Rates and implications of caesarean sections in Latin America: ecological studyCommentary: all women should have a choiceCommentary: increase in caesarean sections may reflect medical control not women's choiceCommentary: “health has become secondary to a sexually attractive body”
BMJ 1999; 319 doi: https://doi.org/10.1136/bmj.319.7222.1397 (Published 27 November 1999) Cite this as: BMJ 1999;319:1397
Abstract
Objectives: To estimate the incidences of caesarean sections in Latin American countries and correlate these with socioeconomic, demographic, and healthcare variables.
Design: Descriptive and ecological study.
Setting: 19 Latin American countries.
Main outcome measures: National estimates of caesarean section rates in each country.
Results: Seven countries had caesarean section rates below 15%. The remaining 12 countries had rates above 15% (range 16.8% to 40.0%). These 12 countries account for 81% of the deliveries in the region. A positive and significant correlation was observed between the gross national product per capita and rate of caesarean section (rs=0.746), and higher rates were observed in private hospitals than in public ones. Taking 15% as a medically justified accepted rate, over 850 000 unnecessary caesarean sections are performed each year in the region.
Conclusions: The reported figures represent an unnecessary increased risk for young women and their babies. From the economic perspective, this is a burden to health systems that work with limited budgets.
Key messages
12 of the 19 Latin American countries studied had caesarean section rates above 15%, ranging from 16.8% to 40%
These12 countries account for 81% of the deliveries in the region
Better socioeconomic conditions were associated with higher caesarean section rates
Over 850 000 unnecessary caesarean sections are performed each year in Latin America
Reduction of caesarean section rates will need concerted action from public health authorities, medical associations, medical schools, health professionals, the general population, and the media
Rates and implications of caesarean sections in Latin America: ecological study
- José M Belizán, director (belizanj{at}clap.ops-oms.org)a,
- Fernando Althabe, researcher in perinatologya,
- Fernando C Barros, Pan American Health Organisation consultanta,
- Sophie Alexander, lecturerb
- a Latin American Centre for Perinatology, Pan American Health Organisation, World Health Organisation, Hospital de Clínicas s/n, 11000 Montevideo, Uruguay
- b Ecole de Santé Publique, Université Libre de Bruxelles, Campues Erasme CP 595 808, Brussels, Belgium
- Princeton University Department of English, Princeton, NJ, USA
- Center for Population and Development Studies, Harvard School of Public Health, Harvard, USA
- PO Box 569, Blackwood SA 5051, Australia
- Correspondence to: J M Belizán
- Accepted 13 July 1999
Abstract
Objectives: To estimate the incidences of caesarean sections in Latin American countries and correlate these with socioeconomic, demographic, and healthcare variables.
Design: Descriptive and ecological study.
Setting: 19 Latin American countries.
Main outcome measures: National estimates of caesarean section rates in each country.
Results: Seven countries had caesarean section rates below 15%. The remaining 12 countries had rates above 15% (range 16.8% to 40.0%). These 12 countries account for 81% of the deliveries in the region. A positive and significant correlation was observed between the gross national product per capita and rate of caesarean section (rs=0.746), and higher rates were observed in private hospitals than in public ones. Taking 15% as a medically justified accepted rate, over 850 000 unnecessary caesarean sections are performed each year in the region.
Conclusions: The reported figures represent an unnecessary increased risk for young women and their babies. From the economic perspective, this is a burden to health systems that work with limited budgets.
Key messages
12 of the 19 Latin American countries studied had caesarean section rates above 15%, ranging from 16.8% to 40%
These12 countries account for 81% of the deliveries in the region
Better socioeconomic conditions were associated with higher caesarean section rates
Over 850 000 unnecessary caesarean sections are performed each year in Latin America
Reduction of caesarean section rates will need concerted action from public health authorities, medical associations, medical schools, health professionals, the general population, and the media
Introduction
Caesarean sections increase the health risks for mothers and babies as well as the costs of health care compared with normal deliveries. 1–5 Concern has been expressed at the growing rates of caesarean section in some countries of Latin America over the past few years. 6 7 Some developed countries have apparently controlled the increase in caesarean section, although the rates may still be high.8–10 However, in other developed countries, caesarean section rates are still increasing and are a matter of concern. 11 12
Information on rates of caesarean section is not easily obtained for most Latin American countries because of a lack of good national records We estimated the recent incidence of caesarean section in several Latin American countries using different sources of information and correlated these rates with the socioeconomic, demographic, and health variables.
Methods
We studied the Spanish, Portuguese, and French speaking American developing countries. Belize, Surinam, Guyana, and the English and Dutch speaking Caribbean countries were not included. Assistance with deliveries in all Latin American countries is provided by at least two types of hospital: public and private. Public hospitals are free of charge for anyone whereas private hospitals charge patients for their assistance directly or indirectly through private health insurance. Some countries (such as Guatemala, Colombia, and Mexico) also have social security hospitals, which are free of charge but open only to people with jobs affiliated to the social security system and their families.
Sources of data
We contacted various institutions in the countries, such as ministries of health, statistical departments, scientific organisations, social security systems, and hospitals, through representatives of the Pan American Health Organisation. We requested figures for caesarean section at national, regional, or institutional levels. The information obtained came from reports of government health offices derived from routine statistical surveillance or national surveys (Argentina, Bolivia, Brazil, Ecuador, Venezuela, Mexico, Uruguay, Paraguay, El Salvador, Guatemala), the social security system (Costa Rica, Argentina, El Salvador), committees for promotion of maternal health (Mexico), private hospitals (Paraguay), and private health insurance companies (Argentina).
Data from the Demographic and Health Surveys Program were retrieved for surveys made in Latin American countries since 1990.13 The demographic and health surveys collect information on fertility and family planning, maternal and child health, child survival, AIDS and sexually transmitted infections, and other reproductive health topics. Surveys are implemented by institutions in the host country, usually government statistical offices, and 4000 to 8000 women of childbearing age are interviewed in a standard survey. Data from the last surveys made in Bolivia, Colombia, Haiti, Peru, and Dominican Republic were used.
We also used data from the Latin American caesarean section study (Latin American Centre for Perinatology, Université Libre de Bruxelles, European Community). This is an ongoing cluster randomised controlled trial in Argentina, Brazil, Cuba, Colombia, Guatemala, and Mexico testing whether obtaining a second opinion before a caesarean section reduces the rate. To participate in the trial, the hospitals had to provide data on caesarean section rates for 1996 and 1997, and we used data for Colombian and Cuban hospitals Information for Panama's hospitals was provided by a collaborative study of the incidence and causes of caesarean section in hospitals of 18 Latin American countries.14 Finally, we performed a Medline search using the term “cesarean section/statistics and numerical data” or “cesarean section/trends” since 1990. Articles that reported incidence of caesarean section in Latin American countries at national, regional, or institutional level were selected. Reference lists of articles retrieved were also checked.
Population, annual mean number of births, doctors per 10 000 population, urban population, institutional or skilled attendant deliveries, mortality, and caesarean section rates for Latin American countries
Total population and annual mean number of births were extracted from Pan American Health Organisation 1997 data.15 Gross national product per capita, proportion of institutional or skilled attendant deliveries, proportion of urban population, number of doctors per head, and maternal and infant mortality were extracted from 1998 data.16 Data about perinatal mortality were extracted from the Safe Motherhood website.17
Estimates of national caesarean section rates
We estimated the rates of caesarean section for all Latin American countries except Nicaragua, where recent figures were unavailable National figures were obtained by different approaches according to the type and source of the retrieved data. Consequently, we formed three groups of countries: those where national figures were available through periodic surveillance (Chile, Costa Rica, Cuba, Ecuador, Guatemala, Uruguay, and Venezuela); those where national figures were available through special surveys (Bolivia, Colombia, Honduras, Haiti, Dominican Republic, and Peru); and those where national figures were not available and had to be estimated from institutional rates and proportion of institutional deliveries (Argentina, Brazil, El Salvador, Mexico, Panama, and Paraguay)
For Brazil, the total number of caesarean sections performed in one year was available and for Paraguay a probable estimate of the number of caesarean sections in one year. These figures were divided by the annual mean number of births to estimate national caesarean section rates. For Argentina and Mexico, only caesarean section rates for deliveries conducted in public and private sectors and the contributions of these sectors to the total hospital deliveries were available. These data were used to estimate the total number of caesarean sections in one year; the annual mean number of births was divided by this figure to give national caesarean section rates. For El Salvador and Panama, data were available only for public hospitals. National caesarean section rates were therefore estimated from caesarean section rates in public hospitals and the proportion of hospital deliveries. Sources and type of data and ways of estimating the national caesarean section rate (when applicable) for each country are available on the BMJ's website.
Estimates of excess caesarean sections
We adopted 15% as the highest acceptable limit for national caesarean section rates This figure was proposed by the World Health Organisation in 1985 based on the caesarean section rates of some countries with the lowest perinatal mortality in the world.18 In 1991, the figure was adopted as a goal for the year 2000 by the United States Department of Health and Human Services.19 Estimations were made for each country, calculating the hypothetical number of caesarean sections if the rate was 15% and subtracting it from the actual number of caesarean sections.
Analysis of data
We calculated Spearman's rank correlation coefficient to measure the association between the countries' gross national product per capita, the number of doctors per 10 000 population, and the proportion of urban population and caesarean section rates. Since information about gross national product was not available, Cuba was not included in this analysis.
Results
Table 1 gives information about population, annual births, institutional deliveries, urban population, doctors per 10 000 population, mortality, and caesarean section rates of the countries. Seven countries had caesarean section rates below 15%. The range for the remaining 12 countries was 16.8% to 40.0%. These 12 countries represent 81% of the deliveries in the region. Information about rates of caesarean section in different types of hospitals were available for Argentina, Brazil, Chile, Colombia, Mexico, and Paraguay. In all of them, the proportion of caesarean section in women in private hospitals was much higher than that of women in public hospitals. Three countries had caesarean section rates over 50% in private hospitals (table 1). Countries with caesarean section rates below 15% also showed lower proportions of hospital deliveries or births assisted by skilled attendants (28% to 67%) than countries with caesarean section rates above 15% (59% to 100%)
Estimated annual number of caesarean sections and annual number of caesarean sections above 15% upper limit suggested by WHO for Latin American countries
A positive and significant correlation was observed between rates of caesarean section and the gross national product per capita (rs=0.746, n=18, P<0.0001; figure), the proportion of urban population (rs=0.730, n=19, P<0.0001), and the number of doctors per 10 000 population (rs=0.690, n=19, P=0.001). All but one of the countries with gross national product per capita below £2800 showed caesarean section rates below 15%, while all but one of the countries with gross national product per capita above £2800 had caesarean section rates above 15%. The exception is Dominican Republic, with a gross national product per capita of £2740 and a caesarean section rate of 25.9%.
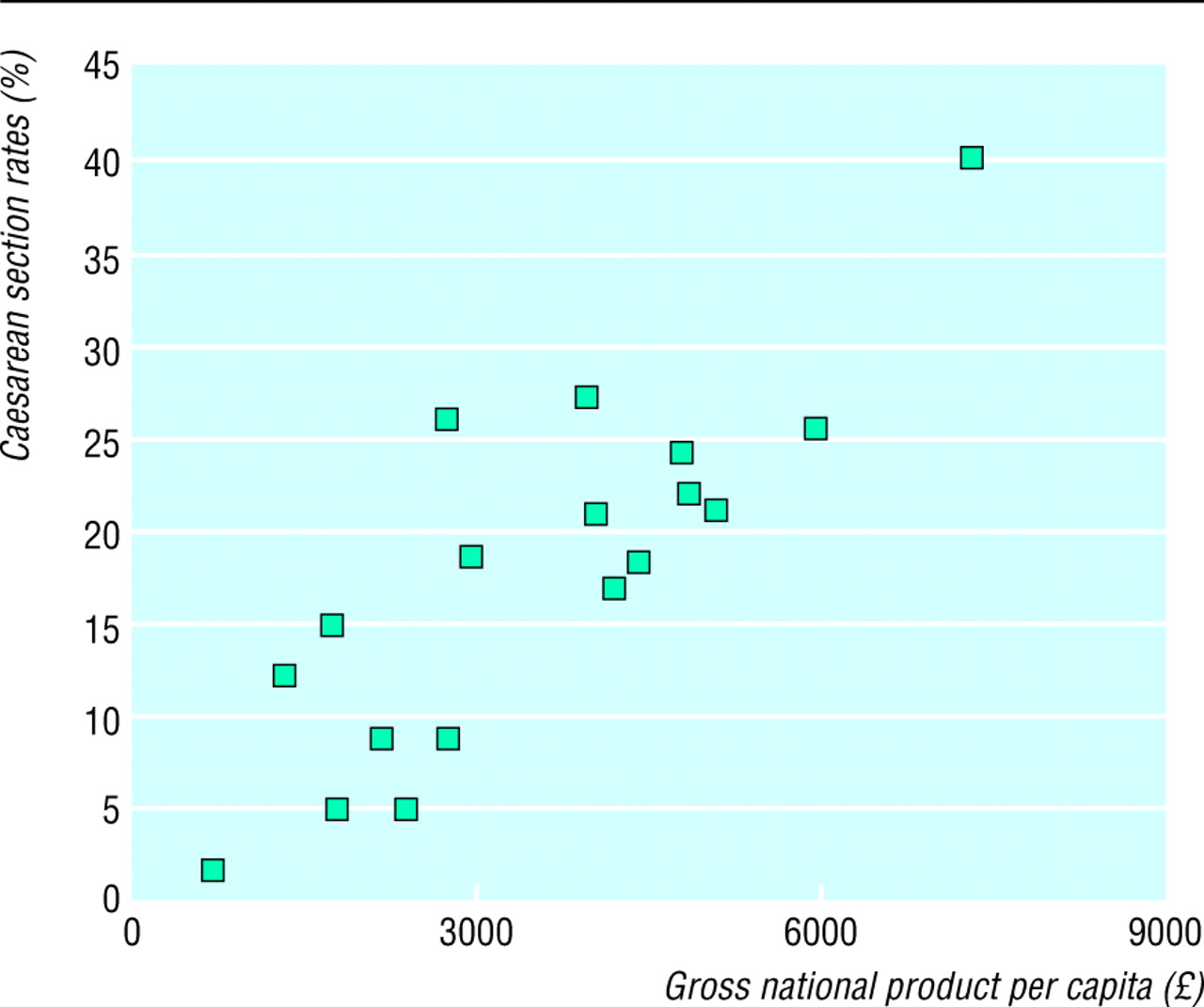
Correlation between the gross national product per capita (£) and caesarean section rates in 18 Latin American countries (rs=0.746)
{kind=link}
In the 12 countries with caesarean section figures above 15%, around 2.2 million caesarean sections were performed each year. Taking 15% as the medically justified rate, we calculate that around 850 000 unnecessary caesarean sections were performed each year in the region (table 2).
Discussion
We had difficulty estimating national rates of caesarean section as national figures were often not available and had to be calculated from different sources of data. Therefore, figures for some of the most populated Latin American countries (such as Brazil, Mexico, and Argentina) cannot be regarded as totally accurate but are the best possible estimates.
For these estimations, we adopted the most conservative approach. We assumed that all non-hospital deliveries were vaginal deliveries and included them in the denominator. When data from the private sector were missing, the national caesarean section rates were based on public hospitals rates, which are generally lower than rates in private hospitals. When multiple sources of caesarean section figures were available for one country (as in Argentina), the lowest figures were used to estimate the national rate.
In the countries where the national caesarean section rates had to be estimated from data from different institutions, estimates are inevitably inaccurate and subject to wide variability. The variability of the estimates calculated from multiple sources (Argentina) or sources with wide coverage (Brazil) was probably smaller than the variability of estimates calculated from only one source (Paraguay) or sources with less coverage.
Relation with socioeconomic indicators
We found a clear positive association between socioeconomic indicators and the proportion of caesarean sections, a finding that has been described in previously. 1 6 20 Strong associations were found between the proportion of caesarean sections and the gross national product per capita, the number of doctors per 10 000 population, the proportion of urban population, and the proportion of institutional deliveries. Moreover, in all countries for which the information was available, the proportion of caesarean sections in private hospitals was higher than that in public or social security hospitals. Although higher caesarean section rates are positively related to higher income and social class, women with low income are at high obstetric risk. Women assisted in public hospitals are more likely to be single, less educated, adolescent, and to have a poorer history than women attending private hospitals.21 No medical justification exists for the finding that women with low obstetric risk, and presumably least likely to benefit from a caesarean section, had higher caesarean section rates.
When considering the implications of our findings the limitations of the ecological design must be remembered. In this type of study, the validity of the inferences depends on the ability to control for differences among countries in the joint distribution of confounders, including individual level variables.22 These data were not available for most countries. Despite the possible confounding effect of factors that were not controlled for, the associations we found suggest the need for further investigation into which factors related to the doctors' and women's decision making processes influence caesarean section rates.
Limiting caesarean sections
Using the limit of 15% set arbitrarily by the WHO in 1985 but still accepted by the scientific community, 19 we calculated an excess of over 850 000 caesarean sections a year for Latin America. This figure represents an unnecessary increased risk for women and their babies. From the economic perspective, it is a burden to health systems that work with limited budgets. On the other hand, the low proportions of caesarean section observed in countries like Haiti, Guatemala, and Bolivia probably represent lack of appropriate medical care rather than ideal health care.
Although the epidemic of caesarean section in Latin America is not new, 6 little action is taking place to reduce its use. This is partly because caesarean section is now culturally accepted as a normal way of giving birth.23 To be effective, actions to reduce caesarean section would need to involve public health authorities, medical associations, medical schools, doctors, midwives, nurses, the media, and the general population. Scientifically tested medical approaches to decrease caesarean section rates at hospital level are also much needed. A multicentre intervention study investigating the effect of obtaining a second medical opinion whenever a caesarean section is indicated is under way in six countries in the region and may indicate new ways to prevent the overuse of this potentially dangerous surgical procedure.
Acknowledgments
We thank all focal points of the health promotion and protection division and all country representatives of the Pan American Health Organisation for sending information about caesarean section rates. We also thank Arachu Castro for providing useful information.
Contributors: JMB had the original idea; participated in the design, execution, analysis, and writing of the paper; and is the study guarantor. FA participated in the design of the study; collected, organised, and analysed the data; and participated in writing the paper. FCB participated in the analysis and writing of the paper. SA participated in writing the paper.
Footnotes
Funding Latin American Centre for Perinatology, Pan American Health Organisation, World Health Organisation.
Competing interests None declared.
References
Commentary: all women should have a choice
- Elaine Showalter, professor of English (112075.445{at}compuserve.com),
- Anne Griffin, research assistant
- a Latin American Centre for Perinatology, Pan American Health Organisation, World Health Organisation, Hospital de Clínicas s/n, 11000 Montevideo, Uruguay
- b Ecole de Santé Publique, Université Libre de Bruxelles, Campues Erasme CP 595 808, Brussels, Belgium
- Princeton University Department of English, Princeton, NJ, USA
- Center for Population and Development Studies, Harvard School of Public Health, Harvard, USA
- PO Box 569, Blackwood SA 5051, Australia
- Correspondence to: E Showalter
The first woman in England powerful enough to demand chloroform in childbirth was Queen Victoria. At the end of the 20th century, medical and social prejudices against women sidestepping their biblical sentence to painful childbirth are still with us. The study on caesarean section in Latin America establishes that the rate of caesarean is higher in private hospitals and among a more prosperous sector of the population. But its conclusions that this rise represents an “epidemic of caesarean section” that has “no medical justification” are based on arbitrary guidelines, insufficient data, and outmoded thinking about women's reproductive needs.
The implication is that wealthy women are wasting the time and money of healthcare providers because they are evading natural childbirth for the selfish convenience of a caesarean section. Because higher caesarean rates are related to higher income and social class does not prove that they are a luxury like plastic surgery. Indeed, the reasons for the increased rates of caesarean section in western societies are both medically and socially complex. According to the 1999 Confidential Enquiry into Stillbirths and Deaths in Infancy, more and more large babies are being born in Britain because of the better nutrition and health of modern mothers. 1 Caesarean section is safer than ever before. The really serious issues around caesarean sections can be seen in underdeveloped countries where they are denied or unavailable to most women, rather than in those western societies where their rates have increased.
A rigorous assessment would investigate the average weight of babies, proportional maternal weight gain, the rates of surgical complications and fetal and maternal death, and the contexts of the medical decision before sounding the alarm. Possibly the increase in rates in Latin American countries reflects an improvement in medical services and education. Possibly it reflects better monitoring for detecting fetal distress.
In a recent article Caroline da Costa noted that “the high rate of caesarean sections in most western countries is now regarded as a major public health problem and has spawned much discussion, numerous publications and meetings, varied recommendations, and some success in reducing the rate in certain hospitals, although without any agreement as to what the optimum rate should be, and with some indications—uterine dystocia and fetal distress—not well defined.” 2 But, she pointed out, the real issue is the discrepancy in maternal health care for women because of economic, political, or religious factors. The World Health Organisation guidelines of 15% for national caesarean section rates are arbitrarily chosen and need to be reviewed. Women's equal access to quality medical services, rather than assumptions about the proper form of labour and delivery, should be our central concern.
Footnotes
Competing interests None declared.
Commentary: increase in caesarean sections may reflect medical control not women's choice
- Arachu Castro, David E Bell research fellow (acastro{at}hsph.harvard.edu)
- a Latin American Centre for Perinatology, Pan American Health Organisation, World Health Organisation, Hospital de Clínicas s/n, 11000 Montevideo, Uruguay
- b Ecole de Santé Publique, Université Libre de Bruxelles, Campues Erasme CP 595 808, Brussels, Belgium
- Princeton University Department of English, Princeton, NJ, USA
- Center for Population and Development Studies, Harvard School of Public Health, Harvard, USA
- PO Box 569, Blackwood SA 5051, Australia
Although safer caesarean sections help reduce maternal and infant morbidity and mortality, they remain a major surgical procedure that carries risk, particularly respiratory complications and neurological impairment for the newborn.1 When not medically indicated, therefore, a caesarean section is less safe than a vaginal birth. It also increases the use of medical and healthcare resources. In addition to these public health arguments, women's voices need to be included in the strategies designed to decrease the incidence of caesarean sections.
Belizán et al present a snapshot showing the high proportion of caesarean sections in Latin America and its association with improved socioeconomic conditions. This association is linked to women's increased access to health services and to the increased availability and use of technical procedures for birth. However, the fact that the proportion of caesarean sections rises as socioeconomic conditions improve does not necessarily mean that the quality of care in the management of labour improves. Actually, it might be otherwise.
Firstly, the systematic use of medical technology, justified by the underlying idea that a woman's body is not capable of giving birth without medical intervention, seems to be more directed towards the convenience of healthcare professionals than the benefit of women in labour. For healthcare professionals, having the woman under control in a horizontal position and stuck to the oxytocin perfusion, the epidural anaesthesia and, although less common in public hospitals in Latin America, the electronic fetal monitor, creates the impression that she is being taken care of. But women tend to perceive such an experience as painful, frightening, and confusing, especially in the many hospitals where they cannot be accompanied by the person they choose.2 The medicalisation of birth seems to preclude the use of less technical, less expensive, and more women centred approaches to birth such as the provision of psychosocial support during labour.
Secondly, the increase of caesarean sections does not necessarily mean that women prefer or request them. 2 3 Our experience in Mexico is that obstetricians, partly because of personal financial benefits, create the high demand for caesarean sections by offering them to the higher socioeconomic groups as a distinctive way of giving birth or by presenting them as a frequent outcome in cases of relative indications for a caesarean section With time, people from other social groups start to imitate this trend, assuming that if the more privileged prefer it, it must be better, and thus it becomes the standard. As a result, many obstetricians end up being better trained to perform a caesarean section than to attend births that could have been safely delivered vaginally. The increase of caesarean sections can thus be regarded as a process in which women are finally given less information and less choice and in which obstetricians appropriate the central role of childbirth at the expense of women.
Finally, “violence” is a strong word, and labelling unnecessary caesarean sections as form of violence against women could be disturbing. But for many women, a caesarean section that could have been avoided is a violation of their bodily integrity, just like having routine episiotomy (or perineal cutting), epidural anesthesia without consent, non-indicated oxytocin induction or augmentation, multiple and painful vaginal examination, non-indicated amniotomy, or pubic shaving, needless exposure of sexual parts in common labour rooms, or even transcaesarean tubal ligations when women do not understand the permanent nature of the procedure. In order to give back to women the central role in childbirth, new guidelines aimed at restricting the use of caesarean sections and other birth technologies by improving the quality of care should be welcomed.
Footnotes
Competing interests None declared.
Commentary: “health has become secondary to a sexually attractive body”
- Hilda Bastian, consumer health advocate (hilda.bastian{at}flinders.edu.au)
- a Latin American Centre for Perinatology, Pan American Health Organisation, World Health Organisation, Hospital de Clínicas s/n, 11000 Montevideo, Uruguay
- b Ecole de Santé Publique, Université Libre de Bruxelles, Campues Erasme CP 595 808, Brussels, Belgium
- Princeton University Department of English, Princeton, NJ, USA
- Center for Population and Development Studies, Harvard School of Public Health, Harvard, USA
- PO Box 569, Blackwood SA 5051, Australia
I am one of those women who see the experience of birth as a profoundly important life event. I gave birth to both my children at home. Some women (including many of the medically trained 1) may think I mortgaged my sexual future and my continence for something trivial, but I would not agree.
I am also a consumer advocate, with a strong commitment to individual rights My personal birth choice was a minority one in my community, of which many disapprove—some would even like to outlaw it. From that position, my commitment lies automatically with women's individual choices. I do not believe that anyone has the right to demand women give birth vaginally—just as no one should force me to have a caesarean.
But national caesarean section rates of up to 40%? In countries where many women in poor health are receiving little health care? Back in the early 1980s, caesarean rates of 75% were already being reported in some urban Brazilian clinics.2 Since then, the national rate has soared but not women's socioeconomic or sociopolitical status. That raises two critical questions: is caesarean section for some Latin American women becoming almost universal? If so, what will that mean for all women in those societies?
At one level, the trend is not so different from that among at least some well off women everywhere. Even in the United Kingdom, where the caesarean section rate is low, a survey of women obstetricians found that 31% of them would choose a caesarean without any medical indication.1 They would do this for much the same reasons as Latin American women do3: mostly to avoid genital damage.
Belizán et al have highlighted an international phenomenon. It is just perhaps more dramatic in countries with “a popular obsession with maintaining a sexually appealing body.”3 Large numbers of women in many wealthy societies starve themselves and take up smoking to achieve a desired body image. That they would choose major surgery for similar reasons is no surprise What, however, is the role of the medical profession in this phenomenon?
High caesarean section rates are partly a consequence of having a surgical specialty responsible for care around birth and as yet poorly understood features of the relationship between private specialists and pregnant women. Brazilian anthropologist Cecilia de Mello E Souza has shown how obstetricians appropriated women's fear of labour pain, body disfigurement, and concern for sexual performance to justify the profession's own preference for surgical birth.3 She believes that as a result “health has become secondary to the production of a sexually attractive body.”3
The medical profession has other overall responsibilities here. Definitive evidence about issues of concern to women (such as pain before and after birth, postpartum depression, and sexual and continence outcomes) is lacking. Other issues that narrow women's choices around childbirth in some countries are not addressed by the profession. De Mello E Souza points out that tubal ligation is illegal and thus can be done only surreptitiously during a caesarean in Brazil. In many hospitals, epidural pain relief is not allowed for vaginal birth.3
If the fashion for caesarean section spreads beyond healthy women with small families, this public health problem could grow into something far worse.1 We saw something similar when upper class women abandoned breast feeding last century. It is poorer families who continue to pay the enormous cost generations later. For a medical community and society that brings women to the point of preferring major surgery to childbirth, serious questions need to be asked—preferably before women start paying for this trend with their lives.
Footnotes
Competing interests None declared.
website extra Further details of sources of data for each country are available on the BMJ's website www.bmj.com