Article Text

Abstract
Background Despite ample evidence that hand hygiene (HH) can reduce nosocomial infections, physician compliance remains low. The authors hypothesised that attending physician role modelling and peer pressure among internal medicine teams would impact HH adherence.
Methods Nine teams were covertly observed. Team member entry and exit order, and adherence to HH were recorded secretly. The mean HH percentage across encounters was estimated by compliance of the first person entering and exiting an encounter, and by the attending physician's HH compliance.
Results 718 HH opportunities prior to contact and 744 opportunities after contact were observed. If the first person entering a patient encounter performed HH, the mean compliance of other team members was 64%, but was only 45% if the first person failed to perform HH (p=0.002). When the attending physician performed HH upon entering the patient encounter, the mean HH compliance was 66%, but only 42% if the attending physician did not perform HH (p<0.001). Similar results were seen on exiting the room. The effects of the first person were not driven solely by the attending physician's HH behaviour because the attending physician was first or second to enter 57% of the encounters and exit 44% of the encounters.
Conclusions If the first person entering a patient room performs HH, then others were more likely to perform HH too, implying that peer pressure impacts team member HH compliance. The attending physician's behaviour also influenced team members regardless of whether the attending physician was the first to enter or exit an encounter, implying that role modelling impacts the HH behaviour of learners. These findings should be used when designing HH improvement programmes targeting physicians.
- Medical education
- nosocomial infections
- patient safety
- healthcare quality improvement
- hospital medicine
- adverse events
- epidemiology and detection
Statistics from Altmetric.com
- Medical education
- nosocomial infections
- patient safety
- healthcare quality improvement
- hospital medicine
- adverse events
- epidemiology and detection
Introduction
Hand hygiene (HH) is a cornerstone of infection prevention. Improving HH rates among healthcare workers has been shown to reduce nosocomial infections1 and is promoted by professional societies and government agencies, including the Infectious Disease Society of America, the Centers for Disease Control and Prevention, WHO, and the Joint Commission.2–4 Nevertheless, published adherence rates remain disappointingly low at 56–66%.5–7 Nurses tend to be more compliant with HH than doctors.8
Despite ample education through professional societies, journals and guidelines, changing physician behaviour remains difficult.9 The reasons for poor physician compliance are incompletely understood but appear to be influenced by workload, beliefs, access to HH products and medical specialty.10 The structure of medical training may also play a role. Medical education is complex and involves academic, experiential and social learning, in a structure that uses a combination of apprenticeship and group training. In an educational setting, we hypothesised that HH behaviour would be affected by the peer pressure associated with group rounding, and the role modelling behaviour of the attending physician.
Methods
The study was performed at a large urban academic medical centre with 659 beds and 320 trainees per year. The study protocol was reviewed and approved as ‘exempt’ by the facility's Institutional Review Board. HH locations are plentiful. Alcohol-based hand rub dispensers are located throughout the institution, outside patient doors, and on walls inside patient rooms to the maximum extent allowable by state fire code. Two to four sinks are located near nursing stations on each unit, in each patient bathroom, and in ante-rooms of isolation rooms.
A research assistant who was already embedded into teams by the Department of Internal Medicine to observe the process of bedside rounds and other activities of team building was secretly recruited to observe HH among nine internal medicine teams over a 3-month period in autumn 2010. Each team consisted of one attending physician, one post-graduate year 3 (PGY-3) resident, two PGY-1 residents, one medical student and one pharmacy student. Only the Director of the Institutional Review Board and the authors were aware that a HH observation study was being conducted. The research assistant was trained to perform observations using a published guideline.11 For each team member, she recorded the order of entry and exit from the room, training level and adherence to HH using an encrypted data collection sheet to maintain total secrecy. Individual subjects were identified only by training level, not by name or other identifiers, as a provision of exempt status.
Statistical methods
For each training level, a simple overall percentage of HH was computed as the number of HH occasions divided by the total number of observed opportunities. These percentages were computed separately for entering and exiting the patient encounter. The HH experience of the two PGY-1 residents was aggregated by summing the results for both clinicians. We estimated the mean HH percentage across encounters by compliance of the first person entering and exiting an encounter (yes vs no), and by the attending physician's HH compliance (yes vs no) separately. We examined two behavioural factors that were thought to influence HH: the effect of the compliance behaviour of the first person on the other team members, and the effect of the compliance behaviour of the attending physician on the other team members.
Statistical comparison of the mean percentages was conducted using the Wilcoxon rank-sum test. Analysis of the proportion of HH compliance by order of entering or exiting the patient encounter was conducted using a non-parametric test of trend in proportions.12 All analyses were conducted in Stata V.11.1 (StataCorp).
Results
There were 123 unique patient encounters with 718 observed HH opportunities prior to contact (entering the patient encounter) and 133 patient encounters with 744 observed HH opportunities after contact. (On three occasions the observer did not view the entire team as they entered a patient's room.) The median size of the clinical team was six (IQR 5–7). Overall, HH compliance was 52% prior to contact and 70% after contact. Compliance by training level ranged from 47–67% prior to contact and 64–87% after contact (p<0.001 before vs after) and was highest among medical and pharmacy students (table 1). The order in which team members entered or exited a room did not independently impact the rate of HH. A test of linear trend in the proportion of HH compliance by order was not significant for either entering (p=0.92) or exiting (p=0.98) a room. In other words, simply being the first, second or last person to enter a room did not impact one's likelihood of performing HH.
Overall compliance with hand hygiene by training level
Effect of first-person HH compliance
There were 113 patient encounters for which the first person's HH compliance was observed on entering the room. If the first person entering a patient encounter performed HH, compliance of the other team members was also increased (figure 1). Upon exiting a patient encounter (n=127 patient encounters), the behaviour of the first person leaving the room did not appear to influence the others.

Impact of the first person's compliance upon remaining team members' likelihood of performing hand hygiene.
Effect of attending physician's HH compliance
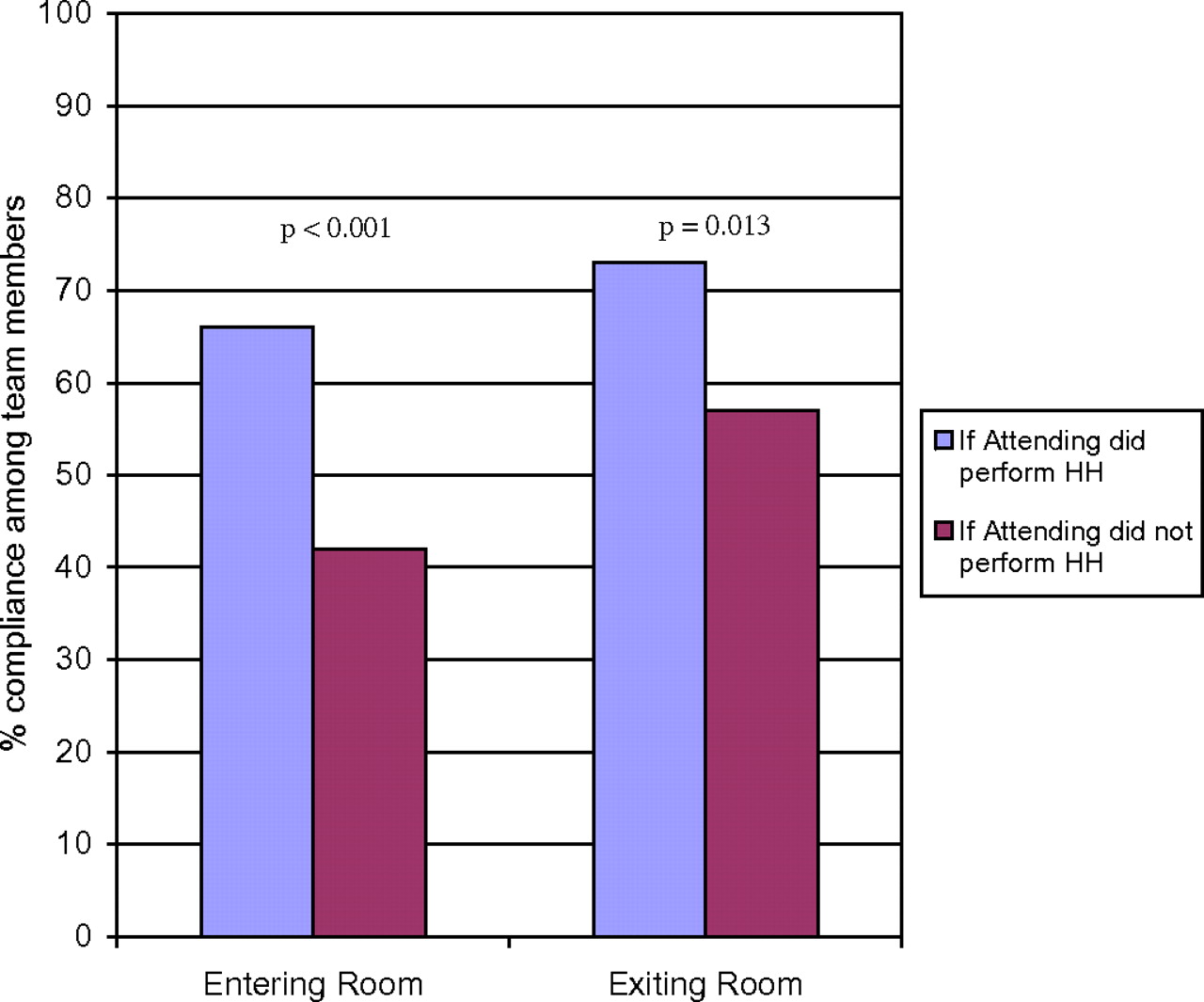
There were 123 patient encounters for which the attending physician's HH compliance was observed on entering the room. Of these, the attending physician entered first on 40 occasions and second on 30 occasions (57% of entries into patient rooms). If the attending physician performed HH upon entering, the overall team member compliance increased (figure 2). Because the attending physician did not always enter an encounter first, we also analysed the behaviour of only those team members who followed the attending physician (n=109 patient encounters). Similar results were found when looking only at these encounters. The mean compliance for only team members who followed the attending physician was 62% if the attending physician performed HH compared with 43% if the attending physician did not perform HH (p=0.006).

{kind=link}
{kind=link}
Impact of the attending physician's compliance on remaining team members' hand hygiene adherence.
The attending physician was observed exiting 127 patient encounters. On 37 occasions, the attending physician exited first and on 19 occasions, the attending physician exited second (44% of all exits). If the attending physician performed HH upon exiting, then overall HH compliance of the team members increased compared with when the attending physician did not perform HH (p=0.013) (figure 2). Similar results were found for the team's HH when we examined only the team members who followed the attending physician (n=95 patient encounters). The mean compliance of the team members following the attending physician was 74% if the attending physician performed HH compared with a mean of 51% if the attending physician did not perform HH (p=0.016). This finding was also supported by qualitative behavioural observations that some initially non-complaint team members who preceded the attending physician doubled back and performed HH when the attending physician was doing so.
Discussion
On the internal medicine teaching service of an academic medical centre, we found a strong follower effect for HH behaviours when entering a patient's room. If the first person entering (regardless of their training level) performs HH, then others are more likely to perform it too. This implies peer pressure may play a role in HH compliance. Additionally, attending physician behaviour exerted an effect on entering and exiting patient encounters, regardless of whether the attending physician went first. This implies that role modelling by attending physicians impacts the behaviour of learners, positively and negatively. In general, HH compliance was greater on exiting patient encounters than on entering them, implying that self-protection may be a stronger driver of behaviour than patient protection.
Our results build on previous findings by Lankford et al showing that HH compliance was more strongly impacted by the HH behaviour of higher ranking staff than by providing more sinks.13 However, no previous studies have quantified the extent to which the social dynamics of medical training can influence HH compliance. The impact of senior physicians on the behaviour of trainees has long been known. However, because role modelling occurs across a wide range of clinical contexts, ensuring that trainees are consistently exposed to good role modelling is difficult. While the effect of role modelling on learning humanistic care and developing a compassionate bedside manner have been described,14 literature is lacking regarding role modelling as a strategy to teach quality and safety at the bedside.
There are several limitations of the study that should be noted. We were unable to examine the independent effects of first-person compliance and attending physician compliance on the team's compliance, adjusting for the effects of other factors, for several reasons. First, there was a substantial correlation between the team's percentage of HH compliance as computed for the first-person effect and the attending physician effect (r=0.89, p<0.001). This may be partly due to the fact that for approximately half of the patient encounters, the attending physician occupied the first or second position. In addition, if the first person and the attending physician performed HH, it is impossible to distinguish the incremental influence of each. Separating these effects would require a controlled behavioural experiment. (Please see online appendix for an expanded discussion of the effects of first-person and attending physician HH compliance.) Second, there are likely to be other factors that we did not measure which may influence HH compliance, such as availability of HH products. Third, some team members did not have contact with the patient or the environment of care during every interaction and thus may have believed they were not required to perform HH. While this fact may have lowered HH rates upon entering a room (because some believed they would not touch anything), we intentionally designed the study to note their compliance because a clinician cannot know whether they will have contact with the patient or the environment before entering the encounter, and thus HH should always be performed beforehand.
There are several implications to be drawn from our study. First, the highest compliance rates were seen with the most junior team members (students), which implies that bad habits are learned from the training environment and pressures of residency. Second, for senior clinicians to make HH an integral part of bedside teaching they need to do little more than perform the task themselves and expect others to follow suit. Third, protecting one's self from harm may be a stronger motivator than protecting others. Finally, healthcare workers at all training levels should be aware that their HH behaviour impacts the behaviour of others, and that good and bad habits can be contagious. These findings should be considered when designing targeted interventions to improve HH compliance among physicians.
Acknowledgments
The authors would like to acknowledge and thank the editor for his thoughtful review and critique of this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by Baystate Medical Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data available on request from the corresponding author.