Article Text

Abstract
Objective: To determine the effect of a shared care programme on the attitudes of newly referred cancer patients towards the healthcare system and their health related quality of life and performance status, and to assess patients’ reports on contacts with their general practitioner (GP).
Setting: Department of Oncology at Aarhus University Hospital and general practices.
Design: Randomised controlled trial in which patients completed questionnaires at three time points. The shared care programme included transfer of knowledge from the oncologist to the GP, improved communication between the parties, and active patient involvement.
Participants: 248 consecutive cancer patients recently referred to the department.
Main outcome measures: Patients’ attitudes towards the healthcare services, their health related quality of life, performance status, and reports on contacts with their GPs.
Results: The shared care programme had a positive effect on patient evaluation of cooperation between the primary and secondary healthcare sectors. The effect was particularly significant in men and in younger patients (18–49 years) who felt they received more care from the GP and were left less in limbo. Young patients in the intervention group rated the GP’s knowledge of disease and treatment significantly higher than young patients in the control group. The number of contacts with the GP was significantly higher in the intervention group. The EORTC quality of life questionnaire and performance status showed no significant differences between the two groups.
Conclusions: An intersectoral shared care programme in which GPs and patients are actively involved has a positive influence on patients’ attitudes towards the healthcare system. Young patients and men particularly benefit from the programme.
- cancer
- shared care
- general practice
- patient-caregiver communication
Statistics from Altmetric.com
Patients with cancer may feel uncertain about what is going to happen when they are referred to hospital and they may experience psychological morbidity and dissatisfaction with the provision of information and care.1 They have stressed the importance of the following aspects in their contact with the healthcare service: doctors’ technical competence, communication skills, continuity of care, family care, and financial circumstances.2 Most patients with cancer are treated as outpatients and may therefore feel left alone at crucial moments. At such times they often consult their general practitioner (GP) for further advice, information, and repetition of information. These contacts place the GP in a key position in which s/he may have problems due to lack of specific knowledge of cancer and lack of collaboration with the oncologists.3–5 This situation occurs frequently and may be remedied by sharing the care between GPs and oncologists.
Shared care has been defined as “care [which] applies when the responsibility for the health care of the patient is shared between individuals or teams who are part of separate organisations, or where substantial organisational boundaries exist”.6 It implies personal communication and organised transfer of knowledge from hospital doctors to GPs and patient involvement. The dialogue between the oncologist and the GP is particularly important.7–9 James et al10 reported that a paediatric oncology information package for GPs helped them to manage their patients’ disease and improved their communication with the oncologists.
This study was undertaken to assess the effect of a shared care programme on the attitudes of newly referred cancer patients towards the healthcare system, their health related quality of life and performance status, and to describe patients’ reports on contacts with their GP. The effect of the shared care programme was measured using questionnaires. Several questionnaires have been developed to assess patient satisfaction with care in either the primary setting or in the hospital. We wanted a questionnaire which could measure the interface between the two settings. The “patient career diary” is a questionnaire which measures patients’ attitude to care across the primary/secondary interface.11 It uses the expression attitude being defined as a psychological tendency that is expressed by evaluating a particular entity with some degree of favour or disfavour.12 A quality of life questionnaire and a performance questionnaire were also used to determine whether the intervention had any influence (negative or positive) on patients’ functioning, symptoms, and overall quality of life.13,14
METHODS
Study population
The study population consisted of cancer patients newly referred to the Department of Oncology at the Aarhus University Hospital, Denmark. The catchment area has a population of 1.3 million, of whom 248 were consecutively included during a 3 month period from August to December 1998. Inclusion and exclusion criteria are shown in box 1.
Box 1 Inclusion and exclusion criteria
Inclusion criteria
-
Informed consent
-
18 years and over
-
Danish citizens, able to understand and speak Danish
-
Mentally able to cooperate
-
Newly referred and diagnosed cancer patients who were scheduled for treatment or attendance for control at the Department of Oncology during a given period
-
Patients with recurrent disease could be included if their last visit took place later than 3 years previously
Exclusion criteria
-
Short palliative radiation therapy without subsequent check up
-
Patients enrolled in a special ambulatory with doctors from other departments (dermatologists and otologists)
-
Patients with a diagnosis of lymphoma (this group was transferred to another hospital during the inclusion period)
-
Patient not listed with a GP, health insurance group II patients (patient co-payment, 2–3% of the Danish population)
Intervention
The intervention was compared with the normal procedure in the department. In the Department of Oncology there were no standard procedures for informing the GPs about newly diagnosed cancer patients. Generally, a discharge summary letter was sent to the GP at the end of the treatment period; some sections in the department would send a short letter at the beginning of the treatment. Sometimes several months could pass before the GP received any information. The discharge summary letters did not follow any guideline.
The shared care programme had three elements (box 2): (1) knowledge transfer; (2) communication channels; and (3) active patient involvement.
Box 2 Shared care programme
Knowledge transfer
-
Discharge summary letters following predefined guidelines
-
Specific information on the disease and its treatment
-
General information about chemotherapy
-
General information about radiotherapy
-
General information about pain treatment
-
Information about treatment of induced nausea and sickness
-
Information about some acute oncological conditions
Communication channels
-
Names and phone numbers of doctors and nurses responsible for the patient were attached to the discharge summary letter to the GPs
Active patient involvement
-
In the intervention group the patients received oral as well as written information about the information package to their GP
-
The patients were encouraged to contact their GP when facing problems they assumed could be solved in this setting
Knowledge transfer
Discharge summary letters were written according to the study guideline and contained details of the investigation, treatment, and information the patient had received. The letters also described in detail which physical, psychological, and social problems the patients had or might expect to get, and contained information about what the oncologists expected the GP to do. In addition, the GP received specific information about the patient’s type of cancer, treatment plans, and prognosis as well as general information about treatment of common side effects and pain.7
Communication channels
Names and telephone numbers of doctors and nurses responsible for the patient were provided.
Active patient involvement
Patients were recommended to contact their GP when facing problems they assumed could be solved in this setting and they were told that the GP would receive an information package.
The shared care programme was launched when the patient left the Department of Oncology or the outpatient department—that is, when the patient left hospital. The information was sent by ordinary mail to the GPs who were receiving patients from the intervention group. The information was expected to arrive the following day.
Outcome measures
The outcome measures focused on the patients’ attitude to the healthcare services, reports on contacts with the GP, and health related quality of life and performance status. Evaluations were performed three times: soon after the introduction of the shared care programme and 3 and 6 months thereafter. The first questionnaire at time 0 was therefore answered after the introduction of the shared care programme. Outcome measures were monitored using three instruments:
(1) The patient’s attitude towards the health care system. Part of an English questionnaire was used together with new questions based on results from interviews with cancer patients and caregivers.7 The new questions were developed on the basis of a template similar to the English questions.11 Two successive pilot tests were performed, each with 10 patients. Firstly, the English questions were translated and tested together with the new questions to reveal linguistic difficulties.15 The second test focused on aspects of content validity.13,16,17 Construct validity was tested on data from the 6 months score, applying principal component analysis, non-parametric correlation Spearman’s rho, and Cronbach’s coefficient α tests.18 The final indexes are shown in the appendix.
(2) The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) (version 3.0). This questionnaire consists of 30 core questions about physical function, global scores, and symptoms. A Danish translation was available and the scoring manual was followed.19 Summarised scales were unweighted in our study.
(3) Eastern Cooperative Oncology Group (ECOG) Scale of Performance Status adopted by the WHO. Questions about performance status were applied to assess the patients’ level of function and capability of self-care.14,20
Sample size
A sample of 194 (2 × 97) randomised patients was theoretically enough to achieve statistically significant differences with a minimal relevant difference of 20%, a 0.050 two sided significance level, and a 10% risk of type II error. Based on an expected withdrawal rate of about 25%, a total of 250 (2 × 125) patients had to be included.
Statistical analysis
Non-parametric analysis was performed as the data did not show a normal distribution. Comparisons between groups were made using the Mann-Whitney U test. Dichotomous data were compared with Fisher’s exact tests. A two sided significance level of 0.05 was chosen.
Results from the questionnaires concerning patients’ attitude towards the healthcare system were dealt with according to the manual.11 The questionnaire scores were linearly transformed to a range of 0–100 where a high score represents a more positive attitude towards the subject. The EORTC-QLQ C-30 questionnaire scores were also linearly transformed to a range of 0–100. A high scale score on a functional scale represents a high healthy level of functioning; a high global health status score represents a high quality of life; but a high score on the symptom scale/item represents a high level of symptoms/problems.19 The results of the questionnaire on performance status were analysed without transformation.
Ethics, randomisation, and masking
The study was approved by the local scientific ethics committee and written informed consent was obtained from the patients.
A project secretary outside the hospital premises kept a list of numbers from 1–250 randomly arranged into two groups. After obtaining written informed consent from the patients, the investigator opened an envelope with a random number of 1–250. This number was communicated to the project secretary who informed the investigator of the group to which this number (patient) belonged. Once a patient was randomised to a particular group, any further patients from the same general practice were automatically assigned to the same group. The study was unblinded. Patients in both groups were informed of the group to which they had been assigned as active involvement of the patients in the intervention group was part of the strategy. The GPs receiving the information packages were asked not to distribute the material among colleagues in order to prevent bias of the control group. The oncologists only had the list to perform discharge summary letters when they had a patient in the intervention group. They were asked not to make any copy of the list to ensure they would not use it in the control group.
RESULTS
Patient characteristics
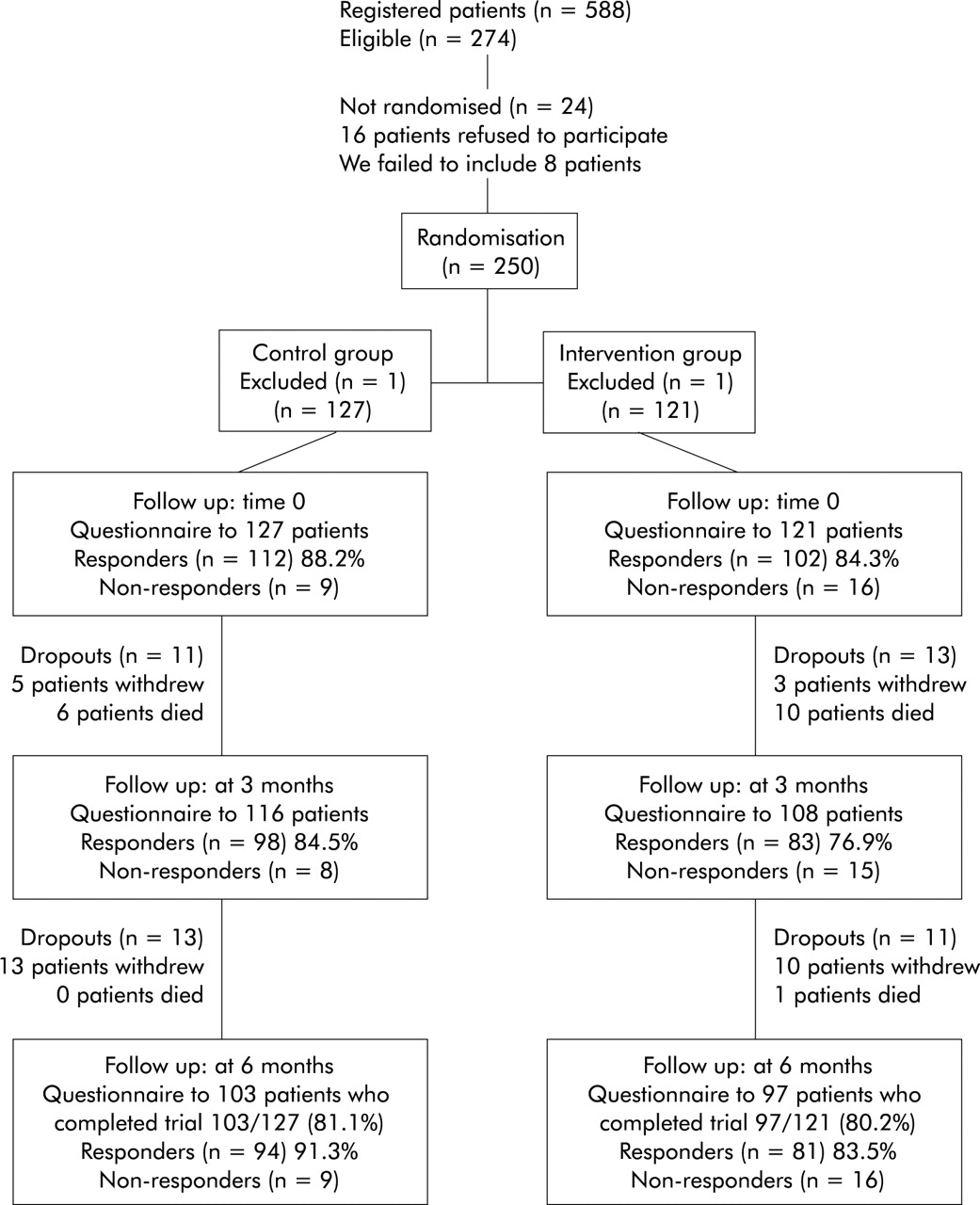
A total of 588 patients were registered between August and December 1998, of whom 274 met the inclusion criteria shown in box 1 and 250 agreed to participate. Sixteen patients refused to participate because they felt they could not manage to fill in the questionnaires and we failed to include eight patients. Two patients were excluded after randomisation because they did not meet the inclusion criteria. The characteristics of the remaining 248 patients are shown in table 1.
Randomisation
Randomisation yielded an almost equal number of patients and an almost equal distribution according to disease and sociodemographic parameters in each group (table 1). However, the randomisation produced an imbalance in age with more young patients (18–49 years) in the intervention group.
Flow of participants and follow up
The progress of the patients through the trial is shown in fig 1. The first questionnaire was given to all 248 patients after introduction of the shared care programme. The response rates and the number of patients who dropped out during the 6 months are shown. A total of 48 patients (24 from each group) dropped out of the study, 17 because they died.
Patients’ attitudes towards cooperation and their feeling of not being left in limbo
The patients’ assessments at 3 and 6 months of four different variables concerning cooperation and their feeling of not being left in limbo are shown in table 2. The questions were not asked at time 0 because the patients had no experience of cooperation between the sectors at this time.
The index and the single item for cooperation showed statistically significant improvements at 3 months (p=0.025 and p=0.004, respectively) but the effect decreased after 6 months. Subgroup analyses on sex and age showed a positive effect for women (p=0.011) and for the younger age group (p=0.001 and p<0.001, respectively) at 3 months.
The index related to patients’ feelings of not being left in limbo indicated a difference at 6 months which was almost statistically significant (p=0.055). At 6 months men in the shared care programme felt less left in limbo (p=0.031), as did the younger age group at both 3 and 6 months (p=0.024 and p=0.031, respectively).
Patients’ attitudes towards their GP
The results for the four variables concerning the GP are shown in table 3. Questions regarding patients’ attitudes towards their GP were asked at time 0 and 3 and 6 months later. At time 0 the intervention group had a more positive assessment of the information they received from their GP than the control group; the difference was almost statistically significant (p=0.051). Men, in particular, assessed the information from the GP more positively at time 0 (p=0.007) and at 6 months (p=0.028). All intervention group patients gave evaluation of care a higher score at time 0 than the controls (p=0.032). In particular, men gave significantly more prominence to this parameter both at time 0 (p=0.003) and at 6 months (p=0.036). The younger age group (18–49 years) also scored higher on care at time 0 (p=0.028). The GP’s knowledge of the disease and treatment was rated more positively by the younger age group at 3 months (p=0.029) than by the controls. The global assessment of the GP was significantly better in the intervention group (p=0.036), particularly for men at time 0 (p=0.010).
Patients’ contacts with their GP during the study
Table 4 shows the patients’ reports on contacts with their GPs. The two groups showed no differences at time 0 when all patients were considered together. However, patients in the intervention group had significantly more contacts with their GPs than the controls, both after 3 months (p=0.049) and 6 months (p=0.046). Analysis by sex showed that men in the control group had the highest number of contacts with their GP at time 0 (p=0.042), but the reverse was the case at 3 and 6 months when men in the intervention group had most contacts with their GPs (p=0.007 and p=0.014, respectively). No differences were seen with regard to the contacts of the female patients. In the older intervention group (50–85 years) the highest contact frequency was seen at 6 months (p=0.050).
Patients’ assessments of their health related quality of life (EORTC QLQ-C30)
The results are presented in table 5 and show no statistically significant differences between the two groups.
Performance status
There was no difference in performance status between the two groups (table 6).
DISCUSSION
The shared care programme used in this study had a significant effect on patients’ evaluations of issues of cooperation, their feeling of not being left in limbo, and their attitudes towards and reported contacts with their GP. Patients in the intervention group overall had significantly more frequent contacts with their GPs than controls. Women in both groups had a positive attitude towards the questions, and Danish women in general contact their GP frequently. Men, on the other hand, are more reticent, but the intervention caused them to contact their GP as often as the women. Studies of sex differences in patterns of confiding among newly diagnosed cancer patients have shown that women turn to several different persons for psychological and social support, whereas men are more likely to have only one confidante, usually their wives.21,22 This study apparently gave men the opportunity of having at least one more confidante—namely, their GP. Young patients in the intervention group ascribed improvements to factors like the GP’s knowledge and care, intersectoral cooperation, and the feeling of not being left in limbo.
There were no differences in EORTC QLQ-C30 scores between the groups and no differences were found in health related quality of life. The intervention did not influence patients’ health related quality of life in either a positive or negative direction, which means that we can tell cancer patients when including them in a shared care programme that it has been shown that it will at least not influence the health related quality of life in a negative direction. The performance status did not differ between the two groups. The shared care programme had no influence on patients’ ability to perform simple physical activities.
The study had the advantage of being prospective and randomised. The participants were included consecutively with a participation rate of 91.2% (248/272), so the study population can be regarded as representative. Randomisation yielded an almost equal number of patients in each group, except that there were more young patients in the intervention group. However, we obtained our goal of equal numbers in each group. Only a few general practices had more than three study patients, which reduced the problem of cluster randomisation as it is known that the design effect is small when the number of patients per general practice is less than 10. Furthermore, assessments were made with validated instruments. Only a few patients were reluctant to participate and high response rates were achieved in both groups, which may indicate that the patients considered the study important. On the other hand, the study may have been too small. The study was designed so that inclusion of 248 patients would be enough to reveal an effect with a minimal relevant difference between the groups of 20%. This may be optimistic, and a type II error may consequently be possible.
We used random allocation without blinding because we wanted to involve the patients by informing them about their possibilities. This implies a risk of information bias by the GP which may have influenced the time 0 scores. Patients in the intervention group may have had more positive expectations of their GP, knowing that they would be better informed about the disease and its treatment, and this may explain why the next two assessments by the GP were relatively less positive. The scores at time 0 should therefore be treated with some caution. However, patients in the control group were also informed about the study and the group to which they belonged, and this information may have caused them to see their GP more than they would otherwise have done. The absence of regular baseline data is a problem as the patients actually received information about the intervention before answering the first questionnaire. They had 14 days to answer the questions at time 0. We had not foreseen this bias due to positive expectations in the intervention group. It would have been a real baseline if the patients had answered the time 0 questionnaires before randomisation, but we had a practical problem with time. The present project took time from the patients’ scheduled time in the hospital. If we had also asked the patients to complete a questionnaire, the logistics in the department would have been disturbed and some patients might have refused to fill in questionnaires in their stressed situation. This might have resulted in only a specific group of patients wanting to participate with the risk of producing a non-representative group of patients. In spite of these problems, we wanted to present the data, knowing that they do not represent a true baseline, so interpretation is not really possible.
Patients’ assessments of the shared care programme were evaluated by questionnaires in which we used part of the “patient career diary” together with new questions. The absence of validation in a large similar study group constitutes a methodological weakness, but the questionnaire was validated with the number of patients we had and we thus obtained a primary validated instrument.11,12
The health related quality of life questionnaire has been validated in Danish cancer patients and we applied the instrument without further validation. The purpose of the EORTC QLQ-C30 questionnaire was to develop an integrated measurement system for evaluating the quality of life of patients participating in international clinical trials to determine whether their quality of life had become better, stayed the same, or become worse while participating in the trial.13,19
The performance status was not validated further in our study as this is a well known and validated instrument. It has also been used to determine whether the use of medication (shared care programme) influences the patient’s ability to carry on his or her normal activities.14,20
Other studies have stressed the importance of providing patients with information as a way of reducing their sense of helplessness.23 Patients with chronic diseases like cancer, who are often treated in different parts of the healthcare system, have a clear opinion about what they demand of the system—namely, access to appropriate care, information about care, knowledge of what is going on, and continuity. Failure in any of these dimensions causes patients to feel left in limbo.24 The present study sought to improve system performance on these dimensions by enhancing patients’ abilities to receive additional information and to have information received in the secondary healthcare sector repeated by their GP. Our results indicate that this approach decreases their feeling of being left in limbo.
Studies on shared care at the primary/secondary care interface show that successful disease management requires communication, role division, and sharing between the healthcare sectors involved.9 Studies on communication across sector boundaries in paediatric oncology have shown that an information package may effectively improve communication between the oncology unit and the GP.10 Our results support these findings. A clinical review of recent advances in oncology emphasises the important role of the GP as cancer treatment is largely an outpatient activity where patients may therefore seek their GP’s advice when presented with treatment options.3 This review stresses the need for GPs to be better educated in cancer care and the importance of communication and discharge summary letters as educational tools for GPs. It also admitted, however, that the best way of achieving good communication between oncologists and GPs has not yet been found.3
The shared care programme used in this study is simple. The oncologists provided the specific information on the different diseases and their treatment. The discharge summary letters were the most difficult part of the programme as they interfered with the daily routine of the doctors. These letters were written according to a predefined guideline and had to be sent on the day the patient left the department or outpatients. However, the department was used to conducting randomised controlled trials so the doctors were willing to follow the guideline for the discharge summary letters. Part of the success was because the department felt an ownership of the project. The head group of consultants accepted the project and told the doctors in the department to follow it. A further reason for its success was that the researcher (JDN) followed the project daily. It is essential to have an innovator when performing shared care programmes across borders in a healthcare system who has connections with both the primary and the secondary sectors. Studies like this could be “rolled out” into routine practice, but not until an innovator for the project is in place. The innovator must be prepared to invest time and energy in getting the project accepted in both settings. In the Danish healthcare system some GPs work a few hours a week in hospital departments as coordinators. These coordinators could be innovators for different shared care programmes.
The challenge to improve interpersonal communication between doctors in different settings remains, however. Further research is required into cultural barriers to communication in the healthcare system because improved communication and patient involvement may give relief to cancer patients and perhaps also improve the overall treatment results and care management. The demand for further research at the interface between the primary and secondary sector is particularly important because the population is growing and its life expectancy increasing, more cancer patients are being diagnosed, and more complex treatment options are being developed. This requires a system in which the organisation of cancer care is well designed, with oncologists sharing their responsibility with GPs.
Key messages
-
Patients with cancer may feel uncertain about what is going to happen when they are referred to hospital and may experience psychological morbidity and dissatisfaction with the provision of information and care.
-
An intersectoral shared care programme had a positive effect on patient evaluation of:
-
attitudes towards the healthcare system;
-
intersectoral cooperation;
-
the feeling of not being left in limbo;
-
contacts with the general practitioner.
-
The effect was particularly significant in men and in younger patients.
Appendix
| Origin | Index/item | Statements |
|---|---|---|
| *Questions developed by Baker et al11 but here mixed with new questions into new indexes. | ||
| †Section 5: Your hospital stay: Your care during the month after you came out of hospital.11 | ||
| ‡Section 2: Other visits to the GP surgery (in connection with your hospital/clinic visits), component 1, information.11 | ||
| New | Intersectoral cooperation | I wished there would be a better cooperation between the hospital doctors and my GP I felt confident about the cooperation between my GP and the hospital doctors I got the impression that the hospital doctors left my GP out The hospital doctors have kept my GP informed of my progress11* |
| New | Global assessment of intersectoral cooperation | Altogether I have been satisfied with the cooperation between my GP and the hospital doctors. |
| Baker et al11 (section 5)† | Feeling of not being left in limbo | After I came out of hospital I sometimes felt as though I had been left “in limbo” After I came out of hospital I knew who to go to for help and advice I wish I had been given a little more help in coping with the medical side of my condition when I came out of hospital I wish I had been given a little more help in coping with my worries when I came out of hospital I would have liked to have been given more information about what to expect when I came out of hospital The hospital staff could have done more to make sure that I would be able to cope when I went home I have had enough information about my progress since I came out of hospital |
| New | Global assessment of not being left in limbo | Altogether I have found things concerning my care that could be improved since I came out of hospital. |
| Baker et al11 (section 2)‡ | Information from the GP | Sometimes I felt that the GP did not see my condition as being very important I came away from the GP visits with some of my questions unanswered I did not get enough advice on my conditions Some of the GP’s advice has been different from the advice that I got from the hospital |
| New | Care from the GP | I felt the GP told me everything that I wanted to know11* My GP has supported me during my illness I felt confident about my GP’s knowledge of my disease My GP is very good at listening to me11* My GP takes the time to listen to me |
| New | GP’s knowledge | My GP has enough knowledge of my disease My GP has enough knowledge of the treatment of my disease My GP has enough knowledge of side effects of my treatment |
| New | Global assessment of the GP | Altogether my GP could have supported me better during my illness |
Characteristics of patients at study entry according to group and sex (n=248)
Patients’ attitudes towards the cooperation between the primary sector and the Department of Oncology and patients’ assessments of their feeling of not being left in limbo
Patients’ attitudes towards their general practitioner (GP)
Patients’ reports on contacts with their general practitioner (GP)
Newly referred cancer patients’ assessments of the EORTC-QLQ-C30 quality of life questionnaire at time 0 and 3 and 6 months after the introduction of the shared care programme
Performance status in control (n=127) and intervention (n=121) groups at time 0 and 3 and 6 months after the introduction of the shared care programme
{kind=link}
Progress of patients through the trial showing number of responders at the three stages of assessment (0, 3 and 6 months). Dropouts between the assessments are shown.
Acknowledgments
The authors thank Morten Frydenberg MSc, PhD, Institute of Biostatistics, University of Aarhus who assisted with the statistical analyses.
REFERENCES
Footnotes
-
This study was funded by the Danish Cancer Society, grant number 9615006.
Linked Articles
- Action points