Article Text

Abstract
Background Situation awareness (SA)—the perception of data elements, comprehension of their meaning and projection of their status in the near future—has been associated with human performance in high-risk environments, including aviation and the operating room. The influences on SA in inpatient medicine are unknown.
Methods We conducted seven focus groups with nurses, respiratory therapists and resident physicians using a standardised semistructured focus group guide to promote discussion. Recordings of the focus groups were transcribed verbatim, and transcripts were qualitatively analysed by two independent reviewers to identify convergent and divergent themes.
Results Three themes emerged: (1) team-based care, (2) availability of standardised data and (3) standardised processes and procedures. We categorised these into social, technological and organisational influences on SA. Subthemes that emerged from each focus group were shared language to describe at-risk patients, provider experience in critical care/deterioration and interdisciplinary huddles to identify and plan for at-risk patients. An objective early warning score, proactive assessment and planning, adequate clinician staffing and tools for entering, displaying and monitoring data trends were identified by six of seven groups. Our data better reflected the concepts of team SA and shared SA than individual SA.
Conclusions Team-based care and standardisation support SA and the identification and treatment of patient risk in the complex environment of inpatient care. These findings can be used to guide the development and implementation of targeted interventions such as huddles to proactively scan for risk and electronic health record displays of data trends.
- Patient Safety
- Communication
- Hospital Medicine
- Safety Culture
- Teamwork
Statistics from Altmetric.com
Background and significance
Healthcare delivery at the frontlines is complex, involving non-linear work with constant interruptions, uncertain goals and communication challenges, making it both critical and difficult for clinicians to maintain situation awareness (SA).1 SA is (1) the perception of data elements, (2) the comprehension of their meaning in context and (3) the projection of their status in the near future.2 ,3 Poor SA, particularly in dynamic, high-risk industries like healthcare, has been associated with error and accidents.2–4 SA guides decision making, and poor SA is associated with reports of critical incidents in the intensive care unit (ICU) and errors during laparoscopic surgery.5 ,6 Models of SA in healthcare are particularly mature in anaesthesia and simulation where increased experience is associated with better SA.7–10 Concepts of SA have been extended to address individual SA, team SA, shared SA and distributed SA (box 1).3 ,7 ,11
Definitions for and examples of related types of situation awareness (SA)
Individual SA: An individual's perception of data elements, the comprehension of their meaning in context and the projection of their status in the near future. Example: A physician determines that fever, tachycardia and symptoms of acute respiratory distress syndrome are due to severe sepsis with a high risk of rapid deterioration.
Team SA: The degree to which every team member possesses the SA required for his or her responsibilities. Example: Each member of trauma team has a clearly defined role such that the person in charge of obtaining intravenous access has data to support that task but may not be aware of airway status.
Shared SA: The degree to which team members have the same SA on shared SA requirements. Example: Both the surgeon and the anaesthesiologist recognise hypotension as a potential sign of a life-threatening bleed so that each can make decisions and attend to treatments to address.
Distributed SA: Developing and maintaining an overall dynamic awareness of the situation based on perceiving the elements of the theatre environment: patient, team, time, displays and equipment, understanding what they mean and thinking ahead about what could happen in the near future. Example: In the intensive care unit a nurse titrates a dopamine infusion through observing the changing arterial line blood pressure and waveform on the monitor. The monitor influences her understanding of the situation and her actions in real time.
At our centre, we determined that poor SA was the cause of almost half of all serious safety events and floor-to-ICU transfers in our hospital.12 ,13 A multidisciplinary expert panel determined this through a 3-meeting root cause analysis process developed by Healthcare Performance Improvement.12 ,14 Examples of poor SA included the clinical team not perceiving data elements such as an elevated heart rate and not putting such elements in context to form a diagnosis of shock. These findings led us to design a proactive system, including individual-level and organisational-level interventions to enhance SA which have reduced the incidence of serious safety events and unrecognised clinical deterioration.13 ,15 The model in figure 1 illustrates how improved clinician SA facilitates better identification of risk which is then tied to developing clear mitigation and escalation plans.
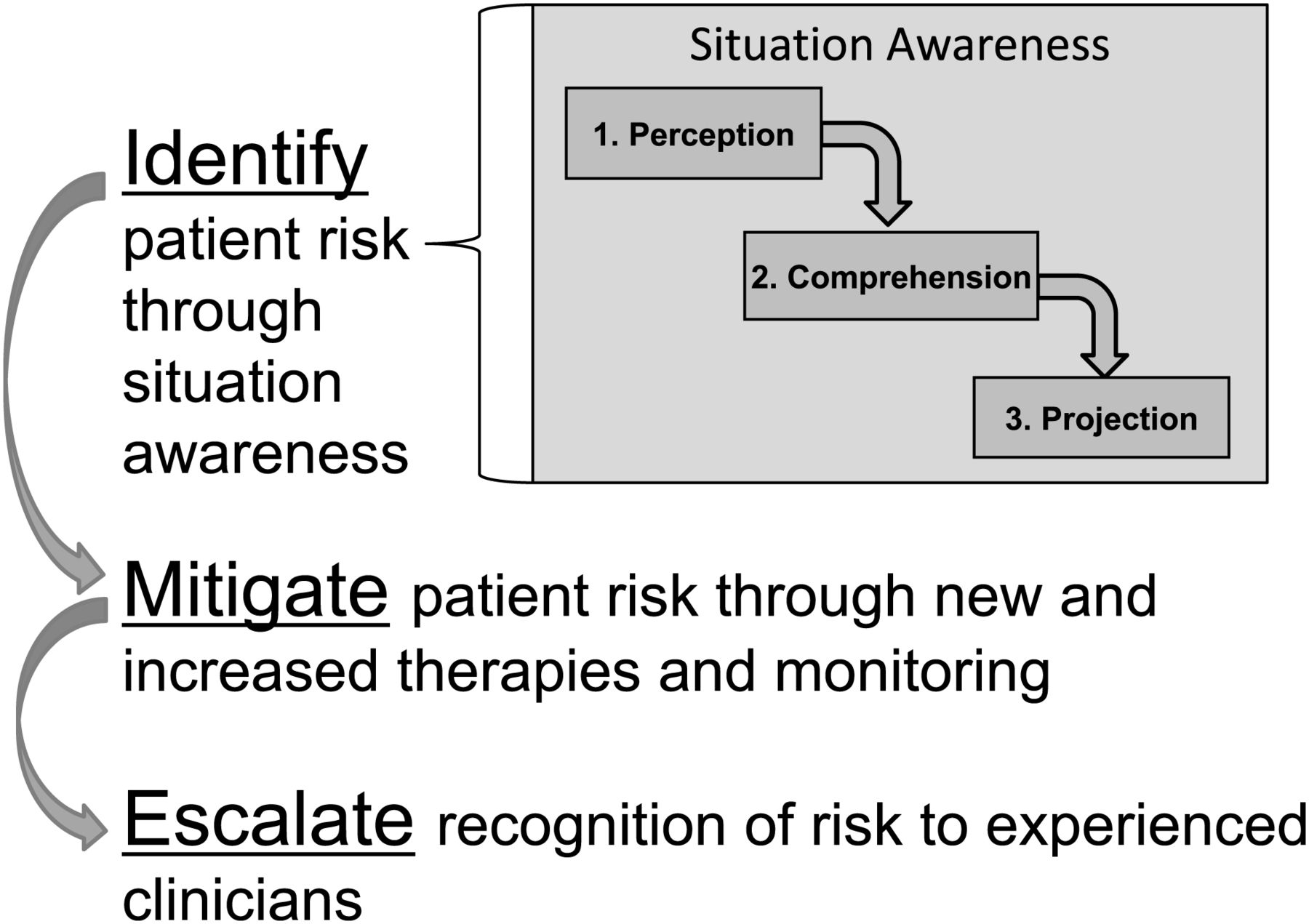
Diagram of the conceptual model of relationship between situation awareness and identifying, mitigating and escalating the recognition of patient risk.
While the SA-related healthcare literature pertaining to the inpatient setting is limited, several qualitative studies have examined why clinicians fail to escalate care to rapid response teams or medical response teams (MRTs) that identify and rapidly intervene on deteriorating patients.16–19 In one study several sociocultural issues were identified, including the belief that the situation was under control, that no ICU beds were available and that there was poor communication among team members.16 Contextual factors, including leadership, organisational culture and training, have been found to either facilitate or hinder MRT implementation.17 We found no studies that examined the barriers and enablers for identifying and mitigating patient risk before escalation through MRT activation.
The goal of this study was to learn more about factors that influence a front-line healthcare providers’ ability to achieve and maintain SA and to identify, address and escalate the recognition of risk for patients in the inpatient setting.
Methods
Setting
Cincinnati Children's Hospital Medical Center (CCHMC) is a 523-bed academic, freestanding children's hospital. The MRT process was first tested and spread in 2006,20 and a Paediatric Early Warning Score (PEWS) was introduced in 2007.21 Improvement work to increase SA and decrease unrecognised clinical deterioration began in 2009.7
Study design
We used a qualitative study design that allowed us to go into more depth about the issues under investigation.
This study was deemed exempt by the CCHMC institutional review board since it was part of an overall quality improvement effort and no identifying information was collected.
Participant recruitment
Targeted study participants included inpatient charge and bedside nurses, respiratory therapists (RTs) and senior paediatric residents. At our hospital one charge nurse is present on each inpatient unit. This nurse does not have patients of her or his own and supervises the bedside nurses with a focus on new admissions, discharges and the sickest patients. Email and hard copy invitations were sent to approximately 700 inpatient charge and bedside nurses and RTs. We spoke with clinical directors, attended morning huddles and resident conferences and posted flyers in high-visibility areas such as conference rooms, staff bathrooms and the resident lounge to enhance recruitment. Follow-up emails were sent to all interested individuals to schedule the focus groups.
Data collection
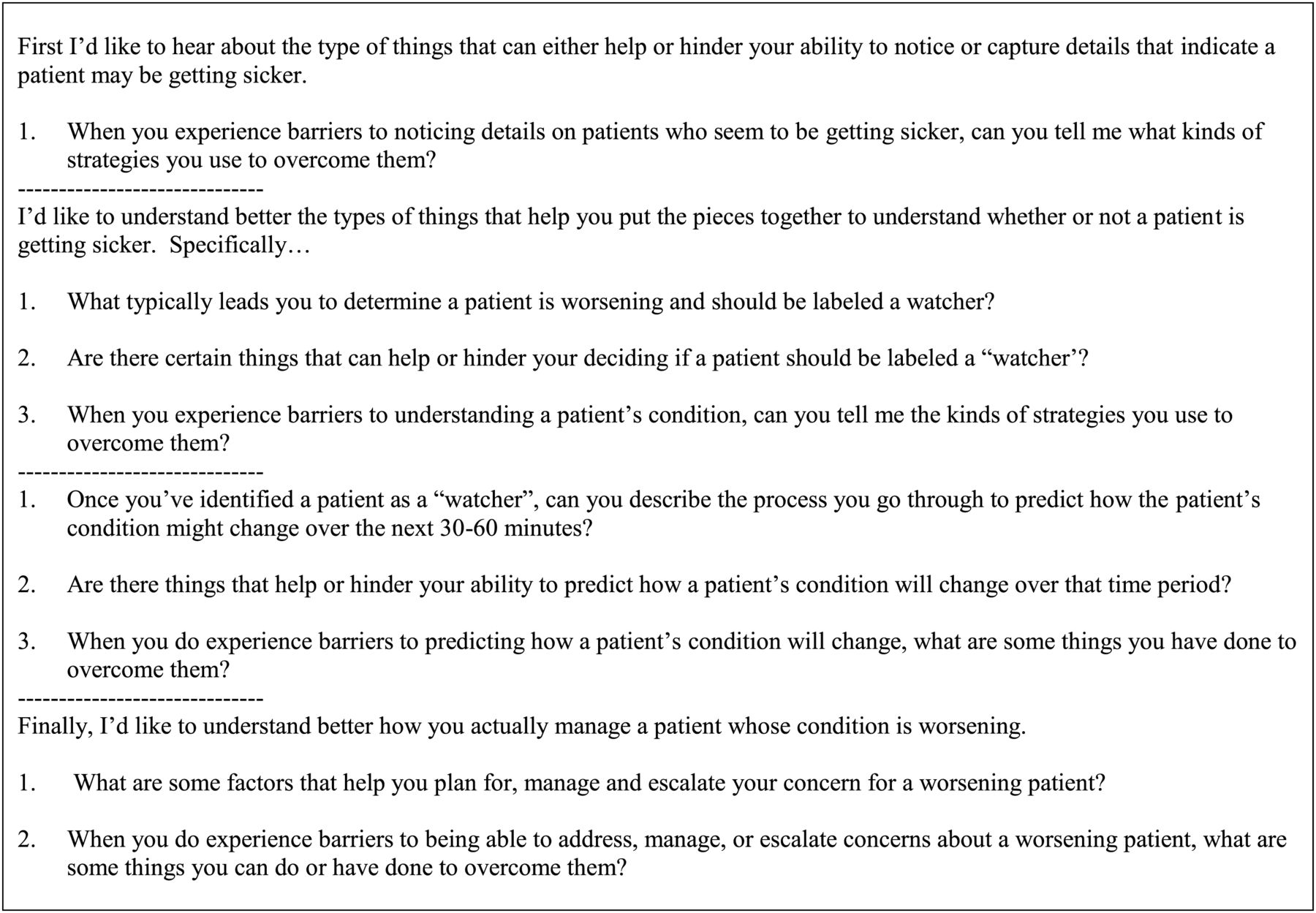
To encourage honest and open dialogue, participants were assigned to a group based on their role (eg, charge nurse, resident). We developed and used a semistructured focus group guide that included open-ended questions about the enablers and barriers to achieving the three levels of SA-related identification of risk as well as enablers and barriers to mitigating and escalating recognition of the identified risk (figure 1). The guides were pretested and revised with a small sample of representative participants (figure 2). Participant demographic and experience data were also collected. A trained facilitator led the 1-h sessions, which were digitally recorded and transcribed verbatim.
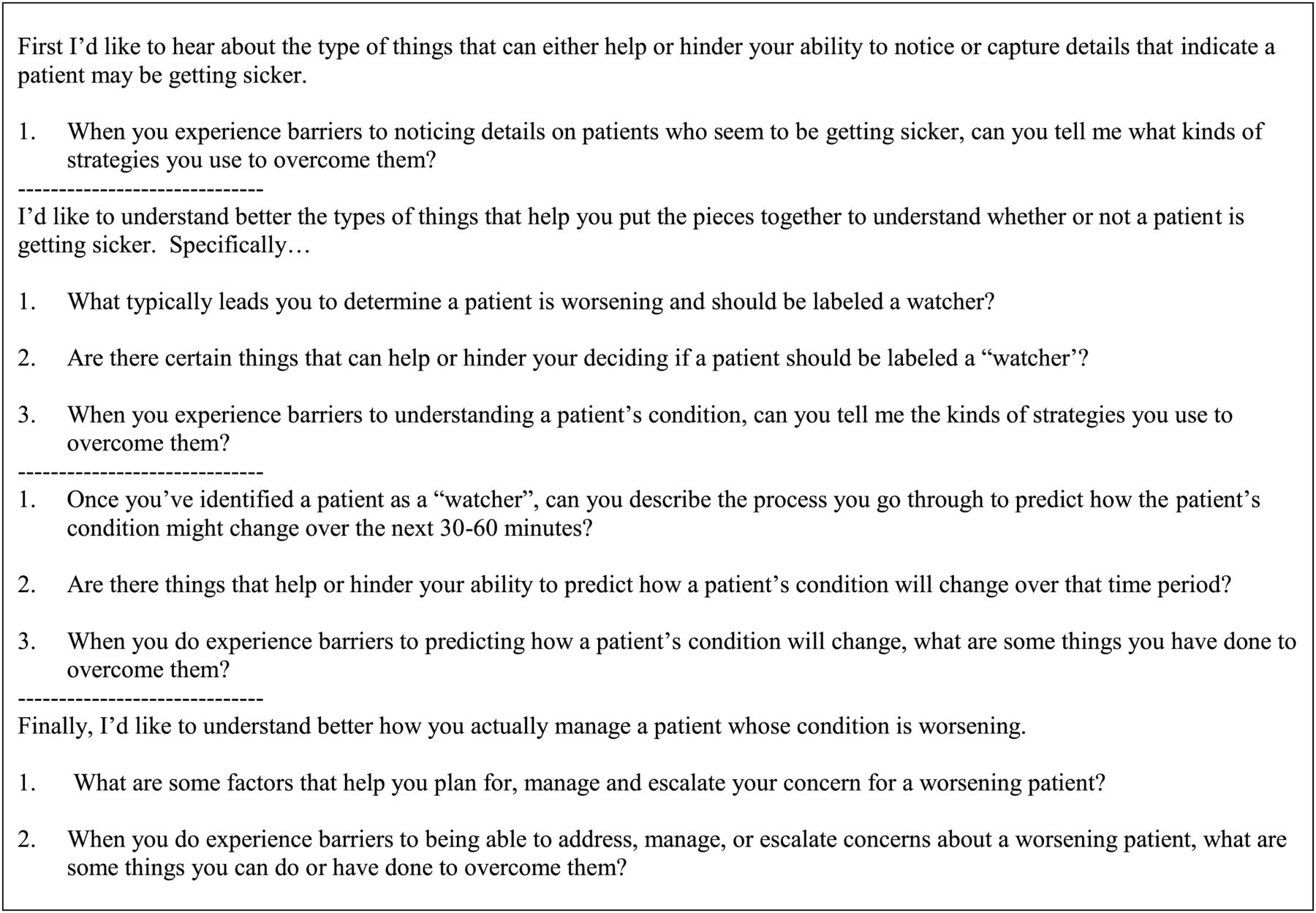
Semistructured focus group guide.
Analysis
We analysed the transcripts using a constant comparison approach.22 Beginning with one charge nurse and one bedside nurse transcript, we independently coded participant comments that reflected issues pertaining to a clinician's ability to identify (perceive and understand data elements), mitigate (predict, plan or act to treat patient deterioration) or escalate (involve more experienced clinicians often from outside the unit) the recognition of patient risk. After comparing, discussing and resolving coding differences, we incorporated the final codes into an initial codebook which we used to analyse subsequent transcripts, adding or altering codes as needed. The final codebook included codes (themes) and subcodes (subthemes), and dimensions that reflected the most frequently expressed influences on achieving SA and to identifying (I), mitigating (M) and escalating (E) the recognition of patient risk.
Results
Participants
A total of 31 inpatient providers participated in the focus groups: 10 charge nurses, 8 bedside nurses, 3 RTs and 10 second-year or third-year residents. This resulted in three charge nurse groups (n=3, 3, 4), three bedside nurse/RT groups (n=3, 3, 5) and one resident (n=10) focus groups. Over half of the nurse/RT participants had 10 or more years of experience (table 1) and 33% had worked at CCHMC for over 20 years. Participants represented 16 of the 20 inpatient units; 81% had been on their current unit for five or more years.
Years of experience for nurse and RT participants
Themes, subthemes and dimensions
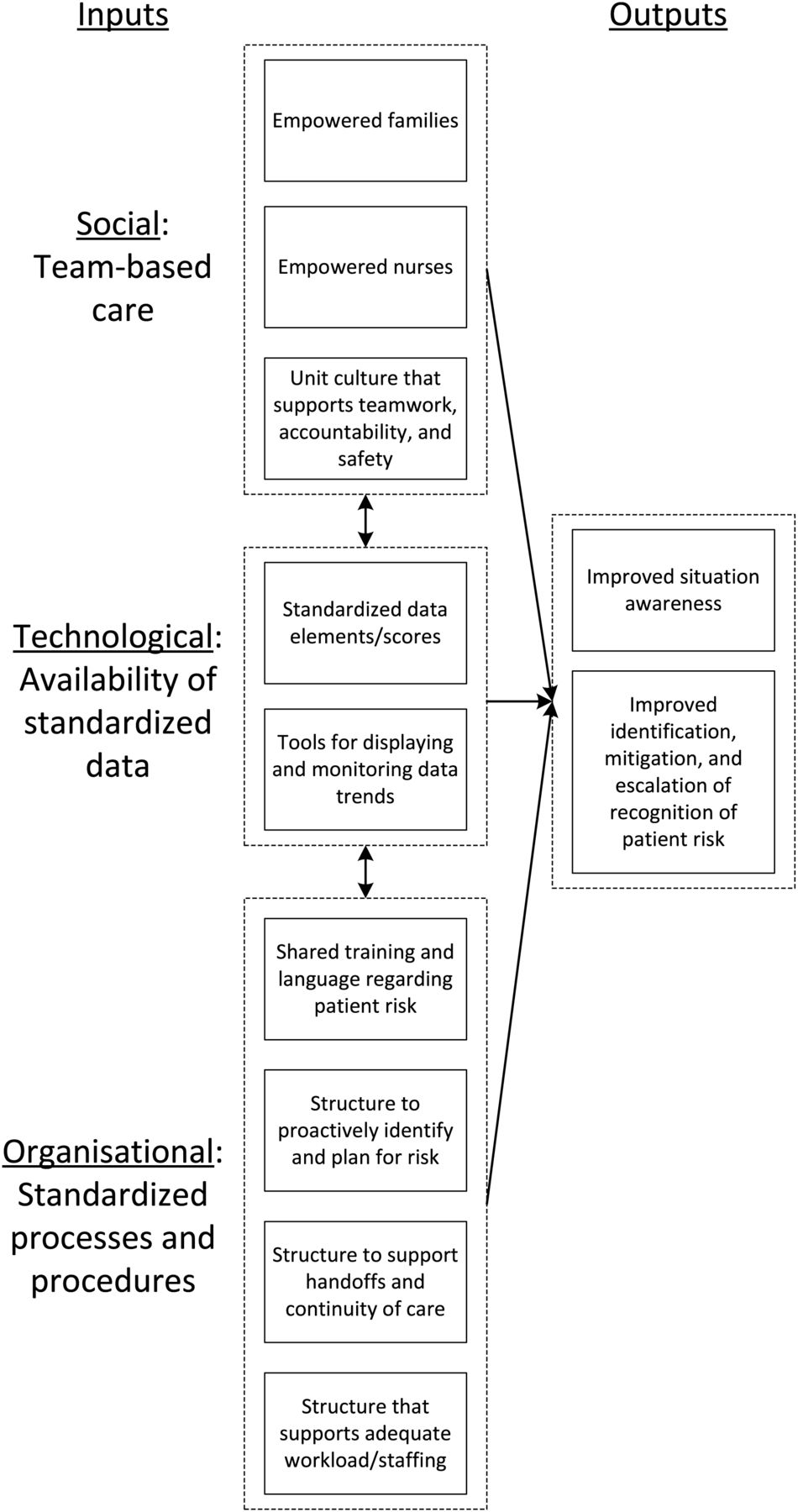
Three overarching themes and nine related subthemes emerged from the data, including (1) team-based care (family empowerment, nurse empowerment, unit culture that supports teamwork, accountability and safety), (2) availability of data (standardised data elements/scores, tools for entering, displaying and monitoring data and data trends) and (3) standardised processes and procedures (shared training and language regarding patient risk, structure to proactively identify and plan for risk, structure to support handoffs and continuity of care and structure that supports adequate workload/staffing). We then determined that each of these themes and subthemes could be categorised as being either a social, technological or organisational system input that influenced the achieving of SA and identifying, mitigating and escalating the recognition of patient risk (figure 3).
{kind=link}
{kind=link}
{kind=link}
Model of inputs for output of improved situation awareness and identification, mitigation and escalation of recognition of patient risk.
Table 2 is a pictorial representation of the final themes, subthemes and the most frequently mentioned dimensions comprising them.
Relative frequency that themes, subthemes and underlying dimensions were discussed in the focus groups
A brief description of each model input, theme and related subthemes, along with illustrative quotes is presented below.
Social
Team-based care
This theme comprised three somewhat overlapping subthemes of empowerment and culture. The influences on family empowerment pertained to healthcare providers listening to and engaging family members in their child's care and also giving families power to escalate their concerns to a higher level if they felt those expectations were not being met (I, M, E).
I like the signs [about family MRT activation] in the rooms. It makes the family…start questioning more things about their kid. (Bedside nurse)
Nurse empowerment influences included having a powerful, equal and welcomed voice in huddles and within the patient care team. This voice supported their reporting of patient-related observations, questioning of proposed plans and suggesting of alternate plans (I, M). There was also the expectation that any provider can go up the chain of command and escalate a situation (ie, call an MRT) if they felt their voice was not being heard or if they disagreed with the plan (E).
I don’t let people off the phone with me until I know what their plan is or, if they don’t know that, they’re coming to the bedside. (Bedside nurse)
The most often mentioned negative influence on nurse empowerment was the fear of speaking up and/or being wrong in front of peers, supervisors and physicians (M, E).
Participants noted that a unit culture that supports teamwork, accountability and safety would support trusting relationships, encourage communicating with all team members (including the ICU team) and encourage a willingness to ask for second opinions (I). Also this culture would require all providers to be accountable for their role in carrying out mitigation plans (M) and escalating patient care if necessary (E).
I feel like nursing, in particular, helps us gauge who we need to direct our attention to …because you know they're constantly around the patients. …they have a pretty good idea of what the patient was like when they first came in or whether or not they're rapidly changing. The communication between us and the nurses is essential. (Resident)
Negative influences on successful mitigation included disagreements about plans among team members and lack of collegiality/teamwork—specifically, physicians not listening to/taking nurse input seriously. Additionally, the lack of familiarity with and trust of team members on the MRT can result in limited input, condescension/intimidation, potential stigma and lack of agreement (E).
Technological
Availability of standardised data
Given the nature of this theme (ie, using data to assess a patient's status), it is not surprising that we found codes associated only with the identification of patient risk. Specifically, the influences associated with the standardised data elements/scores subtheme relate to the benefit of objective algorithms, such as the PEWS, and other standardised tools for conducting patient assessment.21 In addition to the ‘gut feeling’ participants described having when they see a patient deteriorating, these methods and tools provided a comprehensive patient picture that they could more easily share with the other providers.
…the use of the PEWS score actually helps. It's an objective kind of assessment and, if you compare the scores, you can kind of see the trend. (Charge nurse)
In contrast, it was also noted by many of the participants that the objective algorithms were not used in a standardised manner across units or providers, thereby limiting their effectiveness. The other negative influence mentioned was that the algorithms were not applicable for use with certain patient populations because, for example, a high PEW score could actually be a baseline score for certain patients.
The influences associated with the tools for entering, displaying and monitoring data and data trends subtheme pertained to how the task of identifying and monitoring a deteriorating patient had been made easier with the implementation of the electronic health record system and its ability to display data over time. A limitation often mentioned, though, was that nurses, RTs and doctors chart their information differently and in different places, making it more difficult to share patient information.
Organisational
Standardised Processes and procedures
The shared training and language regarding patient risk subtheme pertained to training providers in a common language and terminology that helped to create a collective understanding of patient status, resulting in improved communication (I), improved mitigation planning (M) and enhanced and coordinated efforts for carrying out the escalation strategy (E). One frequently mentioned term was ‘watcher’, defined as having a ‘gut feeling’ about a patient that is at risk for deterioration or ‘close to the edge’.13 Additional influences included experienced providers who have better assessment skills, critical thinking and clinical judgement. Also important were these experienced providers’ knowledge of and effective use of available resources and their ability to train others through peer coaching and debriefs (I, M, E).
I think our culture among the residents has really gotten good at teaching us to, from a systems perspective, think about situational awareness and… thorough communication with nurses. (Resident)
In contrast, inexperienced providers (eg, new nurses and residents) who are unfamiliar with standardised processes may have task fixation, as opposed to seeing the whole picture (I). Additionally, new or even seasoned nurses’ reluctance to ask for a second opinion (I) could influence SA negatively, as could providers being asked to care for complex patients with diseases with which they are unfamiliar (M, E). Additional influences included variation in understanding (I) and application (M) of standardised SA terms such as ‘watcher’ and high-risk therapy.
The influences related to the structure to proactively identify and plan for risk subtheme pertained to developing and implementing standardised organisational processes and procedures, including huddles, frequent scheduled assessments and ‘check-ins’ by charge nurses and physicians, MRT calling criteria, planning tools and explicit contingency planning. These practices worked to create a collective understanding of unit and hospital-wide patient status (I), plus expectations, plans and predicted patient care progression (M and E).
I feel like there’s more of an awareness. I’ve been here since 1998 and, at that point, you were scared to speak up. You could speak, but sometimes you didn’t know what words to use. Now, we’re using similar language and it was like the nurses started with getting their physicians on track. (RT)
A limitation to these positive influences included that while it would be ideal to standardise practices and procedures, it is often not done, leading to lack of role clarity, missed communication opportunities and misunderstandings, particularly between the nurses and physicians.
The influences of structure to support handoffs and continuity of care included clear and standardised handoff practices and knowledge of the patient's initial and current status and the patient's family (I, M, E).
….after you’ve had a patient for a little while, you know the history, so you can notice the subtle changes that you might not notice if you hadn’t had the patient before ... having, that good rapport and trust with the families can also help facilitate seeing any subtle changes when a patient is deteriorating. (Charge nurse)
Resident and nurse respondents frequently noted that shift work, more common after the 2011 residency work-hour restrictions, has decreased continuity.
The influences that emerged for a structure that supports adequate workload/staffing included: (1) an improved staff-to-patient ratio to ensure that patient monitoring is appropriate and timely (I), (2) an experienced and diverse team of providers available on all shifts (M, E) and (3) extra resources available if needed (I, M, E). Negative influences on SA were the demands of caring for very sick patients or those with whom providers have less personal and clinical familiarity (ie, disease type) (I, M). Additional negative influences included having fewer resources (specifically on night shifts) and competing demands due to heavy workload.
You get used to covering a certain number of patients on the resident team during the day and then suddenly your volume increases by double when you have sign-outs from other teams. (Resident)
Additional quotes illustrating enablers and barriers for each theme and subtheme are in online supplementary tables S1–S3.
Discussion
Three themes emerged from the focus group data: (1) team-based care, (2) availability of standardised data and (3) standardised processes and procedures. These themes and their related subthemes represent social, technological and organisational inputs that influence a provider's and team's ability to achieve SA and the identification, mitigation and escalation of recognition of patient risk. As opposed to the operating suite and the anaesthesiologist's SA where substantial research and conceptual model building has been completed, 7–9 ,23 ,24 few data were previously available on how SA is improved or threatened on the inpatient wards. We believe our themes and subthemes are related to but may be distinct from those found in anaesthesiology and that these differences reflect differences in the task and cognitive work involved in these distinct clinical environments. Several recent qualitative studies have examined failures to activate MRTs,16 ,17 ,25 ,26 but this study is, to our knowledge, the first to examine the influences on the early identification and treatment of paediatric deterioration, where factors such as vital sign norm changes as children age and preverbal patients may make identification and management more difficult.27 ,28
Our data illustrate the importance of team SA and standardised procedures to support it in the inpatient context (box 1). While we found little data on the cognitive process of individual clinicians, we found substantial data on how teams with different expertise and experience levels can effectively work together to identify, mitigate and escalate the recognition of patient risk. Our subthemes of shared language and training and structure to support handoffs and continuity of care demonstrate the importance of shared SA in the inpatient setting.3 ,11 Shared SA requirements are dependent on the scenario, goals and tasks at hand. We believe that the structures to proactively identify, communicate and plan for risk (such as huddles and multidisciplinary rounds) facilitate shared SA and group decisions and planning.
In healthcare, SA is best studied in anaesthesiology and the operating theatre. The most mature models of SA in this setting come from Gaba and Fioratou.7 ,8 Gaba's cognitive process model illustrates how an individual anaesthesiologist uses data from a sensory/motor level and supervisory and attentional resources to develop abstract meaning and facilitate action planning and action. This model was developed before Endsley and colleague's 3-level SA model, and Gaba has since observed that the observation, problem recognition and allocation and prioritisation of attention in his model resembled that of SA.8 Our model is fundamentally different from Gaba's in that it does not aim to be a cognitive model. We believe, however, that our model shares similarities in that SA is driven by technological processes (data streams in his example) and team processes such as leadership. Fioratou and colleagues recently proposed a model for distributed SA in anaesthesia.7 Distributed SA builds on distributed cognition models and puts focus on physician–environment interactions and not the internal cognitive processes of models of individual SA. While our study was not designed to rigorously evaluate distributed SA in the inpatient setting, we believe our data do speak to the potential importance of the concepts of distributed SA and team SA and a more limited role for the concept of individual SA in healthcare.2–4 Our theme of the availability of standardised data notes the importance of visual displays, while team-based patient care suggests that the unit of analysis for SA in the inpatient setting is better thought of as the team than any individual.
In our examination of SA and identification, mitigation and escalation in the inpatient setting, we found somewhat different themes than described in anaesthesia. While both anaesthesia and inpatient hospital care are high-risk and dynamic environments, the nature of the task work is often quite different. An anaesthesiologist typically cares for one very high-risk patient. This patient is always well monitored but is not interactive. Family is not present to speak for the patient, so not surprisingly empowered patients and families are not described. Vigilance is quite important in this context as is scanning multiple data elements for signal or risk. In the inpatient setting an individual nurse may care for four or five patients, a charge nurse 24 patients and a senior resident 50 or more. In this context, scanning for risk occurred not at the level of monitor readout on an individual patient but at that of the electronic health record where scanning for elevated PEWS was important work. The nature of teamwork may also be somewhat different in the inpatient setting where the make-up of teams changes frequently and where an individual nurse may work with several physician teams and vice versa. As it is difficult, if not impossible, to establish expected team behaviours and dynamics in this setting, our data spoke to more general social inputs such as empowered nurses and a robust safety culture as well as organisational standardisation of important policies and procedures.
The themes discussed did vary somewhat based on focus group participants (table 2). Only three dimensions were discussed in each focus group: shared language around ‘watcher’, the standardised practice of huddles and provider experience. As these were noted across different groups and professions, we believe these dimensions may be important areas for further study and targeted intervention. Charge nurses spoke most commonly about the importance of the ‘gut feeling’. This may be related to the relatively higher level of experience in this group. This experience likely allowed for pattern matching to situations seen earlier, facilitating better comprehension with less cognitive work. Resident physicians spoke commonly about unit culture subthemes, but did not comment specifically on nurse empowerment.
Our study has several limitations. First, retrospective accounts of SA may be inherently biased as respondents only know which data are important once an event has occurred.29 To some extent, we avoided this bias as our respondents ultimately did not provide data on individual SA.3 Instead they spoke to the complex relationships between social, technological and organisational inputs that better fit the model of team SA. While our focus groups generated substantial data on what participants stated influence their SA, we acknowledge there may be differences in how they recounted their actions and what they actually did. Somewhat different influences on SA may be found on direct observation. We chose focus groups as our method of data collection for a variety of reasons. First, they allow ‘like’ participants to reflect on each other's comments and debate or achieve consensus on particular themes. Hearing from others in the group who have similar experiences triggers thoughts and promotes a more engaging discussion than would be possible with a one-on-one interview. There are no validated survey instruments designed to measure the issues of interest in this study. Indeed, our findings will be an ideal basis on which to develop such a survey tool. As noted, direct observation has advantages including being able to capture a wealth of data in real time, but it is limited as validated tools for observation do not exist in the inpatient setting. SA assessment tool such as the Situation Awareness Global Assessment Tool (SAGAT) would require multiple pauses in course of clinical care, which may not be ethical. Additionally, our aim was to learn from high-risk patients who are uncommon and thus it would have been difficult to time any observation assessments.4 Probes directed at SA through a web interface, smartphone or personal digital assistant are an additional promising option to measure SA in clinical care.4 ,30
Additional limitations relate to generalisability. Our centre is a large, academic, tertiary care facility with a decade of experience intervening to improve quality and safety. Thus, some findings may not be generalisable to other institutions. Our total participation rate among nurses was fairly small. However, 80% of all inpatient units were represented and participants included a mix of critical and acute, medical and surgical and subspecialty and general medical care personnel. The nurses who participated were overall very experienced and it is possible that less-experienced providers would identify somewhat different influences on SA.
We believe the findings from this study have several implications and provide some guidance for next steps. Our conceptual model proposes that social, technological and organisational inputs work together to deliver the outputs of improved SA and improved identification, mitigation and escalation of the recognition of patient risk. Interventions targeted at improving safety culture and specific interventions such as structured nurse and family participation in rounds may improve social inputs. Technological inputs may be easier to bring to scale through electronic health records, but research is needed to improve the accuracy of warning scores and develop evidence-based user interfaces. We believe organisational inputs such as training around shared language and huddles to proactively search for risk are particularly important areas for further evaluation and improvement. This qualitative study was only the first aim in this research agenda. Next steps will be to develop and test a quantitative survey instrument to measure SA and influences on each of our themes/subthemes in the inpatient clinical environment. Data gathered from using such an instrument with a much larger group of healthcare providers should provide even greater guidance for identifying areas to target with interventions designed to improve SA and overcome barriers to identifying, mitigating and escalating the recognition of patient risk.
Acknowledgments
We thank Beth Mainwaring, MPH for her assistance with preparing and recruiting for focus groups and Suzanne Campanella, Bennett Farrell, MPH, Eric Kirkendall, MD, MBI, Joshua Schaffzin, MD, PhD, Pamela Schoettker, MS and Kathleen Sutcliffe, PhD, MSN for their thoughtful review of this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors Both authors contributed to the conception and design of the study. LMG led focus groups and the acquisition of focus group data. Both authors analysed and interpreted these data. Both authors drafted the manuscript and critically reviewed each authors’ content. Both reviewed a final version of the manuscript and accept responsibility for its contents.
-
Funding Portions of this project were supported by cooperative agreement number U19HS021114 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
-
Ethics approval Cincinnati Children's Hospital institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The authors have additional quotes from focus group participants (similar to those in supplemental tables) that are available by contacting the first author at patrick.brady@cchmc.org.