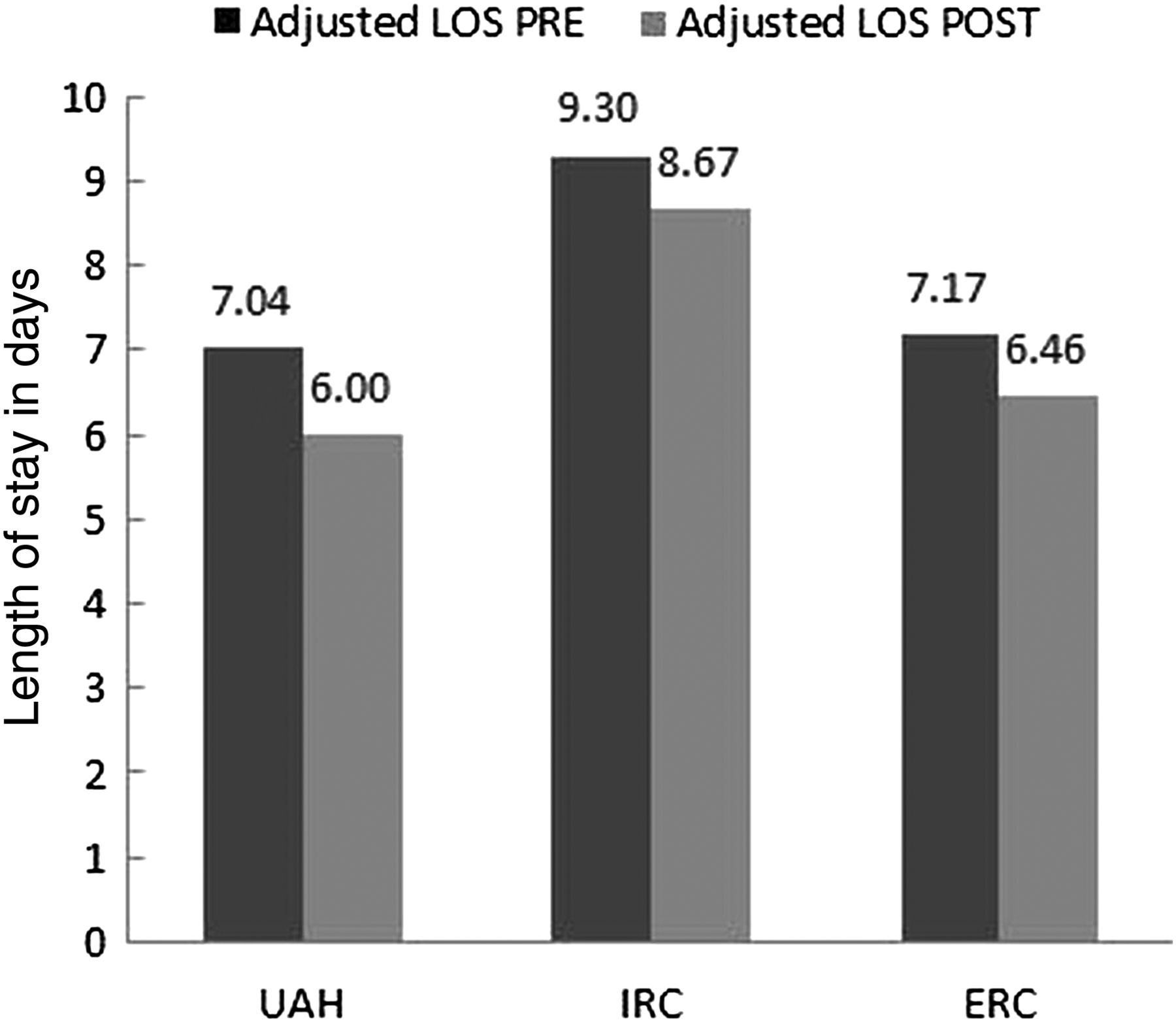
Adjusted length of stay (LOS) pre and post the General Internal Medicine Care Transformation Initiative at the University of Alberta Hospital (UAH), intra-region controls (IRC) and extra-region controls (ERC). IRC, intra-region controls (Edmonton hospitals); ERC, extra-region controls (Calgary hospitals).

{kind=link}
{kind=link}
{kind=link}
Statistical process control (SPC) chart for mean length of stay (LOS) on General Internal Medicine (GIM) wards at the University of Alberta Hospital before and after the GIM Care Transformation Initiative. The SPC chart provides the mean LOS and two sigma control limits (based on the monthly average for patients in each era) calibrated during the ‘pre’-Care Transformation phase and then plotted for the post-Care Transformation era. The squares indicate points that are below the control limits set during the pre-phase. The dots indicate deviation from the prior statistical pattern (at least seven sequential points below the mean). The narrower control limits in the post-phase are the result of the increased patient throughput in the post-time period. LCL, lower confidence limit; UCL, upper confidence limit.
Changes in discharge outcomes (safety)
Patients hospitalised in the POST-intervention time frame at the UAH, compared with patients hospitalised during the PRE-intervention time frame, exhibited no substantial change in the rates of our prespecified safety endpoint of ‘index hospitalisation mortality or all-cause death/readmission within 30 days of discharge’ (17.8% POST vs 18.4% PRE, adjusted OR 1.02, 95% CI 0.80 to 1.31, p=0.94 for level change on ITS, table 2). While rates of the composite safety endpoint did not appreciably change in the IRC hospitals (aOR 1.04, 95% CI 0.89 to 1.22, p=0.33 on ITS), rates at the ERC hospitals increased significantly over the duration of the study (15.9% vs 14.5%, aOR 1.21, 95% CI 1.01 to 1.45), although it was not significant on ITS (p=0.73).
There was no change in index hospitalisation mortality rates at the UAH (4.37% post vs 4.67% pre, aOR 0.93, 95% CI 0.60 to 1.46 and p=0.94 on ITS) and no change in the proportion of patients who were discharged back to the same level of care they were at prior to admission (92.09% vs 89.90%, aOR 1.13, 95% CI 0.84 to 1.52). In-hospital mortality and discharge disposition were also not significantly different in either the IRC sites or the ERC sites in the POST-intervention time frames compared with the PRE-intervention time frames (table 2). After implementation of the GIM Care Transformation Initiative, there were small declines in the proportion of patients who had an outpatient physician visit (and their average frequency) at the UAH but not at the ERC or IRC (table 2).
ITS with adjustment for secular trends, seasonal variation and case mix confirmed that all-cause hospital readmissions or ED visits within 30 days of discharge were not significantly different in the POST-time frame than in the PRE-time frame at either the UAH (p=0.71 and 0.16, respectively), the IRC (p=0.33 and 0.70) or the ERC (p=0.73 and 0.43).
Sensitivity analyses
Our preplanned sensitivity analyses yielded similar results. For example, among patients hospitalised with any of the top five diagnoses, there were no significant changes in adjusted LOS at either the IRC or the ERC POST-intervention versus PRE-intervention (table 2), while the adjusted acute LOS at the UAH declined after the GIM Care Transformation Initiative by 1.35 days (95% CI 0.48 to 2.22 days) without any apparent excess risk of harm (aOR 0.84, 95% CI 0.55 to 1.28, for ‘in-hospital death or death/readmission’ within 30 days of discharge). Similarly, excluding residents of long-term care facilities confirmed that implementation of the GIM Care Transformation Initiative was still associated with a decline in adjusted acute LOS of 1.39 (95% CI 0.93 to 1.86) days at the UAH (p=0.004 on ITS)—this represents a 25% relative reduction in LOS for community-dwelling patients—without evident harm (aOR 0.96, 95% CI 0.67 to 1.34, for our composite primary safety outcome). Finally, results were similar when the analysis was restricted to those with an ambulatory care-sensitive condition as the most responsible diagnosis for their index hospitalisation: the adjusted LOS was reduced by 1.34 days in those hospitalised at the UAH (95% CI 0.49 to 2.19 day reduction) and the aOR was 0.83 (95% CI 0.49 to 1.41) for ‘in-hospital death or death/readmission’ within 30 days of discharge.
Discussion
We observed powerful secular trends suggesting that the efficiency of GIM hospital care in Alberta teaching hospitals has improved over time. Above and beyond these secular trends, in a controlled natural experiment, we found that the GIM Care Transformation Initiative reduced adjusted LOS by a further 20% without increasing index hospitalisation mortality rates or 30 -day rates of readmission, mortality or ED visits after discharge.
Observational studies in both the USA and Canada have reported conflicting results on whether shorter LOSs are associated with poorer post-discharge outcomes.12–21 Our study adds to this evidence base by demonstrating that an intervention that reduced LOS for hospitalised GIM patients did not adversely impact their post-discharge outcomes (at least using quality proxies endorsed within the Patient Protection and Affordable Care Act and by the Centers for Medicare & Medicaid Services).5 ,6 In fact, we had 95% power to detect a 20% relative difference in our composite safety endpoint (in-hospital mortality or death/readmission within 30 days of discharge), a difference deemed clinically important by planners for the Centers for Medicare & Medicaid Services.5 ,6 Our findings are consistent with a recent report that the 27% relative reduction in LOS achieved in Veterans Affairs hospitals between 1997 and 2010 was not associated with an upswing in 30 -day mortality or risk-adjusted readmission rates.12 However, while the Veterans Affairs analyses suggested that hospitals with lower than expected LOS had higher readmission rates, the UAH (our intervention site) had an observed:expected LOS ratio that was reduced to 0.8 but without worsening of post-discharge event rates compared with control teaching hospitals.
A distinct advantage of our study is our ability to capture all re-admissions to any hospital in Alberta for any reason. While some may question the generalisability of our findings beyond Alberta, perusal of our sociodemographics, most common admitting diagnoses, case mix, in-hospital mortality and post-discharge readmission rates reveals that Alberta hospitals are comparable with most hospitals elsewhere in Canada and the USA.3 ,4 ,12–15 Thus, we believe the benefits we observed with the GIM Care Transformation Initiative would be translatable to other jurisdictions.
There are some limitations to our study. First, the use of administrative data meant that we could not capture important clinical data such as severity of disease and functional capacity. However, in our analysis of outcomes in the first 30 days after discharge we adjusted for the LACE score for each patient, an index which incorporates length of index hospital stay and number of prior visits to the ED (proxy markers for frailty) and has been shown to be the best predictor of adverse events in the first 30 days after discharge.10 ,11 Second, the GIM Care Transformation Initiative targeted all patients hospitalised on the UAH GIM wards, not just those perceived to be at ‘high risk’ of readmission, and this may have reduced the potential impact of the programme—however, we felt this necessary since neither experienced clinicians nor researchers using rigorously developed data-rich algorithms can accurately predict which patients will bounce back to the hospital and which will successfully transition back into the community.13 ,14 ,22 ,23 Third, we did not collect detailed process-of-care measures such as prescribing or diagnostic testing data to explore changes in the quality of care and instead used post-discharge outcomes as a proxy for quality of care. Fourth, we deliberately chose only one hospitalisation for each patient as prior work has established that risk adjustment models perform best with single admissions per patient.24 Whether the Care Transformation Initiative would have more or less impact in patients who are frequently rehospitalised is a separate research question which we plan to evaluate in subsequent studies. Finally, we examined all-cause readmissions rather than ‘preventable’ readmissions—we recognise that only a minority of all readmissions are truly preventable25 and that not all readmissions should be viewed as evidence of poor quality of care,26 ,27 but there are currently no validated algorithms to define which readmissions are preventable using administrative data alone. However, our sensitivity analysis confirmed that our results were similar when the analysis was restricted to those hospitalised with an ambulatory care-sensitive condition.
The key limitation of our study is our inability to isolate which element(s) of the Care Transformation Initiative drove the reduction in LOS since all Care Transformation elements were rolled out in such close temporal proximity. Surveys of 84 healthcare providers working on the GIM wards at the UAH (Gibbons-Reid V, Williams U and Dhingra S for Survey & Evaluation Services, Alberta Health Services. Final Evaluation Report for the GIM UAH Care Transformation Project Phase I. September 2011) and semistructured interviews with focus groups involving over 180 healthcare providers working on affected wards (Madsen K, Parajulee A, Spaling M, et al for Survey & Evaluation Services, Alberta Health Services. Final evaluation of Care Transformation. 27 April 2013) attributed the benefits largely to cohorting of GIM patients on dedicated wards and daily rapid rounds (attended by all members of the healthcare team and discharge coordinators to discuss discharge planning for each patient). While prior to October 2010 only 53% of GIM patients were admitted to ‘GIM wards’ and discharge planning rounds occurred once a week on the GIM wards (and never occurred on the off-service wards), by July 2011 97% of GIM patients were admitted to ‘GIM wards’ with discharge planning rounds occurring 5 days a week (Gibbons-Reid V, Williams U and Dhingra S for Survey & Evaluation Services, Alberta Health Services. Final Evaluation Report for the GIM UAH Care Transformation Project Phase I. September 2011). Copies of these Alberta Health Services reports are available from the senior author (AC) on request. However, given the disappointing results for cohorting on dedicated wards recently reported from an academic medical centre in the USA (longer LOS despite—or perhaps because of—more daily patient encounters, and no impact on readmissions in a controlled before–after study),28 further evidence (ideally in the form of a randomised trial) is required before concluding that cohorting alone can improve efficiency on GIM wards.
While various interventions have been proposed to improve the efficiency and quality of inpatient care, with inconsistent results when rigorously evaluated,7 the GIM Care Transformation Initiative did decrease LOS for hospitalised GIM patients above and beyond existing secular trends in teaching hospitals without increasing post-discharge adverse events. Given the nature of healthcare funding where increasing spending in one area can only occur if resources are shifted from other areas, there are potential opportunity costs with any intervention and it is important to ensure that improvements in efficiency measures (such as LOS) do not result in worsening quality metrics (such as post-discharge events). In a recent editorial, Dr Mitchell Katz highlighted the paucity of research in this area and asked ‘Is it even possible to decrease hospital costs while maintaining quality?’2 We believe the GIM Care Transformation Initiative answers Dr Katz's question. Efforts are now underway to roll out the Care Transformation Initiative at the other teaching hospitals in Alberta and in other clinical domains (with evaluation) and a formal cost-effectiveness analysis of the Care Transformation Initiative is being performed.
Acknowledgments
This study is based in part on data provided by Alberta Health to Alberta Health Services Data Integration, Measurement, and Reporting Branch. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta nor Alberta Health Services. None of the Government of Alberta, Alberta Health, nor Alberta Health Services expresses any opinion in relation to this study. FAM had full access to all the data used for this study and takes responsibility for the analysis and interpretation.
References
Footnotes
-
Contributors FAM, RSP, SRM and AC designed the study; FAM, JAB, MB, AC and SD acquired the data; JAB did the analyses; all authors were involved in interpretation of the data; FAM wrote the first draft of the paper and all authors were involved in revisions and approving the final manuscript for publication. FAM is guarantor for the manuscript.
-
Funding This study was supported by operating grants from the Canadian Institutes of Health Research (reference number 122168) and Alberta Innovates—Health Solutions. None of the funding agencies had any input into design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript. FAM and SRM hold career salary support from Alberta Innovates—Health Solutions. FAM holds the Capital Health/University of Alberta Chair in Cardiovascular Outcomes Research. SRM holds the Endowed Chair in Patient Health Management from the Faculties of Medicine and Dentistry and Pharmacy and Pharmaceutical Sciences, University of Alberta.
-
Competing interests None.
-
Ethics approval University of Alberta Health Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.