Article Text

Abstract
Aim To examine the role of workflow redesign to improve medication reconciliation at four Washington State community hospital emergency departments.
Method Lean redesign methodology was used for workflow process mapping and redesign workshops attended by emergency department staff. Observations were made about barriers to successful operation of current medication reconciliation workflows, and ideal future process maps were developed to improve the efficacy of creating a current, complete and accurate medication list for each patient seen in the emergency department.
Conclusion Ideas for an optimal workflow to generate a medication list include involving patients and utilising clerical staff to a greater extent in medication information gathering, identifying and flagging patients with missing medication information, and gathering only the medication information needed to make clinical decisions in the emergency department.
- Medication safety
- emergency department
- process mapping
Statistics from Altmetric.com
Medication reconciliation is a formal process performed by clinical staff to reconcile a patient's medication list with the medications that the organisation is planning to provide.1 Medication lists must be reconciled on admission to a hospital, at the point of transfer between services in the hospital and upon discharge from the hospital. A similar process is used each time a patient is seen in an ambulatory clinic. Medication reconciliation is essential for patient safety because inaccuracies or incompleteness in the current medication list may lead to duplications, drug–drug interactions, omissions and/or dosing errors.2 3 The importance of medication reconciliation for patient safety has been well documented in two Institute of Medicine reports, To Err is Human4 and Crossing the Quality Chasm.5 Supporting research has shown that inadequate medication reconciliation accounts for 46% of all medication errors and up to 20% of adverse drug events resulting from medication errors among hospitalised patients.6 7 Adverse drug events are a leading cause of injury to hospital patients. Approximately two out of every 100 patients admitted to a hospital will experience a preventable adverse drug event during their hospital stay.8–11 Adverse drug events are also among the leading causes of hospitalisation and death in the USA, accounting for about 4.7% of admissions to hospitals.12 13
Most of the literature on medication reconciliation has focused on medication errors and preventable adverse drug events in the inpatient hospital environment. Less is known about medication reconciliation in hospital emergency departments, in which the challenges are fundamentally different than in the inpatient setting. Medication errors in the inpatient setting are due largely to the complexity of in-house medication use and the number of different medications dispensed to patients at various times.8 9 The use of computerised physician order entry and medication dispensing technology, including bar coding, has been effective in significantly reducing inpatient medication error rates.14
The challenge facing emergency department clinicians, on the other hand, is to quickly determine whether any medication a patient is taking may have contributed to the emergency department visit15 16 and whether there is some medication in the patient's system that might limit treatment options.17 With the rapid increase in medication use over the past decade,18 the task of documenting a current, complete and accurate medication list for each patient seen in the emergency department has assumed paramount importance for patient safety. Yet, the task of compiling a comprehensive medication list has become more difficult, especially for those patients taking multiple medications for various conditions. Unlike inpatient staff who often have a hospital information system to assist in creating and cross-checking the medication list for each patient, emergency department staff are more likely to have to rely on patients, family members and other community resources for this essential information, resulting in potentially greater gaps in the medication list or delays in treatment. In an effort to address this burden, the Joint Commission, which is responsible for accrediting hospitals in the USA, including their emergency departments, changed its requirements for medication reconciliation in 2008. Currently, it is adequate to simply include the medication name for patients on entry to the emergency department, dropping the prior full information set, including dose, form, route, frequency and time of last dose.1
Although information technology has the potential to provide specific information to support clinical decision making, it is unlikely that any single technology currently available will automatically generate an accurate medication list on all emergency department patients. This project focused on optimising workflow with the understanding that the information technology tools needed to support an optimal workflow would then become apparent.19 A process improvement strategy based on Lean methodology was used to explore effective ways of redesigning the medication reconciliation workflow.20–22 Lean methodology entails mapping out current workflow processes in detail and then developing an ideal, future-state process map with the goal of reducing wastes and inefficiencies so that a facility can improve its outcomes.
Methodology
The project team organised a 6–8-h workshop at each emergency department site to guide emergency department staff in the workflow assessment and redesign of the medication reconciliation process, and in particular, the creation of the medication list. Each workshop was attended by 8–10 emergency department staff that ‘touch’ the medication reconciliation process. A fundamental concept in Lean methodology is that the people best qualified to analyse and improve a workflow are those actively engaged in the workflow on a daily basis. Thus, the workshop included individuals such as emergency department physicians, triage nurses, pharmacists, health unit clerks, hospitalists and other people with key roles in the emergency department medication reconciliation process. Participants were chosen whom emergency department leadership identified as being opinion leaders and change agents with a whole-systems perspective. This team of individuals created a process map of the current medication workflow. For all emergency department process maps, the starting point was defined as when the patient arrives at the ED and a medication list must be created. The ending point was when the physician enters the room to evaluate the patient, after which clinical decisions are made. This end point was selected (as opposed to when the patient is released from the emergency department) because the medication list is essential in making clinical decisions. The emergency department teams then developed a more efficient and effective future medication reconciliation process based on in-depth discussion and analysis of their current workflow.
Results
Current workflow
All four emergency departments participating in this project independently described current workflows for creating medication lists that were remarkably similar with only minor variations. The main workflow, shown in figure 1, typically consisted of a triage nurse attempting to create a medication list for each patient before the patient was taken back to a treatment room. Medication information brought by patients or supplied by prehospital providers, including emergency responders, assisted living and nursing facilities, was often incomplete. The triage nurse was authorised to access all available information systems and community resources to assemble the medication information; however, competing demands often precluded such efforts. The triage nurse would usually document the medication list completely if the information was known, partially when the information was not readily available or, in some cases, partially with only the medication information that the triage nurse believed would be related to the reason for the emergency department visit. Although the emergency departments all had access to in-house pharmacists, in no case was a pharmacist consistently available in the emergency department to assist in medication reconciliation.

Current workflow for medication reconciliation in the emergency department. ED, emergency department; MD, medical doctor; Pt, patient; RN, registered nurse; Tx Rm, treatment room.
Despite its apparent simplicity, this workflow has several major flaws: (1) it contains a high built-in error rate because patients are often unprepared to help the triage nurse create a reliable medication list; (2) accessing other information sources frequently requires time and effort beyond the capacity of the triage nurse without seriously disrupting patient flow; and (3) there is no consistent mechanism for clinicians downstream to identify which patients have complete or incomplete medication information, often resulting in staff reworking medication lists for patients who have complete information. Emergency department staff members, especially physicians, described how they did not ‘trust’ the patient medication lists that they were given and often felt that they had to restart the process from the beginning. Such miscommunication among staff can be highly disruptive for the emergency department workflow and is responsible for many of the inefficiencies in the medication reconciliation process.
In all four emergency departments, the staff held a set of common beliefs that emerged during the mapping of the current-state workflow. The first of these was an inaccurate assumption that the Joint Commission still requires full medication reconciliation, including dose, time medication was last taken and frequency of use, in addition to medication name upon entry to the emergency department.
Second, there was a cultural phenomenon best described as a resentment of paperwork and regulations among emergency department staff, usually articulated as ‘patient care’ being more important than the ‘administrative’ tasks of compiling a complete medication list. This led to a disconnect between the competing needs of caring for patients with serious trauma (or the emotional needs of their family members) and the essential information gathering tasks required for high-quality clinical decision making and protecting patient safety.
Last, emergency department staff commonly believed that few patients know what medications they are taking. When asked, staff usually stated that about 50% to 60% of patients seen in the emergency department do not know the names of their medications. As part of this project, research assistants documented how many patients truly do not know their medication names. The actual figure averaged 10% (the range was between 2% and 20%). The magnitude of the discrepancy between the perception and the reality illustrates the scale of disruption caused by poor co-ordination of medication information gathering efforts among staff, and the failure to distinguish patients with complete medication lists from those with incomplete lists.
After creating the current state workflow map, emergency department staff turned their efforts to developing an ideal future medication reconciliation workflow. The ideal workflow was created using the staff observations that emerged while mapping the current process, and was based on the principles of waste reduction and single-piece flow integral to the Lean redesign process.
Future workflow
In all four emergency departments, the strategy for the future workflow was to quickly get the percentage of patients who do not know their medications as low as possible and then to standardise the process for gathering any remaining missing information. Emergency department staff in all facilities observed that creation of the patient medication lists would be more productive if patients played a larger role in gathering the information because patients are in the best position to know exactly which medications they are taking. If patients were expected to have their medication lists available when seeking care and were given the tools to track this information, it was felt that the administrative time spent on creating medication lists could be vastly reduced.
The emergency departments began with the premise that efforts to gather medication information upon intake should be limited to the information required for clinical decision making in the emergency department. Additional detail can be gathered later if deemed essential by the emergency department physician or if the patient is admitted to the hospital.
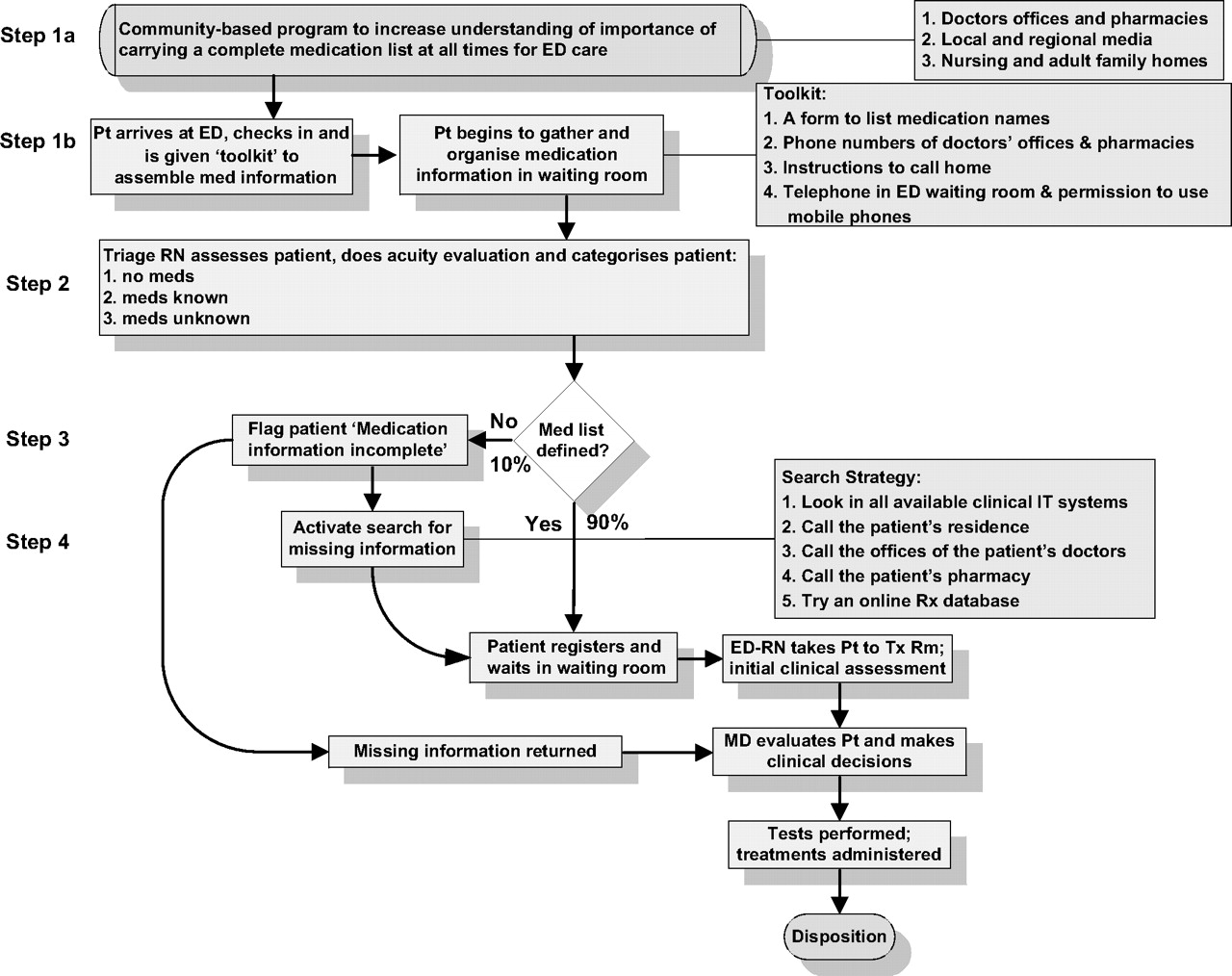
All of the emergency departments developed similar future states workflows with four key steps, as shown in figure 2.

{kind=link}
{kind=link}
Future workflow for medication reconciliation in the emergency department. ED, emergency department; MD, medical doctor; Pt, patient; RN, registered nurse; Tx Rm, treatment room.
Step 1. Involve patients earlier in medication information gathering.
Before patients arrived at the emergency department, they are educated about bringing an updated list of medications with them whenever they visit the emergency department. This education might occur via hospital outreach newsletters, instructions from doctors' offices and pharmacies, and public service messages in local or regional media. Institutions, such as adult and nursing homes, are asked to keep accurate medication lists for their residents and to send that list with the resident in the event of a visit to the emergency department. If they do not come with a complete list, each patient on arrival to the emergency department is given a paper form with instructions to write out a simple list of the names of all his or her medications. The instructions include suggestions to call a family member, a pharmacy or the doctor's office for missing information. Lists of the most commonly used pharmacies and primary care physicians are provided, and telephones are placed in the emergency department waiting room for patients to use for this purpose. This step allows patients to gather as much information as possible before seeing the triage nurse, and it sets expectations for bringing medication organised information on the next visit.
Step 2. Categorise patients by medication knowledge.
The triage nurse reviews the patient's list and categorises the patient into one of three categories.
Category 1: no medications. This group requires no further work other than to document the fact that the patient is not taking medications.
Category 2: medications known. These patients know the names of the medications they take. The triage nurse creates or updates a list of these medications and verifies that the list is complete.
Category 3: medications unknown. This is the small percentage of patients taking medications who do not know the name of at least one of their medications. These patients are the only ones for whom additional information gathering efforts by the emergency department team is necessary.
Step 3. Delegate gathering missing information to clerical staff.
The emergency departments identified a set of standardised tasks, including looking up patient medication information using available information technology tools, such as in-house electronic health records, personal health records and online refill databases, as well as contacting a variety of community resources (see figure 2) that are likely to result in moving the greatest number of patients from ‘medications unknown’ (category 3) to ‘medications known’ (category 2). These tasks can be delegated to medical assistants or even clerical support staff such as unit secretaries, provided they are given adequate tools, clinical support and oversight.
Step 4. Flag patients with missing medication information.
A visual flag is designed to help workers quickly see the status of a process or a product, and is a cornerstone of Lean workflow design. The purpose of flagging patients with incomplete medication lists is to make it obvious to doctors and nurses in the emergency department that a patient has missing medication information. Identifying and flagging patients with missing medication information has the potential to create a larger pool of patients (those with no medications or known medications) for whom the medication list can be trusted, limiting disruptions to the workflow. Finding an ideal visual flag that is acceptable to patients, easily visible to physicians and can be removed as soon as the missing medication information is located poses a challenge. Possible flags include coloured buttons on a hospital gown, a brightly coloured bracelet or a ‘dog-tag’ style necklace. Barriers to implementing such a system include the need to standardise across institutions. Greater reliance on electronic health records may offer opportunities to flag the medication list on the patient's chart rather than the patient.
Discussion
Hospitals throughout the country are grappling with improving their medication reconciliation workflow processes to meet Joint Commission standards for patient safety. Hospital emergency departments have a specific set of barriers independent from the inpatient portion of the hospital in improving their medication reconciliation processes. The medication reconciliation workflow workshops held with four emergency departments in the current project indicate that many emergency department staff are struggling with similar workflow issues and have similar visions for enhancing the process to create a current and complete patient medication list. These enhancement ideas include educating patients about bringing in an updated and complete medication list to each emergency department visit, giving patients additional time and resources to organise their medication information, categorising patients by medication knowledge, identifying and flagging patients who have missing medication information, reorganising staff roles so that the large proportion of clerical duties associated with creating a patient medication list can be performed by lower-level clinical support staff or even clerical staff and assembling only a complete list of medication names for each patient seen at the emergency department, consistent with Joint Commission standards.
Acknowledgments
The authors would like to thank Research Assistants Laurie Rechholtz, Deborah Lee and Michelle Cagat for collecting the data.
References
Footnotes
Funding This project was supported by the Washington State Life Science Discovery Fund to study the interaction between technology and workflow in improving the medication reconciliation process in hospital emergency departments.
Competing interests None.
Ethics approval This study was conducted with the approval of the Washington State Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.