Article Text

Abstract
Background Nursing workload is increasingly thought to contribute to both nurses' quality of working life and quality/safety of care. Prior studies lack a coherent model for conceptualising and measuring the effects of workload in healthcare. In contrast, we conceptualised a human factors model for workload specifying workload at three distinct levels of analysis and having multiple nurse and patient outcomes.
Methods To test this model, we analysed results from a cross-sectional survey of a volunteer sample of nurses in six units of two academic tertiary care paediatric hospitals.
Results Workload measures were generally correlated with outcomes of interest. A multivariate structural model revealed that: the unit-level measure of staffing adequacy was significantly related to job dissatisfaction (path loading=0.31) and burnout (path loading=0.45); the task-level measure of mental workload related to interruptions, divided attention, and being rushed was associated with burnout (path loading=0.25) and medication error likelihood (path loading=1.04). Job-level workload was not uniquely and significantly associated with any outcomes.
Discussion The human factors engineering model of nursing workload was supported by data from two paediatric hospitals. The findings provided a novel insight into specific ways that different types of workload could affect nurse and patient outcomes. These findings suggest further research and yield a number of human factors design suggestions.
- Workload
- mental workload
- patient safety
- medication error
- quality of working life
- human factors
- nurses
- medication safety
Statistics from Altmetric.com
- Workload
- mental workload
- patient safety
- medication error
- quality of working life
- human factors
- nurses
- medication safety
Introduction
Quality of care and quality of working life in healthcare are oft-cited targets for improvement.1–5 Substantive improvements in both can be achieved by combining a thorough understanding of the healthcare work system with human factors design and redesign.6–13 Excessive nursing workload is among the many work system contributors to quality of care and working life problems that has been internationally recognised as needing further study and remediation.14–21
Aiken's seminal study reported that workload affected patient safety and nurses' well-being,21 findings corroborated by studies in the USA22–29 and abroad,30–37 and supported by anecdotal experiences.38–42 Despite increasing interest in nursing workload, much work remains to be done in the conceptualisation and measurement of nursing workload, its causes and its effects.19 43 44
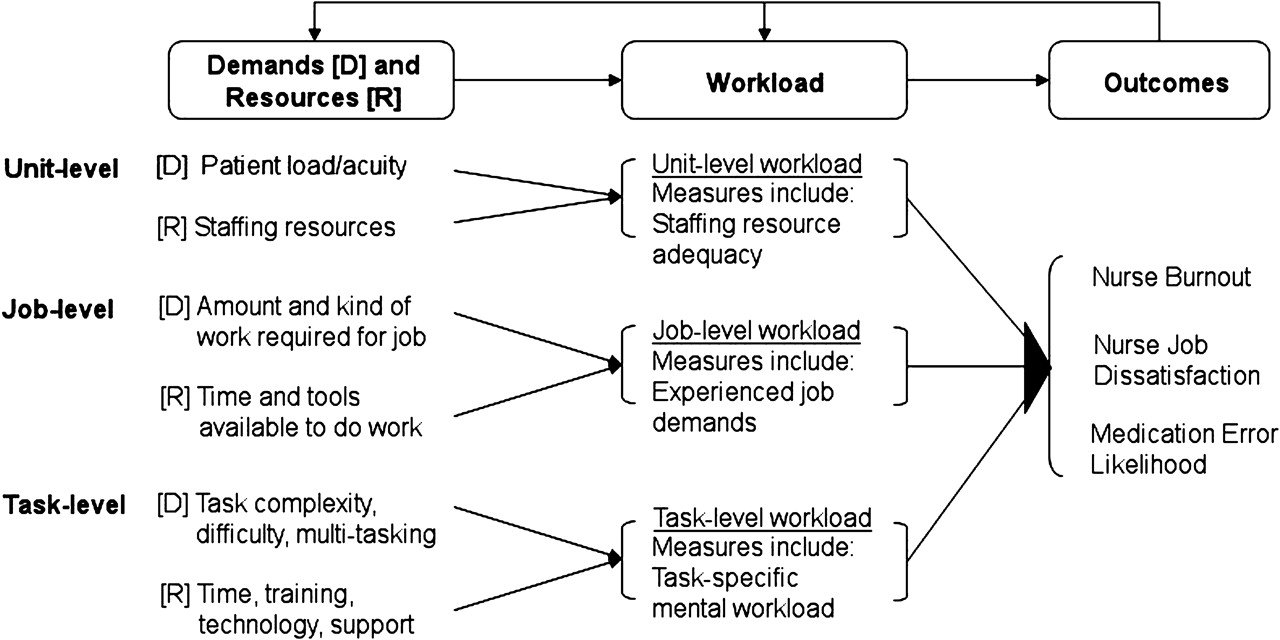
Reviews of nursing workload measurement16 44–47 show that workload is most often defined in terms of staffing ratios. However, staffing ratios are not clearly representative of nurses' actual or perceived workload.47 48 Furthermore, occupational workload research suggests that staffing ratios measure only one type of workload43 49 (figure 1). Generally, workload can be thought of as the ratio of demands (‘task load’) to available resources.50 At one level of analysis, patient-to-nurse ratios might be a good representation of workload. However, there are other levels at which demands and resources interact to produce workload.8 29 43
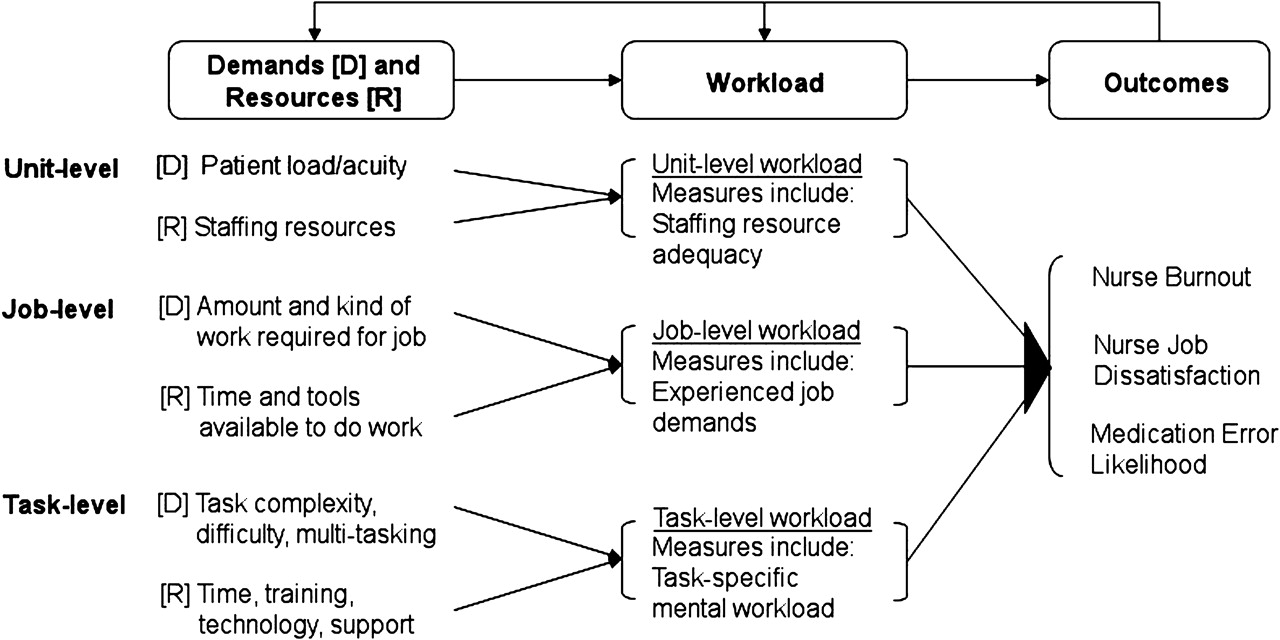
A multi-level human factors framework of nursing workload.
Based on the human factors models of Carayon and Gürses43 and Karsh et al,8 we propose that at least three types of workload exist, resulting from different demands and resources (see figure 1). Unit-level workload refers to the staffing ratios mentioned above. Job-level workload51 52 refers to general and specific demands of the job, including the general amount of work to be done in the day, the difficulty of the work and the amount of concentration or attention required to do it. Resources at this level include time given to complete work, rest breaks and available human (eg, unlicensed assistive personnel) or technological resources. Task-level workload53–55 refers to the demands and resources for a specific nursing task, such as medication administration. Demands might include the need to concentrate or multitask, while resources include training, cognitive capacity, technologies, staff support and more.
Each type of workload is measured in a distinct manner, and each might have a different impact on outcomes such as quality of care, patient safety, nurse behaviour or nurse job dissatisfaction and burnout. Importantly, each type can be addressed through distinct approaches to policy change, training/education and systems design.
The objectives of the current study were (1) to measure each of the three types of workload experienced by nurses at two paediatric hospitals, and (2) to assess whether and which measures of workload were related to three important outcomes: nurses' self-reported job dissatisfaction and burnout, and the perceived likelihood of an error occurring during medication administration. It was expected that some, but not other, types of workload would be associated with each of the outcomes.
Methods
Study design
The study is based on cross-sectional survey data collected from registered nurses at two urban academic tertiary care free-standing paediatric hospitals. The study was approved by both hospitals’ Institutional Review Boards (IRBs).
Sample and setting
Hospital A, in the Midwest, had 222 beds. Hospital B, in the South, had 162 beds. In each hospital, three inpatient units were studied: paediatric intensive care (PICU), haematology–oncology–transplant (HOT), and general medical/surgical. Hospital A, had a 24 bed PICU, 24-bed HOT unit, and 48-bed general medical/surgical unit. In Hospital B, each unit had 24 beds.
Full-time registered nurses (24 h/week or more) in the study units were eligible to participate. Temporary nurses, float nurses or nurses who did not directly provide patient care were not included in the target sample, leaving 203 and 144 eligible nurses from Hospital A and B, respectively.
Measures
All items underwent extensive evaluation procedures56–60 including cognitive interviewing with non-study nurses.61–65 Survey items were measured on 7-point Likert-type scales ranging from 0 to 6, with the category labels ‘not at all,’ ‘a little,’ ‘some,’ ‘a moderate amount,’ ‘pretty much,’ ‘quite a lot’ and ‘a great deal,’ and an option to mark ‘don't know.’ Participants were instructed to think of the past 30 days.
Workload and outcome measures are described in table 1. Both general and specific measures of job-level workload were obtained, the latter focussing on attention demands of the job and comprising two highly intercorrelated subscales that were combined to form a single variable (results were nearly identical using the subscales separately). The two task-level workload scales were developed by the researchers based on the two most valid subjective task workload measures, the NASA-TLX53 and SWAT.54 Using separate internal and external task-level workload scales was a post-hoc decision based on a poor fit between the data and a one-factor confirmatory model; exploratory factor analysis strongly suggested a two-factor solution. The task of interest was medication administration because of the importance of this task to nursing care and patient safety.66 67 Indeed, on a scale of 0 to 6, these same nurses reported that, compared with all nursing interventions, this task had an impact of 5.2 (SD=1.0) on patient outcomes.
Measures used, internal consistency, and examples
Survey administration
Eligible nurses were informed about the study and hand-delivered surveys packets during inservices, staff meetings, or shift-change meetings. Each survey packet was individually labelled with a nurse's name and a unique ID; each contained a personalised cover letter, survey, informational sheet/consent form, stamped reply envelope, and US$5 cash incentive. Nurses were instructed to complete the survey on their own time. Reminder postcards were placed in nurse mailboxes after 1 week, followed by a new survey packet 7–10 days after, and another reminder postcard 7–10 days after that. Data were collected during November–December 2005 and March–May 2006 at Hospitals A and B, respectively.
Analysis plan
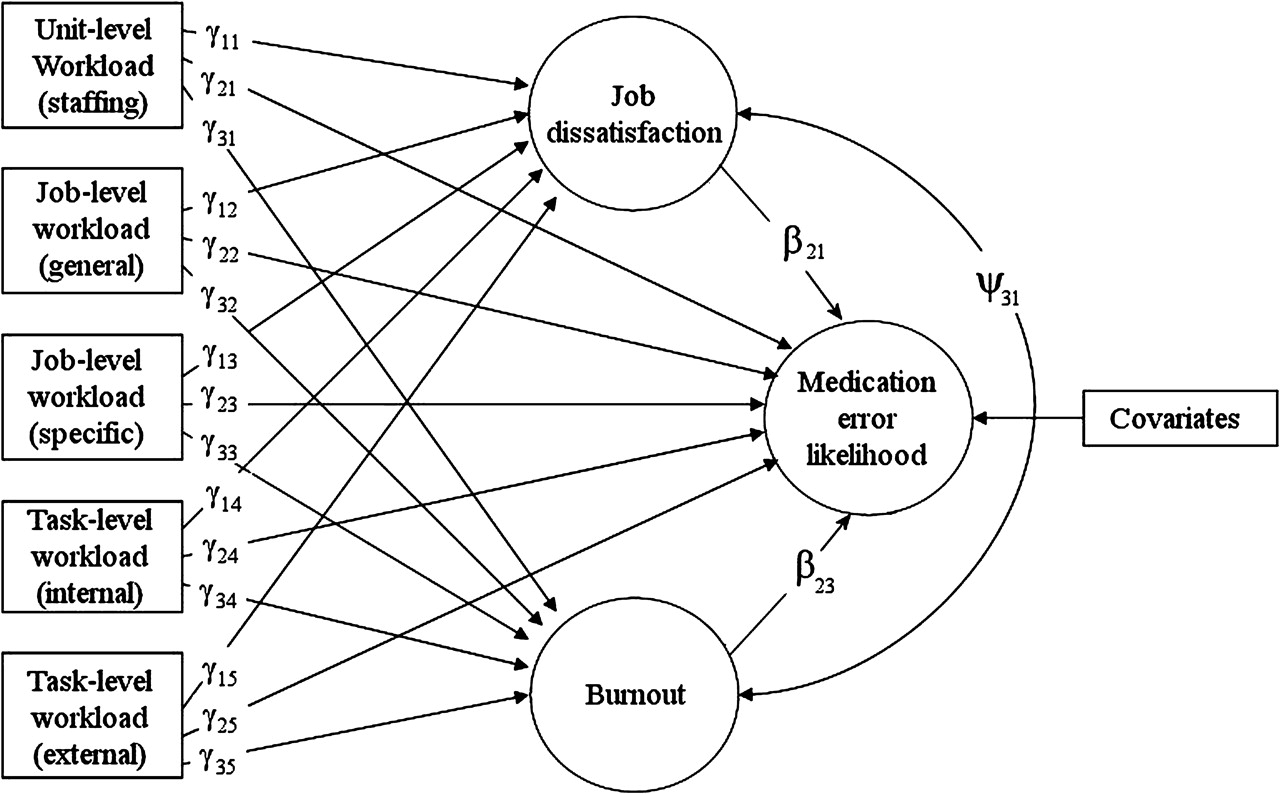
A multilevel logit model68 was constructed, as depicted in figure 2, and path loadings were assessed. Exogenous variables were measures of unit-level, general job-level, specific job-level, task-level internal and task-level external workload. Endogenous variables were job dissatisfaction, burnout and medication error likelihood. The path loading between the three outcome variables were estimated. The model was constructed using the MPlus software (Muthén & Muthén, Los Angeles, California). Parameter estimated standard errors took into account non-independence of observations due to the cluster sampling within units.69 Statistical adjustment was made for hospital, unit, shift, number of hours worked per week, experience (total time with current employer) and age. Due to a lack of variation in gender, ethnicity and education, those variables were not adjusted for. Adding covariates did not change the pattern of results or any outcomes of significance tests. Thus, only statistical values adjusted for covariates are reported. An a priori alpha criterion of 0.05 was used. Where noted, reported correlations were adjusted using the False Discovery Rate approach to counteract the increased chance of Type I error with multiple statistical assessments.70–72

Multilevel logit model. Arrows depict tested path loadings between workload, nurse outcomes, and patient outcomes.
Results
The overall response rate was 57.3%. Table 2 provides sample characteristics. Compared with nurses in the 2004 US National Sample Survey of Registered Nurses (NSSRN),73 nurses in our sample were slightly more likely to be female (NSSRN=93.8% female), more likely to be white (NSSRN=81.2%), more likely to be younger (NSSRN average=45.4 years) and worked fewer hours (NSSRN=43.7). These discrepancies are not unexpected, as in the national sample, 56.2% of nurses worked in hospitals, and only 6.5% worked full-time with paediatric patients, and hospital nurses tended to differ from others.73
Response rates and sample characteristics for both hospitals
For the present analyses, 12 cases were excluded due to missing data on key variables. An additional 11 respondents reported working fewer than 24 h/week and were excluded, although including their data did not change the results of the analyses. The final analysed sample was 176: 99 from Hospital A and 77 from Hospital B.
Table 3 reports descriptive statistics. Self-reported medication error likelihood was assessed with a single item, and the left-skewed (skewness=0.67) distribution of responses on this item suggested dichotomising the variable as follows: responses reporting the likelihood of a medication error to be ‘not at all’ (n=9), ‘a little’ (n=59) or ‘some’ (n=59) were recoded as ‘Low error likelihood;’ responses reporting the likelihood to be ‘a moderate amount’ (n=42), ‘pretty much’ (n=3), ‘quite a lot’ (n=3), or ‘a great deal’ (n=1) were recoded as ‘Moderate error likelihood.’ (Results did not change when medication errors were analysed as a continuous variable).
Descriptive statistics, Pearson correlations and ORs
Table 3 also reports false discovery rate-adjusted Pearson correlations. Workload measures were positively intercorrelated across levels. Job dissatisfaction and burnout were significantly correlated, but neither was significantly associated with the likelihood of medication error. The bivariate correlations between workload and outcome measures demonstrate fairly consistent relationships between the two.
Table 4 summarises results from a test of the statistical model in figure 2. Results show a positive relationship between external mental workload and medication error likelihood (γ25=1.04, 95% CI (0.78 to 1.30)), with a corresponding OR of 2.82 (95% CI (2.17 to 3.67)). There was a significant effect of Hospital on medication error likelihood (OR=0.58; 95% CI (0.37 to 0.93)), such that Hospital B nurses were almost half as likely to report a moderate-or-higher error likelihood, and of unit (OR=1.93; 95% CI (1.04 to 3.58)), such that PICU nurses were nearly twice as likely to report a moderate-or-higher error likelihood, compared with nurses in other units.
Results of model test
Dissatisfaction was positively associated with unit-level workload measure of staffing adequacy (γ11=0.31, 95% CI (0.18 to 0.45)). Burnout was positively associated with both unit-level workload (γ31=0.45, 95% CI (0.24 to 0.66)) and task-level external mental workload (γ35=0.25, 95% CI (0.07 to 0.44)). Dissatisfaction and burnout were also positively associated (Ψ31=0.52, 95% CI (0.42 to 0.63)). All remaining relationships were non-significant. The findings described above were identical to multiple linear and logistic regression equations carried out separately for the three dependent variables (not reported here).
Discussion
This study set out to test the workload–outcome relationships suggested by the multiple-level model in figure 1. The findings provide an understanding of how these relationships may play out: medication errors may be best predicted by task-level workload; dissatisfaction by unit-level workload; and burnout by both unit- and task-level workload.
Representing multiple types of workload jointly as we did here has implications for interpretation and design. Previous studies have demonstrated a relationship between quality/safety outcomes and a single measure of workload such as staffing ratios, as in table 3. A designer might surmise from any significant value from table 3 that a design intervention addressing staffing/resource adequacy, general job demands or task-level (external) workload conditions would improve patient and nurse outcomes. However, the causal inferences and design prospects change when one examines a full model, as in figure 2, where each workload–outcome relationship is adjusted for the effect of the other workload types, and outcomes are free to covary. Following such adjustment, only unit- and task-level (external) workload uniquely relate to the outcomes, and not uniformly so. The multivariate findings suggest to the scientist or designer a deeper understanding of causal mechanisms: for example, the effect of job demands on errors might be mediated by external workload (ie, related to interruptions, divided attention and rushing) during the medication administration task. Thus, a cognitive performance mechanism could be posited to explain medication errors,74 and the designer might realise that for an intervention at the job design level to be successful, it would have to address the task performance factors associated with the medication administration task. This would not be evident from univariate findings.
This is not the first study in which the findings question whether staffing ratios are truly predictive of patient safety,16 31 75 76 raising the possibility that staffing interventions may not be as effective for reducing errors, morbidity or mortality as previously thought, or that only staffing interventions that affect task-level workload will be effective. On the other hand, as expected, workload associated with the medication administration task was related to perceived likelihood of medication error.77–80 Unexpectedly, the task-level workload measure turned out to have two components, an internal one related to mental effort and concentration, and an external one related to exogenous demands of the task. Only the external component was related to patient safety outcomes. This finding requires further analysis and study. One hypothesis might be that mental effort and concentration are beneficial consequences of certain work demands. Perhaps in nursing, some amount of this makes work more satisfying, buffers against burnout and improves patient outcomes through superior performance. Figure 3 shows a comparison of the effect on medication error likelihood of external (upper panel) and internal (lower panel) workload. As suggested here, increases in external workload have deleterious effects on error likelihood, whereas the parabolic error-by-internal workload function is in line with the idea that there are performance benefits to concentration and mental effort at higher magnitudes of these conditions. (This finding is reminiscent of, but not necessarily the same as, the parabolic arousal–performance relationship of the Yerkes–Dodson Law.81) If true, there will be implications for introducing automation and work methods that reduce concentration and effort and make work simpler.82 For example, researchers and organisations studying bar-coded medication administration (BCMA) systems should consider evaluating their impact on clinicians' workload.

{kind=link}
{kind=link}
{kind=link}
Perceived likelihood of medication error as a function of external (upper panel) and internal (lower panel) task-level workload.
Limitations
The use of subjective measures, such as self-reported workload in this study, is the topic of much discussion.83 Because workload is a construct that is internal to a worker,84 85 some argue ‘there is no other way to measure such concepts as workload … directly unless we ask the participant.’86 What is most important in respect to measuring subjective workload is intersubjectivity, or, roughly, the degree to which multiple respondents interpret the questions of the measurement instrument in a similar way.87 The current study took several steps to achieve acceptable intersubjectivity. First, all questions were based on widely used instruments with established validity; second, most constructs were faceted; third, question wording was carefully chosen to reflect commonly understood terminology; fourth, and most importantly, numerous cognitive interviews were conducted in order to evaluate how nurses interpreted survey questions.
A subjective measure of medication error merits careful attention. On the one hand, an internal assessment of error likelihood might have as great an impact as does ‘objective reality.’ Safety-related behaviour such as error reporting, taking risks and taking safety precautions is to a great extent based on risk perception, accurate or not.88–92 On the other hand, patient safety experts are most interested in actual error rates, and subjective assessments of error likelihood are most valuable if they reflect this actuality. Even allowing that nurses' assessments reflect actual error likelihood, the use of subjective error measurement is a limitation of this study. Ongoing analysis of medication error observation at both hospitals will, in the future, provide an objective unit-based error likelihood value that can be used to validate and supplement the self-reported measure.
A further limitation is the inability to assess the direction of causality beyond the theoretical plausibility of the proposed causal model. Another limitation is that workload, a construct purported to exist at multiple levels, was measured by asking individuals. In future studies, this limitation can be addressed through aggregation, consideration of nesting and measurement of workload directly at the level of interest.93 Our specification of task-level workload was limited in that it focused on a single, albeit important, task and that it focused primarily on mental demands of the task. Nevertheless, the findings presented here speak to the importance of medication administration-related (external) mental workload.
Conclusion
In sum, a study carried out at six nursing units at two paediatric hospitals provided interesting possibilities for how different types of workload may relate to common patient and employee problems in paediatric clinical settings. The findings inspire further workload research and a continued multiple-level approach to the study and policy- and design-based resolution of workload in healthcare.
Based on study findings, human factors design solutions include:
Base staffing, assignment and work design decisions on multiple measures of workload, not only on patient census, staffing counts or patient classification systems.
Reduce workload during medication administration by minimising interruptions, concurrent demands and time pressure.29 94
When administration tasks cannot be redesigned, technological interventions such as point-of-care BCMA systems might help detect workload-induced errors before they reach the patient. However, in order to be effective, technologies such as BCMA must be designed and implemented according to good usability and implementation practices.95–99
Do not indiscriminately reduce demands for mental effort and concentration, as these may be beneficial for patient and employee safety. Instead, a task analysis can identify instances in which concentration and effort are important and should be supported, and instances during which they can be alleviated with periods of low mental activity. Related, technological aids or automation may inadvertently reduce the need for concentration or effort, which may not be advisable.
Maintain staffing adequacy. However, if adding staff is not feasible, human factors solutions can be directed at better allocation of work on the unit100 101 or better communication and teamwork.
When redesigning work, changes must be made to the proper level of workload: for example, to reduce errors, general job redesign must include support of medication administration tasks. Care should be taken not to increase one type of workload in an attempt to reduce another.
Finally, further work would benefit from measures of system causes of workload, a broader set of workload measures (eg, capturing physical and emotional demands,49 including physiological indicators of strain102 or focussing on other clinical tasks such as extubation103), and measures of other outcomes of interest, such as safety protocol violations, technology use, perceived quality of care, medication-related injury, turnover and patient satisfaction. Work should continue, especially, in high-risk populations such as paediatrics, critical care and haematology–oncology. Although earlier studies were sufficient to alert us to workload problems, much more remains to be done in the conceptualisation and measure of workload in order to understand the mechanisms at play, a prerequisite for design or engineering interventions to succeed.
Acknowledgments
We thank the study participants and everyone involved in the ‘Bar Coding and Patient and Employee Safety’ study. We also thank the anonymous reviewers, A Alonso and Y Donchin for their helpful feedback. A presentation at the 2007 Human Factors and Ergonomics Society Annual Meeting contained a preliminary presentation of these workload data.
References
Footnotes
Funding This work was supported in part by a grant from the Agency for Healthcare Research and Quality (1 R01 HS013610) to author B-TK. The Agency for Healthcare Research and Quality had no role in the study or publication except for providing funding for the study. Author RJH is supported by a training grant from the US National Institutes of Health (1 TL1 RR025013-01).
Competing interests None.
Ethics approval Ethics approval was provided by the University of Wisconsin IRB, IRBs at each of the two participating hospitals.
Provenance and peer review Not commissioned; externally peer reviewed.