Grommets, tonsillectomies, and deprivation in Scotland
BMJ 1994; 308 doi: https://doi.org/10.1136/bmj.308.6937.1129 (Published 30 April 1994) Cite this as: BMJ 1994;308:1129
- Ann F Bisset,
- Daphne Russell
- Department of Public Health Medicine, Grampian Health Board, Aberdeen AB9 1RE
- Department of Public Health, University of Aberdeen.
- Correspondence to: Dr Ann F Bisset, Department of Public Health Medicine, Grampian Health Board, Summerfield House, 2 Eday Road, Aberdeen AB9 1RE.
- Accepted 7 February 1994
Abstract
Objective: To see whether there is a relation between grommet insertion operation and tonsillectomy rates, otolaryngology services, and deprivation scores in Scotland.
Design: Analysis of routine 1990 NHS data on grommet insertions and tonsillectomies in Scottish children aged 0-15 years compared with data on general practitioner and otolaryngology services and Carstairs deprivation scores.
Setting: All 15 Scottish health boards. Subjects--All children aged 0-15 (1 021 933).
Results: Tonsillectomy was more common than grommet insertion operations in Scotland (6182:4850). Health boards with high grommet insertion rates were more likely to have low tonsillectomy rates (Spearman's rank correlation -0.59; 95% confidence interval -0.87 to -0.03). Grommet insertion rates varied fourfold (from 2.4/1000 to 9.2/1000) and tonsillectomy rates twofold (from 3.6/1000 to 8.0/1000) across Scottish health boards. Variation between health boards had changed over the 15 years 1975-90. Variation in grommet insertion rates did not reflect variation in the supply of otolaryngology consultants (Spearman's rank correlation -0.25). There was a non-significant tendency for high general practitioner referral rates to be associated with high grommet insertion rates, low tonsillectomy rates, and less deprived areas (Spearman's rank correlation coefficients 0.50, -0.53, and -0.43). Deprivation (measured by Carstairs scoring for each health board) was associated with higher tonsillectomy rates (Spearman's rank correlation 0.41; 95% confidence interval -0.22 to 0.80) and significantly lower grommet insertion rates (-0.73; -0.92 to -0.28). Conclusion--Social factors as well as differences in disease prevalence and medical practice need to be considered when studying variation in childhood grommet insertion and tonsillectomy rates.
Public health implications
Public health implications
Grommet insertion rates for children vary fourfold across Scottish health boards; tonsillectomy rates vary twofold
The relative importance of the two operations has varied with time; in 1990 grommet insertion rates exceeded tonsillectomy rates only in the seven boards with the highest grommet insertion rates
Health boards with less deprivation tend to have lower tonsillectomy rates but significantly higher grommet insertion rates
Surgical practice varies widely among health boards
Guidelines for effective surgery should allow for social variation and ensure that appropriate information is given to parents
Introduction
In 1974 a review of adenotonsillectomy suggested that “while variations in operations persist on a geographical basis, variations according to social class have almost disappeared.”1 Much published work on tonsillectomies from 1950 to 19802 expressed similar concerns to later work on grommets, particularly the high rates in middle class children, the preponderance of boys, large regional variations in surgical rates,3 and the lack of clear evidence of long term benefit.4
By 1984 surgery for glue ear was described as an “epidemic.”3 This epidemic had arisen as adenotonsillectomy rates had fallen and had become the commonest reason for surgery in children in England.3 The relative risk of grommet surgery was 1.16 in social class I compared with 0.61 in class V, and rates were higher in boys. Later attempts to produce effective guidelines for glue ear surgery and screening,4 5 however, concentrated on clinical aspects of glue ear, rather than studying glue ear surgery in a wider social context.
This study aimed at describing grommet insertion and tonsillectomy rates in Scotland in 1990 and at finding whether there was a relation between grommet insertion and tonsillectomy rates, otolaryngology services, and deprivation scores.
Method
The study used the Scottish morbidity records (SMR1), generated for all non-obstetric and nonpsychiatric discharges from NHS hospitals in Scotland. The criterion for inclusion was a procedure code for inserting grommets or tonsillectomy, occurring between 1973 and 1991. Unless stated otherwise figures refer to children aged 0 to 15 years, who accounted for 92% of the grommet insertion episodes and 68% of the tonsillectomies.
Outpatient data from the recently introduced Scottish morbidity records 0 (SMR0) became available only in 1991. These gave total numbers of first time referrals of patients aged 0-15 to otolaryngology clinics by health board of residence but no details of symptoms or diagnosis. The Information and Statistics Division of the Scottish Health Service Common Services Agency provided summary statistics for each health board.
Statistical data on private operations in Grampian were supplied by the manager of the only private hospital in Aberdeen.
Rates were analysed by using population estimates issued by the General Register Office for Scotland (population statistics branch) for denominators. Three and five year average rates were also calculated and confirmed that 1990 rates and figures were comparable with data for other recent years. Carstairs deprivation scores6 based on 1991 census data were produced by the public health research unit of the University of Glasgow. Statistical analysis was performed on a microcomputer. X2 Values were calculated by using the SPSS-PC+7 and confidence intervals for relative risks and rank correlation coefficients by using the confidence interval analysis program.8 Island health boards were excluded from statistical analysis because of small numbers.
Results
OPERATION RATES
A total of 4850 grommet insertion operations were carried out in Scotland in 1990 on 0-15 year olds, giving a rate of 4.7/1000; 6182 tonsillectomies were performed on the same population (rate 6.0/1000).9 Only in the age group 0-3 years were grommet insertions (1037 operations) commoner than tonsillectomies (532 operations).
Grommet insertion rates by health board of residence showed a highly significant fourfold variation--namely, from 2.4/1000 in Greater Glasgow (437 operations) to 9.2/1000 in Grampian (938 operations) (overall X2 with 14 degrees of freedom = 940; relative risk in Grampian compared with Glasgow 3.83 (95% confidence interval 3.42 to 4.28).

Grommet insertion and tonsillectomy rates in Scotland during 1975-90 (0-15 year olds)
{kind=link}
Tonsillectomy rates for 0-15 year olds in 1990 varied from 3.6/1000 in Tayside (273 operations) to 8.0/1000 in Greater Glasgow (1460 operations). Boards with high grommet insertion rates tended to have low tonsillectomy rates, though the association was only just significant (Spearman's rank correlation -0.59 (95% confidence interval -0.87 to -0.03); table I).
Deprivation score and grommet insertion and tonsillectomy rates
Variation in grommet surgery rates showed no simple geographical pattern. The two boards with the highest rates were in north east and south west Scotland and there was no urban-rural pattern. For tonsillectomy the two highest rates were in those boards with the largest cities (Glasgow and Edinburgh).
Some 8.7% (422/4850) of grommet insertion operations were combined with tonsillectomy at the same operation. When Forth Valley (3.8%; 13/346) and Dumfries and Galloway (13.7%; 33/241) were excluded there was no significant difference between boards. Adenoidectomy was combined with 33% (1621/4850) of grommet insertions (range across health boards 9% to 52%) and 67% (4132/6182) of tonsillectomies (range across health boards 51% to 79%).
In Grampian, taken as an example, operations in private hospitals increased the number of grommet insertions (all ages) by 136 (13%) to 1194 and tonsillectomies by 101 (11%) to 1059.
TIME TRENDS
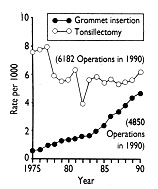
Analysis of Grampian Health Board, which had the highest grommet insertion operation rate in Scotland in 1990, confirmed the findings of Black in 1984.3 The tonsillectomy rate declined from 9.3/1000 (951 operations) in 1975 to 5.6/1000 (575 operations) in 1990 whereas in the same period there was an increase in grommet insertion rates from 3.1/1000 (313 operations) to 9.2/1000 (938 operations) (fig 2). Over the 15 years, however, the pattern for the seven health boards with the highest grommet insertion rates became different from that for Scotland, and particularly from that for Greater Glasgow Health Board, which had the lowest grommet insertion rate (figs 3 and 4). Tonsillectomy rates in Scotland showed only a modest decline and continued to exceed grommet insertion rates, which increased slowly.

Grommet insertion and tonsillectomy rates in Scotland during 1975-90 (0-15 year olds)
{kind=link}
Grommet insertion and tonsillectomy rates in Scotland during 1975-90 (0-15 year olds)
{kind=link}

Grommet insertion and tonsillectomy rates in Glasgow during 1975-90 (0-15 year olds)
{kind=link}
REPEAT OPERATIONS
Tonsillectomy is normally performed only once. Analysis by the Information and Statistics Division of patients having grommet insertion operations for the first time between 1975 and 1986 found a cumulative grommet reoperation rate for patients in Scotland of 8.7% at one year, 19.0% at two years, 23.2% at three years, and 25.1% at four years. Reoperation rates have risen steadily, and the maximum number of grommet insertion operations per child reached 14 for one child in 1991.10 Repeat operations accounted for 40% (378/938) of all grommet insertion procedures in Grampian in 1990. Routine data, however, did not include the type of grommet used or whether the initial procedure was unilateral or bilateral.
WAITING TIMES
The median waiting times for grommet insertion and tonsillectomy in Scotland in 1990 were both two months. Five per cent (262/4836) of grommet recipients and 12% (726/5918) of tonsillectomy patients waited more than six months. (These denominators are less than the total numbers of operations because patients treated urgently were not placed on a waiting list before operation.) There was no association between grommet insertion rates and waiting times.
OUTPATIENT REFERRALS
General practitioner referrals to otolaryngology clinics for children aged 0-15 years ranged from 20/ 1000 in Lanarkshire to 40/1000 in Tayside. There was a non-significant tendency for high referral rates to be associated with high grommet insertion rates, low tonsillectomy rates, and less deprived areas (Spearman's rank correlation coefficients 0.50, -0.53, and -0.43).
OTOLARYNGOLOGY SURGEONS
The annual number of grommet insertion operations performed under the care of individual consultants varied across Scotland in 1990 (range one to 429 operations per consultant). The number of otolaryngology consultants per head of total population bore no relation to grommet insertion rates for that board (Spearman's rank correlation -0.25 (95% confidence interval -0.74 to 0.42); table II).
Otolaryngology consultants per head of population (all ages)
AGE AND SEX
The age distribution at operation was unimodal and positively skewed for both grommet insertions and tonsillectomies. The mean age for grommet insertion was 6 years 2 months (SD 2 years 11 months) and the median age 5 years 9 months. The age distribution varied between boards, though there was no apparent pattern to the variation--for example, Grampian treated half of all Scottish grommet recipients aged under 1 year (compared with 19% of those operated on aged 1-15 years); Lothian, with the sixth highest overall grommet insertion rate, performed a higher proportion (25%) of its operations on under 3s than any other board. For tonsillectomies in Scotland the mean age was 7 years 10 months (SD 3 years 5 months) and median age 6 years 11 months.
In 1990, 56% of 0-15 year olds fitted with grommets11 and 46% of 0-15 year olds having a tonsillectomy were boys.
SOCIAL CLASS AND DEPRIVATION
Social class data on hospital patients are not routinely collected in Scotland. Deprivation scores have been calculated by Carstairs and Morris for postcode sectors and healthboards6 using census data for overcrowding, male unemployment, low social class, and no car as variables. There was a highly significant negative correlation between deprivation score and grommet insertion rate (Spearman's rank correlation -0.73; 95% confidence interval -0.92 to -0.28). The correlation with tonsillectomy was positive but not significant (0.41 (-0.22 to 0.80); table I).
Discussion
In contrast with England and Wales,3 4 tonsillectomy was more common than grommet surgery in Scottish children. This study found considerable regional variation in all aspects of both operations, with a changing pattern among boards during 1975-90. Comparisons across Scotland gave a very different perspective from studying operations only where they were common (and therefore a “problem”; figs 2-4), but explanations for this variation are complex.
MEDICAL EXPLANATIONS
A recent Dutch study found a clear distinction between children who suffer from tonsillitis and those who suffer from acute otitis media but a less clear cut distinction between tonsillitis and glue ear.12 General practitioners' referral rates reflect differences in prevalence and in the behaviour of parents*RF 13-15* or general practitioners2 13 or both. This study found that high general practitioner referral rates did not result in more tonsillectomies and explained only a small part of the wide variation in grommet insertion rates.
The variation in annual number of grommet insertion operations per surgeon indicated that individual surgeons may affect surgical rates,2 15 16 though detailed investigation of case mix would be necessary to confirm this. Otolaryngologists noted that several consultants in the boards with the highest rates of grommet insertion had completed their training in the board with the highest rate.9 We found no correlation between the number of consultant otolaryngologists per head of total population and grommet insertion rates but did not examine consultants' case mix or junior staff.
Surgical practice varied. Combinations with other operations, age at operation, repeat rates, and waiting times all varied across Scottish health boards. Each factor alone accounted for only a small part of the variation in grommet insertion rate, but the interaction of factors was complex.
Waiting times could influence surgical rates at an age when children are outgrowing glue ear4 17 18 and tonsillitis, and three months of “watchful waiting” before grommet surgery has been advocated.4 5 18 The median waiting time for grommet surgery in Scotland was two months. This could increase surgical rates unless the criteria for admission to the waiting list included a period of waiting to ensure persistence and retesting of hearing immediately before operation.18 19 There was no evidence that grommet insertion rates were related to waiting lists.
SOCIAL EXPLANATIONS
Deprivation has proved more useful than social class for explaining variation in health.6 Tonsillectomy rates were higher in health boards with greater deprivation whereas grommet insertion rates were significantly lower. Other studies have shown that tonsillectomies for upper class children became less popular when parents became aware of medical opinion that the operation offered few benefits, except for carefully selected children.1 2 There are social parallels between use of grommets and tonsillectomy, but the long term effect of hearing on development is still uncertain, making selection of surgical cases difficult.18 20
Parents influence the way a child is presented to medical services2 21--for example, taking a child to the general practitioner, attending screening sessions and follow up appointments, giving an account of the child's symptoms and their impact on the family.1 This is affected by social class,2 22 what the parent perceives to be expected behaviour,13 and reinforcement by medical staff.2 15 16 These latter influences are stronger in areas where surgery is common.15
Conclusion
Social variation needs to be addressed as a factor, together with disease prevalence and medical services, which affect variation in childhood surgical rates. Inequalities in Scottish health and mortality have widened over the past 15 years23 and chronic tonsillitis may be more prevalent in areas with high deprivation owing to poor nutrition and living conditions. Government fiscal intervention to reduce differentials in wealth might prevent some of this real variation.
For glue ear geographical variation in prevalence is uncertain, and the strong correlation between high surgery rates and social advantage may be influenced by parents. Improving information to parents19 about the natural (usually benign18) course of glue ear may contribute to ensuring effective surgery as part of “developing protocols with relevant professionals.”4 Advice to parents should emphasise the importance of hearing assessment4 5 18 (which should be repeated before surgery)4 and the possible alternatives to surgery. The fluctuating deafness characteristic of glue ear makes assessment difficult,18 but this should not be used as an excuse for omitting objective assessment of hearing disability. Purchasers need to ensure that there are enough resources and staff for this assessment.4
In summary, this study shows that social factors are associated with surgical rates and need to be considered when assessing the effectiveness of grommet surgery and tonsillectomy for children.
We are grateful to Edwin Alexander, Scott Sim, and Fred Nimmo, of Grampian Health Board; Dr J Clarke, Adam Redpath, and David Murphy, of the Information and Statistics Division of the Common Services Agency of the Scottish Health Service, for supplying data; Moira Napper, librarian; P McLoone, of the Public Health Research Unit, Glasgow, for the 1991 deprivation scores; Professor G G Browning, Glasgow, Professor E M Russell and Dr N Waugh, Grampian, and all the ENT surgeons who gave advice.