Patient relevant outcomes of unicompartmental versus total knee replacement: systematic review and meta-analysis
BMJ 2019; 364 doi: https://doi.org/10.1136/bmj.l352 (Published 21 February 2019) Cite this as: BMJ 2019;364:l352
- Hannah A Wilson, research fellow1,
- Rob Middleton, research fellow1,
- Simon G F Abram, research fellow1,
- Stephanie Smith, postdoctoral research fellow1,
- Abtin Alvand, consultant orthopaedic surgeon1,
- William F Jackson, consultant orthopaedic surgeon2,
- Nicholas Bottomley, consultant orthopaedic surgeon2,
- Sally Hopewell, associate professor3,
- Andrew J Price, professor of orthopaedic surgery1
- 1University of Oxford, Nuffield Department of Orthopaedics Rheumatology and Musculoskeletal Sciences, BOTNAR Research Centre, Headington, Oxford OX3 7LD, UK
- 2Oxford University Hospitals NHS Trust, Nuffield Orthopaedic Centre, Oxford, UK
- 3Centre for Statistics in Medicine, Oxford Clinical Trials Research Unit, Oxford, UK
- Correspondence to: H A Wilson hannah.wilson{at}ndorms.ox.ac.uk
- Accepted 14 January 2019
Abstract
Objective To present a clear and comprehensive summary of the published data on unicompartmental knee replacement (UKA) or total knee replacement (TKA), comparing domains of outcome that have been shown to be important to patients and clinicians to allow informed decision making.
Design Systematic review using data from randomised controlled trials, nationwide databases or joint registries, and large cohort studies.
Data sources Medline, Embase, Cochrane Controlled Register of Trials (CENTRAL), and Clinical Trials.gov, searched between 1 January 1997 and 31 December 2018.
Eligibility criteria for selecting studies Studies published in the past 20 years, comparing outcomes of primary UKA with TKA in adult patients. Studies were excluded if they involved fewer than 50 participants, or if translation into English was not available.
Results 60 eligible studies were separated into three methodological groups: seven publications from six randomised controlled trials, 17 national joint registries and national database studies, and 36 cohort studies. Results for each domain of outcome varied depending on the level of data, and findings were not always significant. Analysis of the three groups of studies showed significantly shorter hospital stays after UKA than after TKA (−1.20 days (95% confidence interval −1.67 to −0.73), −1.43 (−1.53 to −1.33), and −1.73 (−2.30 to −1.16), respectively). There was no significant difference in pain, based on patient reported outcome measures (PROMs), but significantly better functional PROM scores for UKA than for TKA in both non-trial groups (standard mean difference −0.58 (−0.88 to −0.27) and −0.29 (−0.46 to −0.11), respectively). Regarding major complications, trials and cohort studies had non-significant results, but mortality after TKA was significantly higher in registry and large database studies (risk ratio 0.27 (0.16 to 0.45)), as were venous thromboembolic events (0.39 (0.27 to 0.57)) and major cardiac events (0.22 (0.06 to 0.86)). Early reoperation for any reason was higher after TKA than after UKA, but revision rates at five years remained higher for UKA in all three study groups (risk ratio 5.95 (1.29 to 27.59), 2.50 (1.77 to 3.54), and 3.13 (1.89 to 5.17), respectively).
Conclusions TKA and UKA are both viable options for the treatment of isolated unicompartmental osteoarthritis. By directly comparing the two treatments, this study demonstrates better results for UKA in several outcome domains. However, the risk of revision surgery was lower for TKA. This information should be available to patients as part of the shared decision making process in choosing treatment options.
Systematic review registration PROSPERO number CRD42018089972.
Introduction
Partial or unicompartmental knee arthroplasty (UKA) and total knee arthroplasty (TKA) are well established treatment options for end stage medial compartment osteoarthritis, in patients in whom conservative management options have failed.1 An estimated 25-47% of patients who are eligible for primary joint replacement in the United Kingdom have isolated unicompartmental osteoarthritis, and would be eligible to receive either implant.234 However, the rate of implantation of UKA in the UK remains static at around 8% of all primary knee joint arthroplasties, and varies enormously both geographically and between centres in the same region.5 This is likely to reflect the fact that only 38% (n=651) of the 1715 clinicians who reported performing total knee arthroplasty to the UK National Joint Registry in 2017 also performed UKA.5
The debate regarding UKA or TKA as the treatment of choice for eligible patients continues.1 The higher revision rates for UKA than for TKA, as reported in national joint registries and a recent meta-analysis,6 particularly in younger patients, is thought to be a key factor in explaining why more knee surgeons do not perform both procedures.7 But recent literature has shown that the higher failure rates of UKA are associated with centres and surgeons performing low numbers of the procedure.89101112 Some evidence in the UK also suggests that UKA has significant advantages over TKA, with fewer serious medical complications, reduced mortality rates, faster recovery, and superior functional outcome.131415
In reality, when considering between two recognised treatment options for the same condition, the decision should be shared between the patient and the clinician.16 Many medical decisions can only be made once both parties are able to understand and compare the risks and benefits of both treatment options.161718 A wide range of outcomes, relative risks, and potential benefits of each treatment option must be understood and applied to each individual patient. If the full spectrum of outcomes is not considered, then patients cannot be considered as fully informed.1920 When deciding whether to undergo knee arthroplasty surgery, several key outcome domains are important to patients, such as speed of recovery, return to work, revision, complications, mortality, and functional outcomes.1321222324 Data regarding these outcome domains have been reported in the literature, but very few randomised controlled trials and few of the published studies’ methodologies have compared TKA with UKA for multiple outcomes. A recently completed James Lind Alliance priority setting partnership identified the issue of describing outcomes and offering information to patients as a priority for future research.25
Systematic review methodology, with meta-analysis, allows comparison of UKA and TKA across several outcome fields. Previous systematic reviews have used small numbers of studies, using only data from randomised controlled trials26 or using data from studies investigating UKA or TKA individually, often focusing on clinician orientated outcome measures.2728 In the present study, we expanded inclusion criteria beyond trials to include other study methodologies, such as registry and multicentre database analyses and large cohort studies. As a result, it was possible to study more outcome domains, and include outcome data from far more procedures.
These studies presented data collected with such different methodologies that they could not be included in one analysis. Therefore, in the current study, we created three groups of studies: group 1 including data from randomised controlled trials, group 2 including data from national joint registries and large nationwide multicentre databases, and group 3 including data from large cohort studies. Therefore, for each domain of outcome, three separate analyses were presented simultaneously where possible. Therefore, if there was a statistically significant agreement across all the study groups, we thought that this would present a compelling result when comparing the two implant types. If there was disagreement between the groups of studies, the relevant limitations of each groups’ data and or study methodologies could then be considered.
The aim of the present study was to provide a synthesis of evidence from randomised controlled trials, registries and nationally reported databases, and cohort studies, in all outcome domains identified as important by patients undergoing UKA or TKA. This evidence was to enable informed shared decision making in the care of patients when choosing an implant to treat unicompartmental osteoarthritis of the knee.
Methods
This study was conducted in accordance with the MOOSE (meta-analysis of observational studies in epidemiology)29 and PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines.30
Literature search and selection of studies
We conducted a systematic search of Medline, Embase, Cochrane Controlled Register of Trials (CENTRAL), and Clinical Trials.gov, to identify relevant studies published in English between 1 January 1997 and 31 December 2018. The search was limited to studies published in the past 20 years, in order to focus on studies involving modern implants. We excluded conference abstracts and case reports unless they had subsequently been published as full articles. The search strategy is described in appendix 1.
Studies were initially selected on the basis of their title and abstract by two independent authors (HAW and RM). In the case of any disagreement or uncertainty, full papers were retrieved and reviewed, and discussed with a third author (AP). We included randomised controlled trials, retrospective analyses of large national or multicentre databases or joint registries, and large cohort studies. The search was limited to studies that directly compared outcomes of UKA and TKA, in adult patients (age ≥18 years). Studies focusing on the isolated patellofemoral joint or isolated lateral compartment osteoarthritis were also excluded. To avoid overestimating any outcome, we required each study to include a minimum of 50 participants. Studies were also required to have a minimum follow-up of 30 days if assessing an adverse event, or a minimum of six months if assessing outcome data. Studies were excluded if the data presented were insufficient to pool for statistical analysis. Where possible, non-English studies were translated and included into the study. Supplementary table 1 lists a summary of all studies included and their key features.
Selection of domains of outcomes to be investigated
The outcome measures were identified after discussion groups in our unit, with patients who had previously undergone knee arthroplasty surgery. We also took into account the most commonly used measures of outcome from recent publications. Domains included:
Hospital admission impact: length of operation and length of hospital stay
Risk of early complications (myocardial infarction, stroke, venous thromboembolism, or deep infection) or early mortality
Success of operation: range of movement achieved or kneeling ability, reduction in pain, improvement in function
Reoperation or revision rate
Rate of recovery: rate of return to work, rate of return to sporting activities.
We found agreement on the most important outcome domains between the literature search and the patient discussion group. The patient’s discussion group valued information such as return to work and sporting activities more highly, and also suggested inclusion of information regarding length and acceptability or appearance of the operative scar. Furthermore, the literature search demonstrated multiple studies comparing differences in implant design, surgical approach, blood loss or transfusion rates, and cost effectiveness of UKA versus TKA.31323334 These aspects of surgical technique and implant implications were not included in the analysis of this study because we believed that they would not ordinarily be considered when informing patient decision making.
Data extraction
Data were extracted by use of standardised forms. Two authors (HW, RM) independently extracted the data from all included studies. Where available, data recorded included general study characteristics such as the name of the lead investigator and year of publication, recruitment period, median duration of follow-up, number of participants, and mean age and sex of the participants. Furthermore, the primary outcome measures and adverse event data were extracted (appendix 1b, supplementary figures).
Studies were initially categorised into three groups: randomised controlled trials (group 1), national or large multicentre database or joint registry studies (group 2), and large cohort studies (group 3). There were insufficient numbers of studies providing data that were adequately adjusted to be analysed separately, mainly because studies often did not adjusted for grade or stage of osteoarthritis, as well as for age, sex, and health status. If data presented were incomplete, efforts were made to contact the corresponding author for further information.
Risk of bias
We assessed risk of bias using the Cochrane collaboration’s tool for assessing risk of bias for randomised controlled trials,35 stratifying the risk as high, unclear, or low risk in a traffic light configuration for random sequence generation, allocation concealment, blinding of participants, blinding of outcome, and attrition bias. Assessments are reported in supplementary table 2. For the study groups 2 and 3, we used the Newcastle-Ottawa scale36 to assess studies in four key areas, including selection and comparability of cohorts, and outcome assessment and follow-up. Each domain of risk was again classified into low, unclear, or high risk, and presented in a summary table (supplementary table 3).
Statistical analysis
We calculated the overall summary estimates using inverse variance weighted random effects meta-analysis. Individual relative risk estimates and summary estimates were displayed graphically in forest plats. Heterogeneity was quantified with the I2 statistic and Q test. Analysis could not be carried across the different types of study owing to the significant difference in their design. Therefore, for each outcome, data from each type of study were presented sequentially as randomised controlled trials, registry studies, and then large cohort studies. If no data were presented in one or more of the groups of publications for an outcome, we commented on this.
Patient and public involvement
Patient discussion groups were used as a means of involving patients in setting the research question and for determining the outcome measures. Patients were not asked to advise on the study interpretation or participate in the writing up of results. Patients will not be involved in the dissemination of results.
Results
Of 1289 studies eligible for inclusion in the abstract screen, 1201 were excluded for not meeting the inclusion criteria and repetition. After full text review, a further 28 studies were excluded,32343738394041424344454647484950515253545556575859606162 and 60 were included in the final analysis (fig 1).

Flowchart of studies reviewed and included for each analysis. Data were included from 60 studies, several of which contributed to analyses for several domains of outcome. ROMS=range of motion; PROMs=patient reported outcome measures
{kind=link}
Group 1 included seven publications. Of five primary randomised controlled trial papers,63646566 two included patients who underwent a TKA in one knee and a UKA in the contralateral leg,6465 and one included patients who received either simultaneous bilateral UKA or TKAs.67 The remaining two publications were subsequent reports.6869 This allowed a maximum analysis of 898 implants in 764 patients from the trial data.
Group 2 included 12 publications from seven national joint registries813142370717273747576777879 and five multicentre database studies.8081828384 The non-national joint registry studies were included in this group because their data collection methods and patient cohorts were more akin to registry studies than cohort studies. Examples include studies in which data were requested to answer specific research questions from an established database, data were collected from multiple hospitals and from different clinicians, and different implants were used with no control on operative technique or postoperative care. Some data on the same procedures were presented in different studies as part of different cohorts, so we were unable to calculate the actual number of procedures.
A further 36 cohort studies were included in group 3. Of these studies including data comparisons between UKAs and TKAs,153182858687888990919293949596979899100101102103104105106107108109110111112113114 only five included data specifically in patients with anteromedial osteoarthritis.158599103111 Again, we saw some crossover in the data presented from the same unit in multiple papers, but the maximum number of implants was 26 418. Of the 60 studies included in the final analysis, 14 reported on length of operation, 21 on length of hospital stay, 24 on complication rates, 11 on early mortality rates, 17 on range of motion and kneeling ability, 31 on patient reported outcome measures (PROMs), 13 on reoperations, 28 on revision rates, and four on return to work (fig 1).
Outcomes
For each outcome measure, data from study groups 1-3 were presented sequentially, for ease of comparison. If no data or inadequate data were available at any level, it was represented by a zero in the results table. For ease of interpretation, all the outcome data were presented in forest plots with UKA favourable results presented on the left hand axis and TKA favourable results on the right hand axis. A summary of all data analyses are presented in table 1.
Summary of all analyses for study groups in comparison between outcomes of unicompartmental versus total knee replacement
Domain 1: hospital admission impact
Operation duration
Fourteen studies involving a maximum of 3262 UKA and 53 989 TKA procedures reported results for length of operation. “Operation duration” was often not defined in the studies, but all times were recorded in minutes. In group 1, data from three randomised controlled trials656667 showed no difference in operating times between UKA and TKA (mean difference −1.72 minutes, 95% confidence interval −11.89 to 8.45). Data from group 2 included two studies,8183 with a corresponding mean difference of −3.21 minutes (−6.33 to −0.09). Data from nine cohort studies15449598104106111115116 were included in group 3, which showed a significantly shorter operation duration for UKA than for TKA (mean difference −23.80, −37.81 to −9.79; supplementary figure 1).
Length of hospital stay
Length of hospital stay was reported by 21 studies. Although the recording method was also often not described in the papers, the outcome was measured as number of days spent in hospital. Data were included from a maximum of 47 960 UKA and 547 275 TKA procedures. All levels of analysis reported a significantly shorter hospital stay after UKA than TKA. In group 1, one randomised controlled trial67 showed a mean difference of −1.20 (95% confidence interval −1.67 to −0.73). The group 2 analysis included data from five studies,73768182838493 which showed a mean difference of −1.43 (−1.53 to −1.33). In group 3, data from 13 cohort studies154494959698101104105106107115116117118 showed a mean difference of −1.73 (−2.30 to −1.16; supplementary figure 2).
Domain 2: early complications
Myocardial infarction or cardiac events
Seven studies specifically reported myocardial infarction as an outcome measure. No study satisfactorily characterised what constituted a cardiac event, but we included all events reported. Data were included from a maximum of 32 263 UKA and 180 275 TKA procedures in this analysis. We saw a significantly lower rate of myocardial infarction after UKA than TKA in groups 1 and 2, but no significant difference in group 3. In group 1, data from one randomised controlled trial119 showed a risk ratio of 0.33 (95% confidence interval 0.01 to 8.14). In group 2, data from four studies814818284 showed a risk ratio of 0.22 (0.06 to 0.86). In group 3, data from two cohort studies9094 showed a risk ratio of 1.45 (0.46 to 4.55; fig 2).
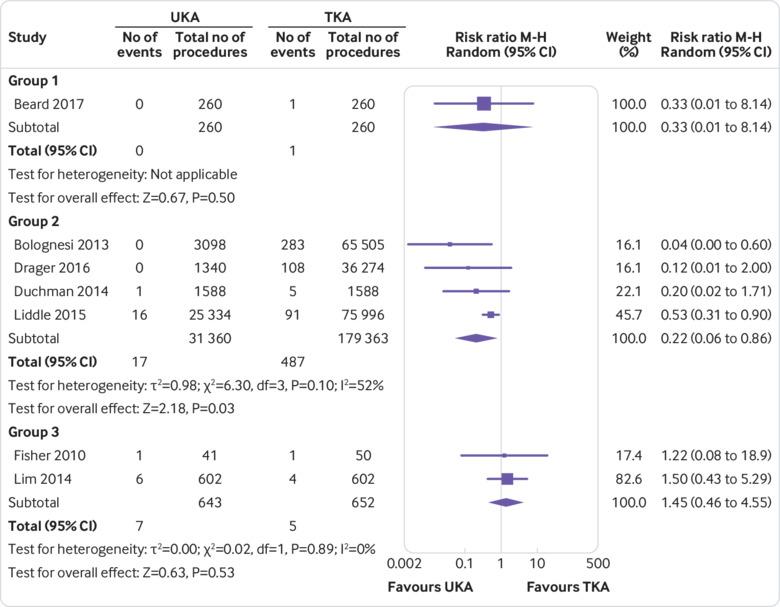
Forest plot comparing risk of myocardial ischaemic events after unicompartmental (UKA) versus total knee replacement (TKA). Also appears in the supplementary material as supplementary figure 3. M-H=Mantel-Haenszel test
{kind=link}
Cerebrovascular events
Data were presented in only two comparative studies regarding risk of stroke, but still included data from 26 922 UKA and 77 583 TKA procedures. The analysis showed a significantly reduced risk of cerebrovascular accidents after UKA (supplementary figure 4). Group 1 studies presented no relevant data. Data from two studies1481 were included in group 2, which showed a risk ratio of 0.34 (95% confidence interval 0.15 to 0.74). No data were available for inclusion from cohort studies in group 3.
Venous thromboembolism (deep vein thrombosis and pulmonary embolus)
Data from 11 studies were included regarding incidence of venous thromboembolism (both deep vein thrombosis and pulmonary embolus) after TKA and UKA, including a maximum of 33 232 UKA and 229 166 TKA procedures. Methods of confirming venous thromboembolism were not always detailed in all of the studies included. All groups of analysis showed a trend that risk of venous thromboembolism was higher after TKA than UKA (fig 3), but this trend was only significant in group 2. In group 1, data from two studies6566 showed a risk ratio of 0.24 (95% confidence interval 0.04 to 1.37). Data from five studies1481828384 were included in group 2, showing a risk ratio of 0.39 (0.27 to 0.57). In group 3, data from four cohort studies101104107112 showed a risk ratio of 0.49 (0.20 to 1.17).

Forest plot comparing risk of venous thromboembolism after unicompartmental (UKA) versus total knee replacement (TKA). Also appears in the supplementary material as supplementary figure 5. M-H=Mantel-Haenszel test
{kind=link}
Deep infection
A total of 15 studies reported incidence of deep infection after UKA or TKA, including data from a maximum of 23 274 UKA and 259 299 TKA procedures (supplementary figure 6). Deep infection was classified as infection that requires further intervention—ether revision, reoperation (debridement and implant retention), or long term suppressive antibiotics. We did not include superficial wound infections because they were frequently reported inconsistently or not reported. In group 1, data were presented from only one randomised controlled trial66 but no deep infections were reported. In group 2, data from six studies717579818284 showed a reduced rate of infection after UKA, with a risk ratio of 0.59 (95% confidence interval 0.43 to 0.82). Data from eight cohort studies15858691949697111 were included in group 3, which showed a risk ratio of 0.40 (0.16 to 1.01).
Early mortality
We included all cause mortality reported within the first 45 days after the procedure; 10 studies were included, with a maximum of 73 585 UKA and 696 778 TKA procedures. TKA was associated with a significantly higher risk of early mortality than UKA in the one group of studies that supplied sufficient data (fig 4). In group 1, four randomised controlled trials63646566 reported no early mortalities, and so could not be included in the analysis. Data from six studies131481828384 were included in group 2, showing a risk ratio of 0.27 (95% confidence interval 0.16 to 0.45). In group 3, data for this domain were reported in one cohort study,104 but also did not show any early mortalities, and so could not be included in the analysis.

Forest plot comparing risk of early mortality (at 45 days) after unicompartmental (UKA) versus total knee replacement (TKA). Also appears in the supplementary material as supplementary figure 7. M-H=Mantel-Haenszel test
{kind=link}
Domain 3: success of operation
Range of movement
Seventeen studies reported postoperative range of movements in degrees for a maximum of 2541 UKA and 3848 TKAs; several studies reported only the improvement or difference in range of movement, which could not be included because the data were not comparable. The studies included showed a greater range of movement after UKA than TKA, but the results were only significant in groups 2 and 3 (supplementary figure 8). In group 1, data were presented from three randomised controlled trials,636568 which showed a mean difference of −4.58 degrees (95% confidence interval −10.75 to 1.59). Data from one study95 could be included in group 2, which showed a mean difference of −5.00 degrees (−7.28 to −2.72). Data from 13 cohort studies15548586879091959699104106111 in the group 3 analysis showed an overall mean difference of −8.71 degrees (−11.77 to −5.64).
Kneeling ability
Only two studies that reported kneeling ability after TKA and UKA could be included in this analysis using our selection criteria. This inclusion allowed analysis of 712 UKA and 715 TKA procedures at varying time points postoperatively. These studies showed a greater risk of patients not being able to kneel after TKA than after UKA (supplementary figure 9). No studies were eligible for inclusion that presented data on kneeling ability in groups 1 or 2. In group 3, the two cohort studies included8587 showed a risk ratio of 0.53 (95% confidence interval 0.28 to 1.01).
Patient reported outcome measures (PROMs)
PROM scores were included in the analysis if reported at a minimum of six months’ follow-up after the procedure, and those scores recorded at the greatest possible time points were included in the analysis. We included all studies presenting more than one score. For simplicity, all scores were transformed so that a higher score reflected a better outcome.
Combined scores—These combined PROMS scores included the Oxford knee score, Bristol knee score, Western Ontario and McMaster Universities index, Knee Society score, and the Japanese Orthopaedic Association score. Thirty seven postoperative combined PROM scores was reported in 29 studies, allowing analysis of a maximum of 30 514 PROMs after UKA and 25 657 PROMs after TKA. In all levels of analysis, significantly better PROM scores were recorded after UKA than after TKA (fig 5). Data presented from six randomised controlled trials636465666769 were included in the group 1 analysis for this domain (standard mean difference −0.19 (95% confidence interval −0.32 to −0.05)). In study group 2, data from five studies7072889298 showed a standard mean difference of −0.05 (−0.25 to 0.15). In group 3, data from 18 cohort studies15548689909194959699100103105106108112120 showed an overall standard mean difference of −0.19 (−0.31 to −0.06).

Forest plot comparing combined pain and function measured using knee specific patient reported outcome measures after unicompartmental (UKA) versus total knee replacement (TKA). Also appears in the supplementary material as supplementary figure 10. IV=inverse variance weighting; OKS=Oxford knee score; JKSC=Japanese knee osteoarthritis score; WOMAC=Western Ontario McMaster Universities osteoarthritis index; KSS=Knee Society Score; JOA=Japanese orthopaedic association score
{kind=link}
Pain scores—Eleven studies reported outcomes on a maximum of 3916 UKA and 11 624 TKA procedures, and reported either pain specific scores or the pain element of a larger combined PROM score. PROM scores were collected from various time points after the operation. Pain specific PROM scores were found to be equivocal after UKA compared with TKA in all study groups (supplementary figure 11). In group 1, data were presented from two randomised controlled trials6869 (standard mean difference −0.30, 95% confidence interval −0.63 to 0.03). In group 2, data from five studies7488929597100 showed a standard mean difference of −0.23 (−0.46 to 0.00). Data from four cohort studies96108110121 in the group 3 analysis showed an overall standard mean difference of −0.08 (−0.35 to −0.20).
Function scores—Sixteen studies, including a maximum of 3011 UKA and 10 470 TKA procedures, reported either function specific PROM scores or the function element of a larger combined PROM score. A higher score related to a better clinical outcome. In this analysis, significantly higher functional PROM scores were achieved after UKA than after TKA in groups 2 and 3, but the difference was not significant in group 1 (supplementary figure 12). In group 1, data were presented from two randomised controlled trials,6667 including three functional PROM scores, which showed a standard mean difference of −0.12 (95% confidence interval −0.12 to 0.04). In group 2, data from four studies7488929798 showed a standard mean difference of −0.58 (−0.88 to −0.27)). In group 3, data from 10 cohort studies5486909599100108112 showed an overall standard mean difference of −0.29 (−0.46 to −0.11).
Domain 4: need for further operations
Reoperation
Thirteen studies reported reoperation rates after TKA and UKA. These studies reported data from a maximum of 9662 UKA and 123 118 TKA procedures. Reoperation included any further procedure described in the study including manipulations under anaesthetic. Studies included in groups 1 and 2 showed no significant difference in reoperation rates between UKA and TKA, but group 3 data showed a higher reoperation rate after TKA than after UKA (fig 6). Data were presented in two randomised controlled trials6667 in the group 1 analysis, which showed a risk ratio of 0.73 (95% confidence interval 0.27 to 2.02). Data from five studies70818384122 in the group 2 analysis showed a risk ratio of 1.05 (0.75 to 1.46). In group 3, for this domain, data from six cohort studies909596101107111 showed a risk ratio of 0.45 (0.31 to 0.65).

Forest plot comparing risk of reoperation after unicompartmental (UKA) versus total knee replacement (TKA). Also appears in the supplementary material as supplementary figure 14. M-H=Mantel-Haenszel test
{kind=link}
Revision at five years
Seventeen studies reported revision data at five years, including data from 10 435 UKA and 171 460 TKA procedures. The revision rate at five years was significantly higher after UKA than after TKA at all levels of analysis (supplementary figure 15). Data from three randomised controlled trials636465 in the group 1 analysis showed a risk ratio of 5.95 (95% confidence interval 1.29 to 27.52). Data from two studies7182 in group 2 showed a risk ratio of 2.50 (1.77 to 3.54). Data from 11 cohort studies15868990959697101102111112 in the group 3 analysis showed a risk ratio of 3.13 (1.89 to 5.17).
Revision at 10 years
Thirteen studies reported revision data comparing a maximum of 25 526 UKA procedures with 209 751 TKA procedures at 10 years. Overall, UKA was associated with a higher revision rate than TKA in group 2 studies, equivocal in the group 3 studies, and was associated with a lower rate in one small group 1 trial (fig 7). Data from only one randomised controlled trial69 could be included in the group 1 analysis (risk ratio 0.64, 95% confidence interval 0.19 to 2.14). Data from eight studies included in group 273757678798097123124 showed a risk ratio of 1.85 (1.43 to 2.38). Group 3 included data from four cohort studies,85919497 which showed a risk ratio of 1.68 (1.07 to 2.64).

Forest plot comparing incidence of revision at 10 years after unicompartmental (UKA) versus total knee replacement (TKA). Also appears in the supplementary material as supplementary figure 16. M-H=Mantel-Haenszel test
{kind=link}
Revision at 15 years
Three studies presented data regarding revision rates or survival of UKA and TKA to 15 years, on a maximum of 6651 UKA and 132 168 TKA procedures. Revision rates were higher after UKA than TKA in group 2, but reported as lower in the one group 1 trial, although this group 1 result was not significant (supplementary figure 17). In group 1, the one randomised controlled trial69 reported revision rates at 15 years, showing a marginally lower revision rate after UKA than after TKA at this time point, with an overall risk ratio of 0.64 (95% confidence interval 0.19 to 2.14). Two group 2 studies7176 showed an overall risk ratio of 5.18 (1.39 to 19.22). No data were available from studies in group 3.
Domain 5: rate of recovery
Return to work or sport
Limited comparative studies were available for inclusion under our search criteria for speed of recovery, with several different methods of reporting speed of recovery. No data were available from studies in groups 1 or 2. Group 3 included two cohort studies3795 reporting the time rate (in weeks) of return to work after UKA or TKA, including data from 146 UKA and 156 TKA procedures. We saw a quicker return to work after UKA than after TKA (supplementary figure 18). The analysis from the two group 3 studies showed an overall mean difference of −0.96 (95% confidence interval −1.31 to −0.61). No data were presented from group 1 or 2 studies regarding the return to sport after UKA or TKA. In group 3, two cohort studies95110 could be included in the analysis, with results from 151 UKA and 155 TKA procedures. In the data presented, return to sport was marginally quicker after UKA than after TKA. The analysis from the two cohort studies showed an overall mean difference of −5.24 weeks (−6.84 to −3.64; supplementary figure 19).
Discussion
The present study, comparing unicompartmental and total knee arthroplasty, provides a synthesis of evidence from randomised controlled trials, national and nationwide registries, and cohort studies, including all outcome domains identified as important by patients. The study aimed to provide evidence to support informed shared decision making in the care of patients presenting with medial unicompartmental osteoarthritis of the knee.
Main findings
A large amount of research was used to address the aim of this study. With the selected search criteria, 60 studies presented data comparing UKA with TKA, and were included for analysis in the present study. Analysis of this data showed significant differences in outcomes between UKA and TKA, with advantages associated with UKA across multiple outcome domains. In domain 1, patients undergoing a UKA had significantly shorter operating times than those undergoing TKA in data from groups 2 and 3. Furthermore, patients undergoing UKA were shown to have significantly shorter hospital stays in all study groups analysed.
In domain 2, fewer early complications were seen in those patients undergoing UKA than in those undergoing TKA. Incidence of myocardial infarctions was only reported in a small number of studies. The only randomised controlled trial in group 1 and the registry and database data in group 2 studies showed a significantly higher risk of myocardial infarction after TKA than UKA, and group 3 studies showed equivocal results. Cerebrovascular events were reported in only two studies from group 2, which showed an increased risk of a patient having an event after TKA than after UKA (relative risk ratio 0.34 (95% confidence interval 0.15 to 0.74)). Fewer events of venous thromboembolism were reported after UKA than TKA, but the relative risk was only significantly different in the registry data (risk ratio 0.39 (0.27 to 0.57)). The risk of developing a deep infection was higher after TKA than after UKA at all levels where analysis was possible. The single randomised controlled trial reporting data on this outcome was not large enough to show any infections. However, analysis of study groups 2 and 3 showed a significant difference (relative risk ratio 0.59 (0.43 to 0.82) and 0.40 (0.16 to 1.01), respectively). It was not possible to calculate the risk ratio of mortality after UKA or TKA with studies in groups 1 or 3, because they were too small to capture this outcome. However, the larger database and registry studies in group 2 showed a significant increased risk of mortality after TKA than after UKA (risk ratio 0.27 (0.16 to 0.46), Z=5.02, P≤0.001).
In domain 3, group 1 studies did not show a significant difference in the range of movement. However, a significant improvement was seen in those patients receiving a UKA than in those receiving TKA in group 2 and 3 studies. In the limited analysis possible for postoperative kneeling ability, patients undergoing UKA had significantly better results (risk ratio 0.53 (95% confidence interval 0.28 to 1.01). PROM scores were reported to be significantly better after UKA than TKA in groups 1 and 3, but not significantly better in group 2 studies. For isolated pain scores, no significant difference was seen between UKA and TKA. However, UKA had better scores in functional PROMs scores, with significant results in the group 2 and 3 analyses.
In domain 4, reoperation rates were equivalent between UKA and TKA, with the only significant result in the group 3 analysis showing fewer reoperations after UKA when MUAs manipulations under anaesthetic were included. Revision rates were significantly better in all study groups for TKA versus UKA at five years. Only one randomised controlled trial in group 1 reported data up to 10 and 15 years, showing a non-significant reduction in revision rate after UKA. However, group 2 studies reporting data at 10 and 15 years showed consistently significantly better revision rates for TKA than for UKA.
For domain 5, only limited data were available for the rate of recovery. However, for return to work and return to sporting activities, a significantly quicker recovery was seen after UKA than after TKA (mean difference −0.96 (95% confidence interval −1.31 to −0.61), P<0.001, −5.24 (−6.84 to −3.64), P<0.001, respectively).
Comparison with other studies
We are not aware of any other study that has used our approach, but useful comparison can be made with previous systematic reviews, meta-analyses, and simple cohort studies. Arirachakaran and colleagues published a systematic review125 that included only randomised controlled trial data. This review reported similar results with significantly better function PROMs scores, range of movement after UKA, equivocal pain PROMs scores, and lower revision rates after TKA. Longo and colleagues,126 in reviewing the data available for UKA and TKA in the same patient, concluded that the only significant difference was an improved range of movement after UKA. More recently, Mohammad and colleagues28 did a meta-analysis on outcomes after the “Oxford” (Biomet) medial unicompartmental knee arthroplasty, showing a similar set of outcome advantages for this specific UKA device. Furthermore, Burn and colleagues27 investigated the economic implications of choosing between UKA and TKA. They found that despite a higher revision rate, patients receiving UKA had shorter hospital stays, quicker recovery periods, and reduced complication rates, and with an earlier return to work these patients have a reduced economic impact compared with those receiving TKA. This review shows very similar findings to our present study and to another analysis127 showing a quicker return to activities in younger patients.
The lower revision results for UKA than for TKA shown in our study are supported by other published literature.6 Annual reports from national registries have shown consistently higher revision rates for UKA than for TKA.5128 Further analysis of national joint registry data has allowed greater insight into the higher revision rate seen with UKA practice. The Nordic registries have reported a significantly higher implant survival of UKA at 10 years in centres that perform more than 11 UKA procedures per year,129 with the lowest revision rate seen in those centres performing more than 40 procedures a year.130 Robertsson and colleagues had reported a similar trend in the Swedish Knee Arthroplasty Register.131 Baker and colleagues132 showed increased revision rates in the UK National Joint Registry (NJR) for those surgeons performing fewer than 13 UKA procedures per year, and a greater propensity to revise UKA for unexplained pain.
Additionally, Liddle and colleagues8 showed that surgeons who report at least 20% of their arthroplasty practice as UKA achieve lower rates of revision, but that over 80% of surgeons performing UKA in the UK who enter data to the National Joint Registry performed fewer than 10 UKA procedures per year. Furthermore, single centre cohort studies, which used methods outside the scope of the present study, have shown that similar revision rates can be achieved for TKA and UKA.91112121 Hamilton and colleagues133 showed a reduced revision rate in those studies undertaken in high volume centres, although the strength of this evidence was weak. These results are considered to be related to the expertise and experience of the operating surgeons, producing better results, and their units having a higher threshold for revision surgery for unexplained pain and better postoperative support. Furthermore, more equivocal revision rates after UKA versus TKA (than those shown in the present study) have been reported in studies solely reporting outcomes on individual implants.134
Our methodology included insufficient studies to accurately analyse patients’ return to work or sporting activities after UKA and TKA. Published studies comparing all types of lower limb interventions, or UKA and TKA individually, were analysed by Witjes and colleagues,135 who found 36-89% and 75-100% of patients returned to sport after TKA and UKA, respectively, with a return to low impact sports at 12 weeks after UKA and 13 weeks after TKA.
Strengths and limitations
We have demonstrated the lack of good quality data from randomised controlled trials comparing outcomes of TKA with UKA, particularly pertaining to outcome measures important to patients such as returning to work and kneeling ability after the procedure. Ongoing studies such as TOPKAT119 will provide more high level evidence but have not been designed to investigate all of these outcome measures.
This study includes analysis of all levels of evidence, from level 1 trial data to level 4 cohort data, which has allowed a wide inclusion of studies and therefore a large number of individual cases. The inclusion of multiple study types does introduce significant heterogeneity (supplementary table 3), which would therefore affect the robustness of this study’s conclusions. However, the use of trial data, reports from national joint registries and national multicentre databases, and large cohort studies has allowed inclusion of as much data as possible, such as good quality research data from smaller studies, which can often be missed in systematic reviews. Despite our extensive search strategy, relevant studies for inclusion could have been missed, but on repeat searches using modified language, no new historical studies were identified. We decided to include studies from only the past 20 years to discount data from very early implant designs, and to remove some of the effect of the development of new implant designs and implanting techniques.
Our literary search confirmed the paucity of trial data in this field comparing TKA with UKA. The lack of level 1 data from randomised controlled trials does reduce the robustness of our conclusions, because there were only five trials comparing UKA with TKA, of which only four reported data on outcomes greater than one year, involving only 156 patients in total. Furthermore, despite the large number of studies reported, they varied in inclusion criteria, population demographics, end assessment points and methods, and varying degrees of statistical adjustment. The five year results from the TOPKAT study, the largest trial in this field, will offer an important contribution to the evidence base, and more high quality studies will be required.66
Inclusion of data from joint registry studies and large, multicentre, nationwide database studies might be considered controversial in such an analysis, because the data they present have many variables that are often not accounted for, such as detailed breakdown of multiple implant types, the grade of surgeon, surgical approaches, and centre experience. However, the value and feasibility of using these data has been highlighted,136 and meta-analysis of their outcomes has also been presented.137138139 One value of these studies is their size and statistical power, enabling differences in rare complications such as mortality rate.13 In addition, because implant survival and revision rates are likely to be affected by the experience of the operating surgeon and centre performing the procedure, registry data could be considered valuable “real world” data.
Another limitation of the study is that data from registry and large national multicentre database studies (group 2) tended to dominate the outcome domains they were included in, given the large patient numbers included in these studies. The effect of this limitation is uncertain, because these data have been recognised to include flaws owing to incomplete or inaccurate data collection.140141142143 Furthermore, data from studies in groups 2 and 3 were largely based on unmatched patient cohorts in relation to their preoperative disease severity or pattern, which could have resulted in a protopathic bias.
This study did not present data on all the outcome domains identified by the literature search. Aspects of UKA or TKA design were not explored in the current study, because further subdivision of the data could have diminished the validity of any conclusions drawn. Surgical approach was considered, but the studies identified were not comparative between UKA and TKA, and patients were often more concerned about the length of the scar, which is rarely reported. Blood loss or need for transfusion was discussed as a potential outcome domain but was thought to be a less important factor within the patient decision group. Lastly, cost effectiveness of UKA versus TKA featured highly in the literature search, and has been extensively studied in previous analyses.313233 Despite this factor being significant for healthcare providers, the present study was designed to aid patient decision making, and demonstrating cost implications could have unfairly influenced patients.
Despite its limitations, the study design followed appropriate methodology, and included many studies that reported data across multiple outcome domains on a substantial number of patients and implants. With this analysis, we aimed to provide the most complete representation possible of the differences in outcome between UKA and TKA.
Interpretation of available data
This study aimed to have immediate and practical relevance in helping to inform a patient centred, shared decision making process when deciding between UKA and TKA treatment for unicompartmental osteoarthritis. The need to choose between treatments could apply to 25-47% of patients presenting with primary osteoarthritis.2 This study showed some benefits for UKA over TKA in some outcome domains, including reduced length of stay in hospital, better functional outcome, and fewer medical complications. But in the longer term, the risk of revision was higher with UKA than TKA, although overall reoperation rate is lower. Our study highlights that a multidimensional approach to determining outcome is required when different treatment options are available for a single condition and there is no consensus on the best option.144
The most important beneficiaries of the outcome of our analyses are patients, who must decide which treatment option they wish to pursue. Their final decision will hinge on the relative value they place on the advantages and disadvantages of each treatment option. At present, many UK knee surgeons do not perform UKA, preferring to use TKA as their sole treatment option. As the case for UKA as a viable treatment option increases, more surgeons could offer UKA or refer to appropriate specialists. If such changes in patient and clinician preference occur, then the proportion of UK primary knee arthroplasties performed as UKA could increase from the present level of 8%.5
What is already known on this topic
Partial (or unicompartmental) and total knee replacement are both viable surgical options for treating unicompartmental knee osteoarthritis, but most patients with this condition currently undergo total knee replacement
Many patients are not offered partial knee replacement as part of the shared decision making process
The revision rate for total knee replacement is lower than for partial knee replacement in the longer term, but complication rates are lower after partial procedures in the shorter term
What this study adds
Partial knee replacement has several advantages over total knee replacement, including shorter time in hospital, fewer serious medical complications, lower mortality, lower deep infection rate, and better functional outcome
Revision surgery is less likely after total knee replacement, but reoperation for other causes occurs at the same rate for both procedures
This evidence should be used to inform shared decision making for patients
Footnotes
Contributors: HAW was responsible for the design of study, data collection, analysis, and writing of the paper. RM and SGFA were responsible for the abstract review, data extraction, and text editing. SS and AA facilitated patient discussion groups to establish outcomes of domain to be studied. WFJ and NB provided patients for discussion groups, and contributed to the review and text editing. SH gave statistical support for data analysis. AJP is the senior author and contributed to the development of study design and text editing. SH and AJP are the study guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: No separate funding was supplied for this study.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no direct support from for the submitted work, however, there was institutional funding from Arthritis Research UK and National Institute for Health Research Oxford Biomedical Research Centre; the researchers and funders were independent; AJP has received research grants from Zimmer-Biomet, and personal consultancy fees from Zimmer Biomet and Depuy; WFJ has received personal consultancy fees from Zimmer-Biomet; NB has received support from Zimmer-Biomet for educational consultancy and lectures.
Ethical approval: Ethical approval was not required for this analysis as all included data were already anonymised.
Data sharing: The full dataset and all technical appendices are available from the corresponding author. Consent was not obtained but the data presented are all anonymised and risk of identification is low.
The lead author affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.