Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: systematic review and meta-analysis
BMJ 2017; 359 doi: https://doi.org/10.1136/bmj.j4849 (Published 14 November 2017) Cite this as: BMJ 2017;359:j4849
- Chenhan Ma, foundation year 1 doctor1,
- Alison Avenell, professor1,
- Mark Bolland, associate professor2,
- Jemma Hudson, statistician1,
- Fiona Stewart, research fellow1,
- Clare Robertson, research fellow1,
- Pawana Sharma, research fellow1,
- Cynthia Fraser, information officer1,
- Graeme MacLennan, professor3
- 1Health Services Research Unit, University of Aberdeen, Health Sciences Building, Foresterhill, Aberdeen AB25 2ZD, Scotland, UK
- 2Bone and Joint Research Group, Department of Medicine, University of Auckland, Private Bag 92 019, Auckland 1142, New Zealand
- 3Centre for Healthcare Randomised Trials, University of Aberdeen, Health Sciences Building, Foresterhill, Aberdeen AB25 2ZD, Scotland, UK
- Correspondence to: A Avenell a.avenell{at}abdn.ac.uk
- Accepted 4 October 2017
Abstract
Objective To assess whether weight loss interventions for adults with obesity affect all cause, cardiovascular, and cancer mortality, cardiovascular disease, cancer, and body weight.
Design Systematic review and meta-analysis of randomised controlled trials (RCTs) using random effects, estimating risk ratios, and mean differences. Heterogeneity investigated using Cochran’s Q and I2 statistics. Quality of evidence assessed by GRADE criteria.
Data sources Medline, Embase, the Cochrane Central Register of Controlled Trials, and full texts in our trials’ registry for data not evident in databases. Authors were contacted for unpublished data.
Eligibility criteria for selecting studies RCTs of dietary interventions targeting weight loss, with or without exercise advice or programmes, for adults with obesity and follow-up ≥1 year.
Results 54 RCTs with 30 206 participants were identified. All but one trial evaluated low fat, weight reducing diets. For the primary outcome, high quality evidence showed that weight loss interventions decrease all cause mortality (34 trials, 685 events; risk ratio 0.82, 95% confidence interval 0.71 to 0.95), with six fewer deaths per 1000 participants (95% confidence interval two to 10). For other primary outcomes moderate quality evidence showed an effect on cardiovascular mortality (eight trials, 134 events; risk ratio 0.93, 95% confidence interval 0.67 to 1.31), and very low quality evidence showed an effect on cancer mortality (eight trials, 34 events; risk ratio 0.58, 95% confidence interval 0.30 to 1.11). Twenty four trials (15 176 participants) reported high quality evidence on participants developing new cardiovascular events (1043 events; risk ratio 0.93, 95% confidence interval 0.83 to 1.04). Nineteen trials (6330 participants) provided very low quality evidence on participants developing new cancers (103 events; risk ratio 0.92, 95% confidence interval 0.63 to 1.36).
Conclusions Weight reducing diets, usually low in fat and saturated fat, with or without exercise advice or programmes, may reduce premature all cause mortality in adults with obesity.
Systematic review registration PROSPERO CRD42016033217.
Introduction
Adults with obesity have an increased risk of premature mortality, cardiovascular disease, some cancers, type 2 diabetes, and many other diseases.12 These associations inform the need for programmes to prevent obesity, but, apart from prevention of type 2 diabetes,34 limited evidence from randomised controlled trials (RCTs) shows that weight loss interventions can prevent serious harm for people with obesity. Evidence from cohort studies has led to debate that deliberate weight loss for people who are overweight or obese, with body mass index (BMI) ≤35 kg/m2, might actually be harmful.5 Studies show that older people,6 and those with cardiovascular disease7 who are less markedly obese, might experience adverse consequences from deliberate weight loss. Recent analyses by the Global BMI Mortality Collaboration, however, tried to limit confounding and corrected for reverse causality, finding that the risk of premature mortality was lowest at BMIs of 20-25.8
Association studies cannot tell us if deliberate weight loss in adults with obesity can reduce their risk of premature mortality, cardiovascular disease, or cancer. Only one systematic review and meta-analysis of RCTs of intentional weight loss in adults with obesity has examined this question.9 That review included 15 trials, reporting a 15% relative reduction in premature mortality (risk ratio 0.85, 95% confidence interval 0.73 to 1.00), but did not evaluate causes of death or cardiovascular and cancer outcomes.9 We knew of many other weight loss RCTs with mortality data, as well as cancer and cardiovascular outcomes, from our database of long term RCTs of weight loss interventions for adult obesity, which was developed for health technology assessments1011 and is continually updated. We systematically reviewed long term (≥1 year) RCTs of weight loss interventions for adults with obesity to examine the effects of any type of weight loss diet on all cause, cardiovascular, and cancer mortality, cardiovascular disease, cancer, and body weight.
Methods
We adhered to the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines for systematic reviews of interventions.12 We used a prespecified protocol, registered with PROSPERO (CRD42016033217).13
Search strategy and selection criteria
We included RCTs with adults (mean or median age ≥18 years) and a minimum follow-up of one year. Participants had a mean BMI ≥30 at baseline. Included trials had to be focused clearly on weight loss with a weight reducing diet, with or without advice for increasing physical activity and/or provision of a physical activity programme to attend, compared with a control intervention. We didn’t include trials in pregnant or postpartum women.
We sought summary data for three primary outcomes: all cause mortality, cardiovascular mortality, and cancer mortality. Secondary outcomes were participants with a new cardiovascular event, participants with a new cancer, and weight change. In our main analysis we used cardiovascular mortality and events as defined by the investigators but did not include the development of hypertension. We undertook post hoc analyses of cardiovascular mortality and cardiovascular events as defined in the American College of Cardiology/American Heart Association (ACC/AHA) guidelines.14
We identified RCTs by searching the full texts of trial reports in our database of all long term (≥1 year) RCTs of weight loss interventions for adults with obesity used in our previous systematic reviews and health technology assessments. Our database is derived from previous search strategies compiled from Medline, Embase, and the Cochrane Central Register of Controlled Trials, from 1966 to December 2015.1011 We performed an updated search from August 2015 to December 2016. We didn’t apply any language exclusions. In 2016-17 we contacted the authors of 48 RCTs to clarify data or request unpublished outcome data, where trial reports implied that relevant data might be available; for example, when the trial reported hospital admissions or adverse events without giving further details.
Data analysis
AA and CM independently confirmed study eligibility. CM, FS, CR, and PS extracted data, which were then checked by a second author (AA, CM). Cancer outcome and cardiovascular outcome data (including coding outcomes defined by the ACC/AHA guideline14) were further adjudicated by MB, with differences resolved by Andrew Grey (associate professor in the Department of Medicine, University of Auckland). Two authors (AA, CM, FS, CR, PS) independently assessed quality using the Cochrane risk of bias tool.15 All differences were resolved by discussion.
We used random effects meta-analysis to analyse pooled outcome data. For binary outcomes, we estimated risk ratios and 95% confidence intervals, using all participants randomised for the denominators. We estimated weighted mean differences and 95% confidence intervals for continuous outcomes, giving preference to intention to treat data and data taking account of dropouts (preferentially baseline observation carried forward) if these were provided. We included outcome data from two cluster RCTs1617 using the correction method described in the Cochrane Handbook18 and the intraclass correlation coefficients reported in the original trial publications. We assessed heterogeneity between studies using Cochran’s Q statistic and the I2 test. We originally planned meta-regression to investigate heterogeneity in disease outcomes, but I2 tests for disease outcomes were 0%, so it was not appropriate. We carried out a sensitivity analysis with a random effects bayesian logistic regression model (with non-informative priors) using WinBUGS 1.4.319 because some trials reported few events, which may cause sparse data bias. We performed all other analyses using Stata Release 1420 and used funnel plots to examine small study bias.
For all outcomes we performed prespecified subgroup analyses for sex, age (<60 v ≥60), BMI (<40 v ≥40, later changed to <35 v ≥35 as we found no trial with BMI ≥40), glycaemic control (normal v impaired glucose tolerance or impaired fasting glucose v type 2 diabetes), ethnicity (defined if ≥80% of participants belonged to an ethnic group, otherwise defined as mixed), physical activity interventions (none v advice only v exercise programme provided).
In post hoc additional analyses we added trials in any Asian population group if the mean BMI was ≥25, as diseases associated with obesity are known to occur at lower BMI in Asian populations than other ethnic groups.21 No single BMI cut-off has been agreed to define obesity in Asian populations. Although the World Health Organization recommends 27.5 as a BMI threshold for a high risk of comorbidities,21 it also suggests that Asian countries develop their own specific BMI cut-offs for obesity. India and Japan have set ≥25 as the threshold for obesity,2223 and in China the risk of comorbidities has been found to increase for BMI over 28.24
For all outcomes we performed two prespecified sensitivity analyses for allocation concealment (low risk of bias vs other risk of bias) and follow-up (<80% vs ≥80%).
We used GRADE (grading of recommendations, assessment, development, and evaluations) to judge the quality of the evidence for mortality, cardiovascular, and cancer outcomes.25
Role of the funding source
The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing this report. CM and AA had full access to all study data and had final responsibility for the decision to submit for publication.
Patient involvement
No patients or members of the public were involved in the development of research questions, the design of the study, or the development of outcome measures. No patients were asked to advise on interpretation or writing up of results. There are plans to disseminate the results of the research to the relevant patient community.
Results
Trial characteristics
We screened 1174 full text trial reports and 5982 titles and abstracts (fig 1⇓) and identified 54 RCTs for inclusion3416172627282930313233343536373839404142434445464748495051525354555657585960616263646566676869707172737475767778798081828384858687888990919293949596 in the final review.

{kind=link}
Table 1⇓ provides details of the included studies, involving 30 206 adults with obesity. Nine trials (16.7%) included women only,264445505152778894 and two (3.7%) men only.5872 Twelve trials (22.2%) recruited participants with no reported existing medical conditions or no reported increased risk of developing comorbidities related to obesity. Other trials recruited participants with increased risk of type 2 diabetes or hypertension or included participants that already had at least one of the following conditions: hypertension, type 2 diabetes, hyperlipidaemia, breast cancer, colorectal adenoma, psychiatric illnesses, cognitive impairment, osteoarthritis of the knee, coronary heart disease, or urinary incontinence.
Characteristics of randomised controlled trials
Five trials (9.3%) were undertaken in Asian populations,1617597580 but only one with BMI ≥30,216 one trial (1.9%) was in a population of black people in the USA,50 31 (57.4%) in populations of white people, and 17 (31.5%) in mixed population groups. Thirty one (57.4%) trials took place in North America, 16 (29.6%) in Europe, two (3.7%) in Australia, and one (1.9%) in Brazil. The four trials in Asian populations outside the UK had mean BMIs between 25 and 30. 17597580 Thirty six (66.7%) trials had participants with a mean or median BMI <35, and 14 (25.9%) had BMIs ≥35 (table 1⇑).
Most trials recruited predominantly middle aged adults. Fourteen (25.9%) had a mean or median age at baseline of 60 years or more, none had a mean or median age of under 40 years. Thirty one (57.4%) trials followed participants for two years or longer, and seven (13.0%) trials (9,937 participants) followed participants for five years or longer. In 39 trials (72.2%) the drop-out rate was <20% at trial completion.
Detailed descriptions of the weight loss diets were not always clearly provided in the trials. All but one of the trials described at least one of their interventions as being a low fat weight reduction diet (usually ≤30% of energy as fat, although this was not always specified) or had sufficient information to establish that a reduction in fat intake was prescribed. Most trials also described the prescription of a reduction in saturated fat. One trial described using a balanced Mediterranean diet.79 One trial included the option to undertake a diet with ≤50 g/day of carbohydrate.96 Two weight loss trials specifically described diets to reduce low glycaemic index as part of their intervention,2630 whereas other trials generally described diets that would be compatible with lowering glycaemic indices by increasing intake of complex carbohydrates and dietary fibre. Four trials (7.4%) were based on the DASH (dietary approaches to stop hypertension) diet.31394054 Eight (14.8%) trials based their diets on those of the US Diabetes Prevention Program,426526067749394 and four trials (7.4%) described basing their content in part on different editions of the Dietary Guidelines for Americans.64697276
Only three trials (5.6%) did not report providing exercise advice or an exercise programme.455568 Twenty two trials (40.7%) provided an exercise programme for participants to attend, and 29 trials (53.7%) described providing advice to increase exercise only, without an exercise programme.
Supplementary figure 1 provides our risk of bias assessments for individual studies. Only 15 trials (27.8%) reported methods of randomisation and allocation concealment judged to be at low risk of bias. Blinding of participants and study personnel was rarely possible, but we judged that lack of blinding of outcome assessment would rarely have been a source of bias except for weight outcomes. Only 10 (18.5%) trials were judged to be at low risk for attrition bias, and 12 (22.2%) at low risk for reporting bias. Seven (13.0%) trials were judged to be at high risk of bias as a result of premature trial termination,526575 change in the primary outcome,16 influence of a drug placebo in the control group,4 or trial investigators reporting that they were sponsored by grants from a commercial weight loss programme71 or that they were co-owners of a company developing products related to the research.72
Meta-analyses
Details of our adjudication processes for cardiovascular and cancer outcomes are provided in supplementary tables 1-3. Supplementary table 1 compares all cause mortality, cardiovascular mortality, and cancer mortality across all trials, showing that we were not always able to obtain causes of death from authors.
Based on the GRADE approach for judging quality of the evidence (supplementary table 4) we found high quality evidence from 34 trials (21 699 participants) providing data on all cause mortality (fig 2⇓), which showed a decrease in premature mortality with weight loss interventions (n=34 trials, 685 events; risk ratio 0.82, 95% confidence interval 0.71 to 0.95; I2=0%). The Look AHEAD trial had 54.6% of the weighting in the meta-analysis.6566 Without this trial weight loss interventions were still associated with decreased all cause mortality (n=33 trials, 309 events; risk ratio 0.78, 95% confidence interval 0.63 to 0.96; I2=0%). The funnel plot showed no evidence of small study bias (Egger’s test P=0.269, supplementary figure 2).

Fig 2 Random effects meta-analysis of the effects of weight loss interventions on all cause mortality. ADAPT=arthritis, diet, and activity promotion trial; CLIP=community level interventions for pre-eclampsia; DPP=diabetes prevention program; DPS=diabetes prevention study; FFIT=football fans in training; Look AHEAD=look action for health in diabetes; PRIDE=program to reduce incontinence by diet and exercise; TAIM=trial of antihypertensive interventions and management; TOHP=trials of hypertension prevention; TONE=trial of nonpharmacologic intervention in the elderly.
{kind=link}
Fewer trials reported data for cardiovascular mortality and cancer mortality, resulting in considerable uncertainty in the estimates of effects of weight loss interventions on these outcomes. We found moderate quality evidence for an effect on cardiovascular mortality (n=8 trials, 134 events; risk ratio 0.93, 95% confidence interval 0.67 to 1.31; I2=0%) and very low quality evidence for an effect on cancer mortality (n=8 trials, 34 events; risk ratio 0.58, 95% confidence interval 0.30 to 1.11; I2=0%) (figs 3 and 4⇓). Limiting cardiovascular mortality to ACC/AHA defined events did not influence this result, as the data were identical (n=8 trials, 134 events; risk ratio 0.93, 95% confidence interval 0.67 to 1.31; I2=0%).

Fig 3 Random effects meta-analysis of the effects of weight loss interventions on cardiovascular mortality. DPP=diabetes prevention program; DPS=diabetes prevention study.
{kind=link}
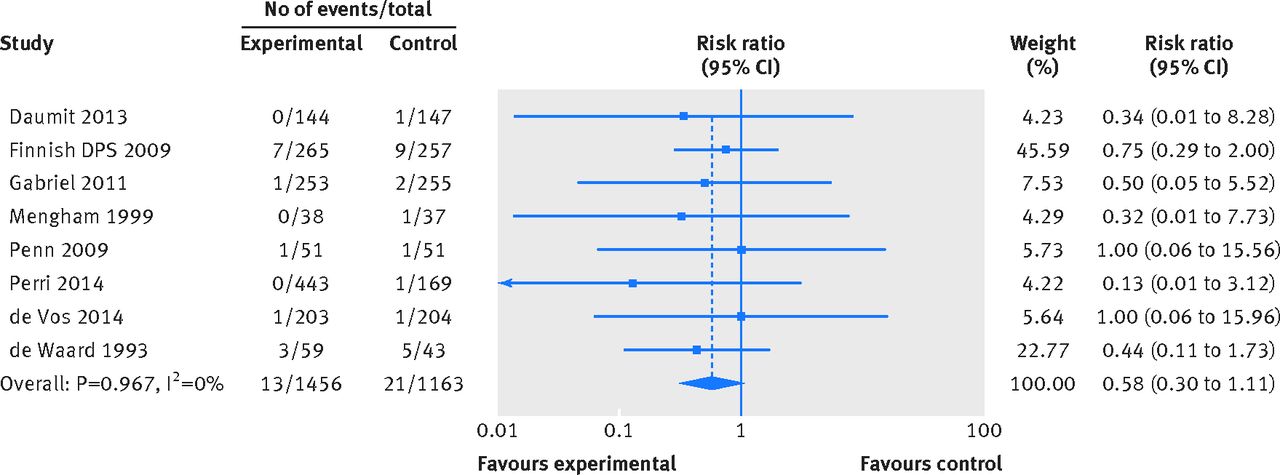
Fig 4 Random effects meta-analysis of the effects of weight loss interventions on cancer mortality. DPS=diabetes prevention study.
{kind=link}
Twenty four trials (15 176 participants) reported high quality evidence on participants developing new cardiovascular events (n=24, 1043 events; risk ratio 0.93, 95% confidence interval 0.83 to 1.04; I2=0%). Using events classified according to ACC/AHA definitions, results were very similar (fig 5⇓, supplementary figure 3). Nineteen trials (6330 participants) provided very low quality evidence on participants developing new cancers (n=19, 103 events; risk ratio 0.92, 95% confidence interval 0.63 to 1.36; I2=0%) (fig 6⇓). Bayesian meta-analyses for all of the above outcomes provided similar results (supplementary table 5).

Fig 5 Random effects meta-analysis of the effects of weight loss interventions on participants with a cardiovascular event. CLIP=community level interventions for pre-eclampsia; DPP=diabetes prevention program; FFIT=football fans in training.
{kind=link}

Fig 6 Random effects meta-analysis of the effects of weight loss interventions on participants developing cancer. DPS=diabetes prevention study.
{kind=link}
Interventions had a beneficial effect on weight change after one year (n=44, mean difference −3.42 kg; 95% confidence interval −4.09 to −2.75 kg; I2=92%), after two years (n=20, mean difference −2.51 kg; 95% confidence interval −3.42 to −1.60 kg; I2=89%) and after three or more years (n=8, mean difference −2.56 kg; 95% confidence interval −3.50 to −1.62 kg; I2=87%) (supplementary figures 4 to 6). Heterogeneity for each of these meta-analyses was very high (I2=87% to 92%), reflecting the wide diversity of weight loss interventions and their effects on weight.
Sensitivity analyses
Sensitivity analyses for allocation concealment (low risk of bias versus other risk of bias) and completion of follow-up (<80% v ≥80% of participants completed) did not show any statistically significant heterogeneity for mortality, cardiovascular outcomes, or cancer outcomes (supplementary table 6).
Weight change at final follow-up was lower in trials with low risk of bias for allocation concealment (n=17, mean difference −2.33 kg; 95% confidence interval −2.87 to −1.79 kg) than for trials with high or unclear risk of bias for allocation concealment (n=31, mean difference −3.24 kg; 95% confidence interval −4.00 to −2.49 kg).
Weight change at final follow-up was lower in trials with completed follow-up of less than 80% (n=15, MD −2.09 kg; 95% CI: −2.80 to −1.37 kg) than for trials with follow-up of 80% or more (n=33, MD −3.13 kg; 95% CI: −3.71 to −2.55 kg).
Subgroup analyses
We undertook many subgroup analyses, including post hoc analyses with the addition of trials in Asian populations with BMI ≥25 (supplementary table 6, supplementary figures 7-9). Tests for subgroup differences for mortality, cardiovascular outcomes, and cancer outcomes provided weak evidence that participants without type 2 diabetes might be at lower risk of a new cardiovascular event than participants with type 2 diabetes or those with impaired glucose tolerance or impaired fasting glycaemia. Similarly, we found weak evidence that groups of white participants may be at lower risk of a new cardiovascular event than black, mixed, or Asian population groups when following weight loss interventions.
Subgroup analyses for weight change at final follow-up provided weak evidence that participants aged 60 or over lost more weight than younger participants and that participants in trials in Asian populations lost less weight than those in trials with other population groups. Similarly, we found weak evidence of better long term weight loss with trials that provided a physical activity programme, compared with trials that gave only physical activity advice or did not report providing physical activity advice.
Discussion
We found high quality evidence that weight reducing diets for adults with obesity, usually low in fat and low in saturated fat, were associated with a 18% relative reduction in premature mortality over a median trial duration of two years, corresponding to six fewer deaths per 1000 participants (95% confidence interval two to 10). This evidence provides a further reason for weight reducing diets to be offered alongside their already proven benefits, such as type 2 diabetes prevention. We were unable to show effects on cardiovascular and cancer mortality, or participants developing cardiovascular events or new cancers, although fewer trials reported events for these outcomes, resulting in much uncertainty around their effect estimates.
We identified 34 trials reporting mortality data compared with 15 in the previous systematic review by Kritchevsky and colleagues,9 which included weight loss interventions irrespective of baseline BMI, and we made very considerable efforts to clarify data and retrieve unpublished data from 48 trialists. We used a comprehensive search strategy with full text searching of trials in our obesity database. The trials we included were not necessarily designed to collect data on mortality, cardiovascular, and cancer outcomes, although larger trials generally were.656681828384858687 We might have failed to identify all trials with outcome data, if trialists did not present these outcomes or presented them as unspecified adverse events. This may have biased results, although we could not see obvious funnel plot asymmetry for all cause mortality. Trials generally excluded participants with a recent diagnosis of cancer, but this was not always clear, so some participants may have had a recurrence of cancer, rather than a new event. Many of the trials had quite intensive control group interventions, and the unblinded nature of the interventions could have led to more medical treatment in control groups, tending to reduce differences between groups.65 Using GRADE to assess the quality of the evidence aids interpretation of the limitations of the evidence. We undertook sensitivity and subgroup analyses, including post hoc analyses, which should be regarded with caution. Individual patient data meta-analyses are required for further exploration of these subgroup findings.
In systematic reviews of controlled cohort studies, bariatric surgery has been associated with significant reductions in mortality, cardiovascular events, myocardial infarction, stroke, and risk of cancer.9798 A systematic review and meta-analysis of population prospective cohort studies by Flegal and colleagues found that BMIs of 30 to <35 were not associated with higher mortality, compared with BMIs of 18.5 to <25.5 By contrast, the Global BMI Mortality Collaboration found that obesity (BMI 30 to <35) was associated with higher mortality; the investigators reduced reverse causality by examining data in non-smokers and excluding the first five years of follow-up.8 Their findings were consistent for men and women, up to 89 years, and in the four continents examined. Similar findings were seen for deaths due to coronary heart disease, stroke, cancer, and respiratory disease. Our findings for BMI from RCT evidence are consistent with data from the Global BMI Mortality Collaboration.8 Epidemiological studies can demonstrate the risks of higher BMIs and, therefore, the necessity for preventing obesity, but epidemiological associations between changes in body weight and changes in disease and mortality are often limited by the lack of information on the intentionality of that weight loss. Furthermore, treatment effects found in RCTs might differ from those expected in epidemiological studies, whereby epidemiological studies might overestimate benefits.99
Evidence from systematic reviews indicates that physical activity as an adjunct to weight reducing diets might be more effective than diets alone, in terms of weight loss and improvements in blood lipids and blood pressure.100 We were unable to show differences for mortality, cardiovascular disease, and cancer between weight reducing diets alone, diets plus advice on exercise, and diets plus an exercise programme for people to attend, for which we had limited statistical power. The majority of RCTs of weight loss interventions for obesity in adults have used low fat, weight reducing diets. But a recent systematic review by Tobias and colleagues101 found that low carbohydrate weight reducing diets were more effective for weight loss than low fat, weight reducing diets, but found no difference between low fat, weight reducing diets (defined as <30% fat) and higher fat, weight reducing diets on weight loss. Recent US guidelines102 have been criticised for the lack of evidence from RCTs to support guidance.103 Thus, we must consider whether the type of weight loss diet, particularly low fat, weight reducing diets, usually with <10% of energy as saturated fat, affects important health outcomes beyond cardiovascular risk factors or weight.100 That all except one of the interventions included here used a low fat, weight reducing diet provides important evidence on all cause mortality for weight reduction with this type of diet. We do not have the evidence to establish whether other forms of weight reducing diets have this effect, and we cannot dissociate the effects of weight loss from the use of low fat diets in our results.
We encourage investigators studying weight reducing diets to adhere to CONSORT guidance on reporting harms by always reporting clinically important outcomes and adverse events, irrespective of whether they think these events are related to the interventions.104 Collecting and reporting major disease outcomes in weight reducing trials for obesity is important, particularly cardiovascular disease and cancer. We did not have sufficient data to examine whether other types of diet or physical activity influence outcomes or whether certain groups in the population are more or less likely to benefit.
In conclusion, weight reducing diets, usually low in fat and low in saturated fat, with or without an exercise component, may reduce premature all cause mortality in adults who are obese. By implication, our data support public health measures to prevent weight gain and facilitate weight loss using these types of diet.
What is already known on this subject
Whether recommendations to follow weight reducing diets can reduce premature mortality, cardiovascular disease, and cancer for adults who are obese is unclear
What this study adds
Weight reducing diets, usually low in fat and saturated fat, with or without exercise advice or programmes, may reduce premature all cause mortality in adults who are obese
Our data provide supporting evidence for public health measures to prevent weight gain and facilitate weight loss using diets low in fat and saturated fat
Footnotes
We thank Andrew Grey for helping to resolve discrepancies in data extraction and interpretation for cardiovascular events and cancer events. We thank trialists from 16 studies for clarifying or providing additional information for this review (Andrews 2011, Aveyard 2016, Bennett 2012, de Vos 2014, Finnish Diabetes Prevention Study 2009, Goodwin 2014, Green 2015, Horie 2016, Hunt (FFIT) 2014, Katula 2013, Li (Da Qing) 2014, Logue 2005, Ma 2013, O’Neil 2016, Rejeski (CLIP) 2011, Uusitupa 1993) and others who provided information, but their trials were later found not to fulfil our inclusion criteria.
Contributors and sources: AA, CM, MJB, CF, and GM designed this study. CM, AA, and CF searched the literature. CM, AA, FS, CR, PS, and MJB extracted data. CM, AA, JH, MJB, and GM analysed data. CM and AA wrote the first draft of the manuscript. All authors contributed to revisions of the manuscript. AA is the guarantor.
Funding: The Health Services Research Unit is funded by the Chief Scientist Office of the Scottish Government Health and Social Care Directorate.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: The Health Services Research Unit is funded by the Chief Scientist Office of the Scottish Government Health and Social Care Directorate. No author has financial relationships with any organisations that might have an interest in the submitted work in the previous three years.
Data sharing: All data are included in the paper or supplementary appendix. No additional data are available.
Transparency: AA and CM affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.