Article Text

Abstract
Objective: To examine the quality of diabetes care and prevention of cardiovascular disease (CVD) in Australian general practice patients with type 2 diabetes and to investigate its relationship with coronary heart disease absolute risk (CHDAR).
Methods: A total of 3286 patient records were extracted from registers of patients with type 2 diabetes held by 16 divisions of general practice (250 practices) across Australia for the year 2002. CHDAR was estimated using the United Kingdom Prospective Diabetes Study algorithm with higher CHDAR set at a 10 year risk of >15%. Multivariate multilevel logistic regression investigated the association between CHDAR and diabetes care.
Results: 47.9% of diabetic patient records had glycosylated haemoglobin (HbA1c) >7%, 87.6% had total cholesterol ⩾4.0 mmol/l, and 73.8% had blood pressure (BP) ⩾130/85 mm Hg. 57.6% of patients were at a higher CHDAR, 76.8% of whom were not on lipid modifying medication and 66.2% were not on antihypertensive medication. After adjusting for clustering at the general practice level and age, lipid modifying medication was negatively related to CHDAR (odds ratio (OR) 0.84) and total cholesterol. Antihypertensive medication was positively related to systolic BP but negatively related to CHDAR (OR 0.88). Referral to ophthalmologists/optometrists and attendance at other health professionals were not related to CHDAR.
Conclusions: At the time of the study the diabetes and CVD preventive care in Australian general practice was suboptimal, even after a number of national initiatives. The Australian Pharmaceutical Benefits Scheme (PBS) guidelines need to be modified to improve CVD preventive care in patients with type 2 diabetes.
- BMI, body mass index
- CHDAR, coronary heart disease absolute risk
- CVD, cardiovascular disease
- DBP, diastolic blood pressure
- HbA1c, glycosylated haemoglobin
- HDL, high density lipoprotein cholesterol
- LDL, low density lipoprotein cholesterol
- SBP, systolic blood pressure
- TC, total cholesterol
- TG, total glycerides
- coronary heart disease
- diabetes
- general practice
- quality of care
- BMI, body mass index
- CHDAR, coronary heart disease absolute risk
- CVD, cardiovascular disease
- DBP, diastolic blood pressure
- HbA1c, glycosylated haemoglobin
- HDL, high density lipoprotein cholesterol
- LDL, low density lipoprotein cholesterol
- SBP, systolic blood pressure
- TC, total cholesterol
- TG, total glycerides
- coronary heart disease
- diabetes
- general practice
- quality of care
Statistics from Altmetric.com
- BMI, body mass index
- CHDAR, coronary heart disease absolute risk
- CVD, cardiovascular disease
- DBP, diastolic blood pressure
- HbA1c, glycosylated haemoglobin
- HDL, high density lipoprotein cholesterol
- LDL, low density lipoprotein cholesterol
- SBP, systolic blood pressure
- TC, total cholesterol
- TG, total glycerides
- coronary heart disease
- diabetes
- general practice
- quality of care
- BMI, body mass index
- CHDAR, coronary heart disease absolute risk
- CVD, cardiovascular disease
- DBP, diastolic blood pressure
- HbA1c, glycosylated haemoglobin
- HDL, high density lipoprotein cholesterol
- LDL, low density lipoprotein cholesterol
- SBP, systolic blood pressure
- TC, total cholesterol
- TG, total glycerides
- coronary heart disease
- diabetes
- general practice
- quality of care
Cardiovascular disease (CVD) is responsible for the deaths of 17 million people worldwide each year (approximately one third of global deaths annually),1,2 and many patients at high cardiovascular risk remain undetected.3 In Australia CVD is a major cause of death.4,5 In 2002 expenditure on cardiovascular drugs totalled $1.2 billion annually, $695 million of this on lipid lowering drugs.6
The AusDiab survey found that type 2 diabetes affects over 7.4% of the total population in Australia aged over 25 years.7 McCarty et al estimated that the direct annual healthcare costs of diabetes in Australia will reach $2.3 billion by 2010.8 Diabetes is a major CVD risk factor.9,10 People with diabetes are 2–4 times more likely to develop CVD,11 with about 65% of those with diabetes dying from it.12
The accurate estimation of CVD risk is critical to determining the benefit of preventive treatment. Coronary heart disease absolute risk (CHDAR) is the probability of developing CHD over a given time period (usually 5 or 10 years). The estimation of CHDAR accounts for multiple factors and has been recommended by many clinical guidelines to guide the management of CHD risk in other countries9,13–15 as well as in Australia.16–18 This is especially important in people with type 2 diabetes.
General practitioners (GPs) play a significant role in primary health care across the continuum of care from prevention of illness to treatment and rehabilitation, and provide consultations to approximately 90% of Australians each year.19 There have been relatively few studies on CHDAR in the Australian general population.20,21
Our aims in this study were to examine the quality of diabetes care and CVD prevention (including medication and referral) in Australian general practice patients with type 2 diabetes, and to investigate the relationship between the treatment and CHDAR. The hypothesis is that patients with a higher CHDAR are more likely to receive therapeutic interventions (pharmacotherapy and referral).
METHODS
Data resource
The Division Diabetes and CVD Quality Improvement Project (DDCQIP)22 is part of the National Divisions Diabetes Programs in Australia. This project collected 3 year data from 2000 to 2002 from CARDIAB, an electronic register system for data collection.23 A formal quality check was used on the register.22 Of 23 divisions using CARDIAB by 2000, 19 agreed to participate. By 2002 there were 16 active divisions (250 practices) participating; the data from three divisions were excluded because the register was not consistently used over the 3 years, having ceased by 2002. GPs using the register were similar to those not using the register with respect to size of practice (32.6% v 38.6% with five or more GPs, p>0.05), accreditation (76.4% v 61.7%, p>0.05), sex (70.7% v 68.9% men, p>0.05), and country of graduation (18.2% v 17.2%, p>0.05). However, they were more likely to be full time than part time (86.0% v 74.3%, p<0.05), and were more frequently aged 45–54 (57.3% v 34.0%, p<0.05) and less frequently aged 35–44 (17.2% v 36.5%, p<0.05).22 Data analysed in this study were extracted from the 2002 register as it had the largest register record and best data quality.
Ethical approval for the study was obtained from the human research ethics committee of the University of New South Wales (UNSW). Participating patients had consented to data being provided by their GPs to the divisions and data were de-identified before extraction.
Statistical methods
A total of 15 294 patients were registered in 2002; 3286 patients were included in the analysis and 12 008 (78.5%) were excluded including 1598 without type 2 diabetes, 1158 due to existing stroke or CVD, 51 due to missing sex, 11 179 due to missing information on smoking status, and 225 who were of indigenous and/or Torres Strait Islander descent and might be unreliably recorded24 and underestimate CHDAR.25 When we compared the contributing factors to CHDAR before and after excluding missing records in smoking, there were no significant differences in age, systolic blood pressure (SBP), glycosylated haemoglobin (HbA1c), but duration was shorter and blood lipids were worse after exclusion. The missing values of independent continuous variables were imputed based on age, sex, and duration using the Expectation Maximisation (EM) method which can produce study variables with a sequence of parameter estimates that, under mild regularity conditions, converge to the maximum likelihood estimator.26 These included SBP (15%), total cholesterol (TC, 36.1%), high density lipoprotein cholesterol (HDL, 50.6%), and HbA1c (35.1%). Ten year CHDAR was calculated for all patients using the United Kingdom Prospective Diabetes Study (UKPDS) risk spreadsheet for populations.27 In accordance with the UK National Institute for Clinical Excellence (NICE) guidelines,28 the CHDAR was divided into lower (⩽15%) and higher (>15%) absolute risk groups. As recommended in the Australian guidelines for diabetes management in general practice,18 the targets for diabetes care were HbA1c ⩽7%, TC <4.0 mmol/l, low density lipoprotein cholesterol (LDL) <2.5 mmol/l, total triglycerides (TG) <2.0 mmol/l, HDL ⩾1.0 mmol/l, and BP <130/85 mm Hg.
Statistical analysis was conducted using SPSS and multilevel logistic regression software (MLwiN).29 Continuous variables were tested for significance by an independent t test, categorical variables by χ2 test.
Patients attending the same practice tended to receive treatment which was more alike than those of another practice.30 Multivariate multilevel logistic regression analysis was therefore conducted with the patient as level 1 and general practice as level 2 using the MLwiN software. To achieve the most parsimonious multivariate model, non-significant factors (p>0.05 or p = 0.05) were gradually excluded from the model with backward elimination. These were sex, current smoking status, HDL, LDL and diastolic blood pressure (DBP).
RESULTS
CHDAR
The characteristics of 3286 patients with type 2 diabetes in different CHDAR groups are shown in table 1. All risk factors were worse in the higher CHDAR group than in the lower CHDAR group (p<0.01) except for body mass index (BMI) and DBP which were worse in the lower CHDAR group.
Characteristics of study subjects by CHDAR cut off (n = 3286)
The mean CHDAR in the 3286 patients (1572 women and 1714 men) was 20.3% (15.0% in women and 25.3% in men); in 1893 patients (57.6%) the CHDAR was higher than the cut off figure of 15% (fig 1). Total CHDAR was significantly higher in men than in women (p<0.01).

Distribution of coronary heart disease absolute risk (CHDAR).
Quality of diabetes care
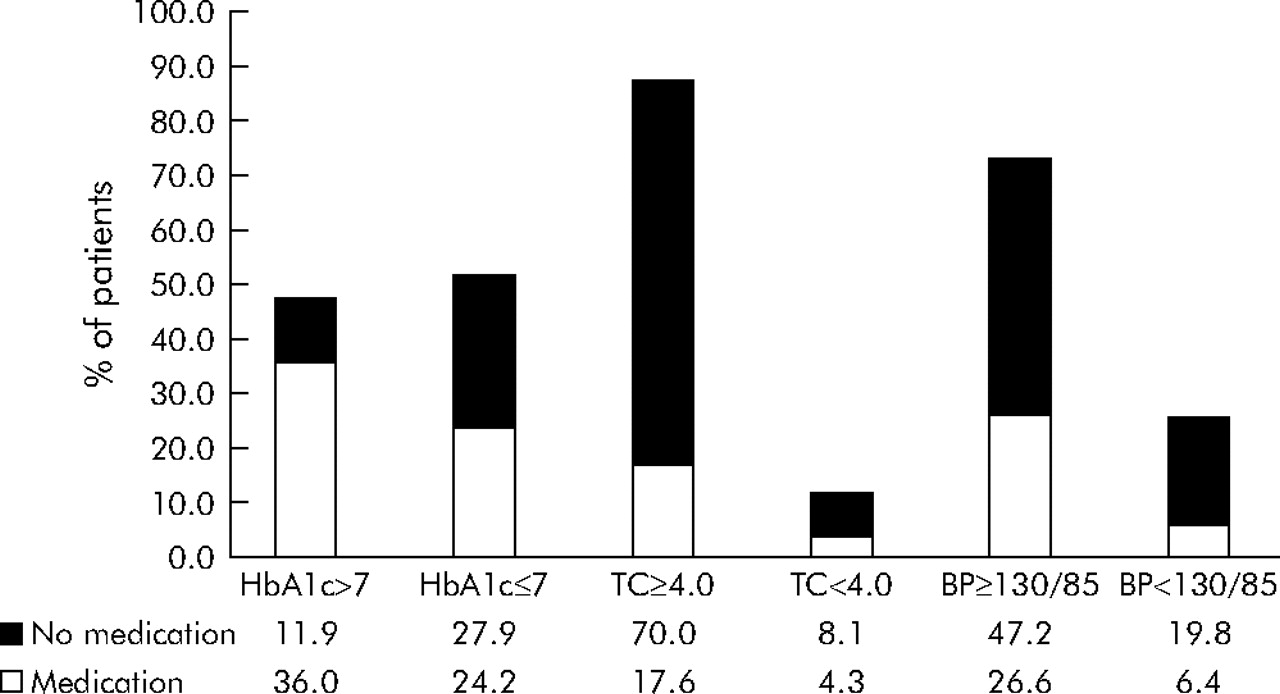
Of 2132 patients for whom HbA1c records were available, 1021 (47.9%) had HbA1c >7%, 768 (75.2%) of whom were on glucose lowering medication; of 2101 patients for whom TC records were available, 1840 (87.6%) had TC ⩾4.0 mmol/l, 369 (20.1%) of whom were on lipid lowering medication; and of 2794 patients with BP records, 2062 (73.8%) had BP ⩾130/85 mm Hg, 744 (36.1%) of whom were on antihypertensive medication (fig 2).

{kind=link}
{kind=link}
Medication use for patients in or out of target (hypoglycaemic, lipid modifying, and antihypertensive medication respectively).
Table 2 shows that 1878 patients (57.2%) were on glucose lowering medication, including 1136 (60.0%) with a higher CHDAR; 727 patients (22.1%) were on lipid modifying medication, including 439 (23.2%) with a higher CHDAR; and 1012 patients (30.8%) were on antihypertensive medication, including 639 (33.8%) with a higher CHDAR. Total cholesterol levels were lower (0.3 mmol/l, p<0.001) in those on lipid medication than in those who were not. Both HbA1c and SBP levels were higher in those on medication (0.9 mmol/l and 4.2 mm Hg respectively, p<0.001). 722 patients (22.0%) were referred to ophthalmologists or optometrists, including 378 (20.0%) of those with a higher CHDAR. Of 295 patients (9.0%) who attended consultations with other professionals (diabetes educators, dieticians or podiatrists), 156 (8.2%) had a higher CHDAR.
Number (%) of patients on treatment by CHDAR cut off
Multilevel analysis
In the final multilevel regression model, after adjusting for clustering effect and age, factors with significant odds ratio (OR) are shown in table 3. Glucose lowering medication was significantly positively related to HbA1c and CHDAR (OR 1.14). Lipid modifying medication was positively related to duration and TG, and significantly negatively related to CHDAR (OR 0.84) and TC. Antihypertensive medication was positively related to duration, SBP and BMI, and significantly negatively related to CHDAR (OR 0.88). Referral to ophthalmologists/optometrists was not significantly related to CHDAR or individual risk factors. Attendance at other professionals was negatively related to age, but not with CHDAR or other individual risk factors. There was a significant clustering effect at practice level (p<0.05). Most of the variance in the medications (glucose lowering medication 65.5%; lipid modifying medication 62.2%; and antihypertensive medication 59.8%) was between patients. However, most of the variance in attendance at other health professionals (80.6%) was between practices.
Odds ratio and variance for relationship between CVD risk factors and treatment in the final multilevel logistic regression
DISCUSSION
Our study found that the mean estimated CHDAR in patients with type 2 diabetes in Australian general practice was above the cut off recommended in the NICE guidelines for medication treatment.28 This supports the proposition that patients with diabetes are at high risk of CVD.11 Men had significantly higher CHDAR than women. This confirms the need for more aggressive management of CHD risk in patients with type 2 diabetes, especially men.
The control of glycemia, blood lipids, and blood pressure improves health outcomes.31–33 However, it is difficult to achieve target treatment goals for patients with type 2 diabetes. A recent study in the United States showed that more than half of the diabetic patients did not attain goals of glycemia control (37.0% with HbA1c <7%), TC control (48.2% with TC <5.18 mmol/l), and BP control (35.8% with BP <130/80 mm Hg).34 Our study found better glycemia control (47.9%) but a higher proportion of patients (73.8%) with BP above 130/85 mm Hg. The proportion of patients in our study with abnormal TC was quite high (87.6%), which might be because our target is more strict (TC <4.0 mmol/l). In Australia there is wide variability in the rates of medication for hypertension (25.6–51.2%) and lipid disorders (8.4–35.7%) between general practice and the hospital setting.35,36 Even allowing for small differences between the guidelines, the rates of prescription of lipid lowering and antihypertensive drug treatment in our study (22.1% and 30.8%, respectively) were low, possibly because GPs were not following the guidelines.
The management of chronic disease (especially CVD and diabetes) is a national priority in Australia. Since 1996 a number of programs such as the National Divisions Diabetes Program37 and the National Integrated Diabetes Program38 have supported improvements in diabetes care in general practice. In the service incentive payment (SIP) general practices received financial incentives if their patients completed an annual cycle of care.39 Despite all these initiatives, this national study of 250 practices found that the quality of diabetes care in Australian general practice was still suboptimal. This implies that there is a gap between the evidence based guidelines (care) for treatments and the accepted standards of quality and the reality of management of CHD risk factors in patients with type 2 diabetes in Australian general practice.
The control of blood glucose, blood lipids, and blood pressure in diabetic patients is very important to prevent CVD complications and decrease mortality.31–33 However, the objective of treatment should be to lower the risk of patients developing CVD complications, not just to lower their blood pressure or lipids. In our study, when lipid medications were prescribed, they were more likely to be associated with lower lipid levels and lower CHDAR. The Australian Pharmaceutical Benefits Scheme (PBS) guidelines,40 which recommend the use of lipid treatment solely on the basis of serum lipid levels, may need to be reconsidered in the light of our findings that over three quarters of diabetic patients with higher CHDAR were not on lipid lowering medication.
Our results also showed that the majority of patients who were in the higher CHDAR group had not been prescribed antihypertensive medication. Those with lower CHDAR were more likely to be on antihypertensive therapy. Again GPs may have been prescribing antihypertensive therapy based on BP level alone, rather than considering CHDAR together with the BP level. Even when antihypertensive medication was prescribed, it was associated with a higher SBP than when medications were not prescribed. This suggests that GPs may need to be more active in controlling BP in their patients with diabetes.
The frequency of attendance with other health professionals such as podiatrists, diabetes educators, or dietitians was low and not significantly related to CHDAR or any of the patient factors other than age. Regular attendance at a diabetes educator, dietitian, or podiatrist might be expected to influence self-management of diet, smoking, physical activity, as well as adherence to treatment. All these may further contribute to both lowering the CVD risk and complications which were more common in patients with a higher CHDAR. Most of the variance in attendance at other health professionals was between practices. This suggests that it was due to the patterns of care of GPs or availability rather than patient selection.
The apparent lack of a relationship between CHDAR and decisions about antihypertensive, lipid, and glucose treatments and referral has important policy implications. The evidence based NICE guidelines28 and other guidelines41,42 have recommended that the management of blood lipids and BP should consider blood lipids and BP along with CHDAR, and that patients with higher CHDAR should be targeted. Our findings highlight the importance of identifying patients with diabetes at higher risk and the need for prescription of medication and referral of patients to be based on combining the assessment of multifactorial CHDAR, together with single CVD risk factors such as lipids or BP. This combined approach needs to be reflected in the Australian PBS guidelines for lipid and BP treatment in patients with diabetes, as well as in education programs for GPs and patients, which will contribute to improving the current suboptimal quality of preventive care in people with type 2 diabetes.
This study has some limitations. It was cross sectional in design and thus unable to draw causal inferences. More research is needed to investigate the impact of quality improvement in clinical indicators especially CHDAR and individual factors over time. There is also a need for improvement in the quality of the data. There were problems in this register with the completeness of some of the information recorded, which reduced the number of useable records. For instance, there is a need to improve the quality of recording of certain items such as smoking status and non-prescribed drugs such as aspirin.
In summary, this is the first national study of CHDAR and diabetes and CVD risk care in patients with type 2 diabetes in Australian general practice. Our study shows that there is a gap between clinical guidelines and accepted care of patients, which suggests that more effort is required to improve the quality of preventive care for CVD in Australian general practice for patients with type 2 diabetes.
Acknowledgments
The authors thank the participating Divisions of General Practice and Mr Gawaine Powell Davies and Ms Sarah Ford from the Centre for Primary Health Care and Equity at UNSW for their assistance with this study.
REFERENCES
Footnotes
-
This study was supported by a grant from the Australian Government Department of Health and Ageing.
-
Competing interests: none.