Management and prevention of exacerbations of COPD
BMJ 2014; 349 doi: https://doi.org/10.1136/bmj.g5237 (Published 22 September 2014) Cite this as: BMJ 2014;349:g5237
- Shawn D Aaron, professor, University of Ottawa
- Correspondence to: S D Aaron saaron{at}ohri.ca
Abstract
Patients with chronic obstructive pulmonary disease (COPD) are prone to acute respiratory exacerbations, which can develop suddenly or subacutely over the course of several days. Exacerbations have a detrimental effect on patients’ health status and increase the burden on the healthcare system. Initial treatment is unsuccessful in 24-27% of patients, who have a relapse or a second exacerbation within 30 days of the initial event. No obvious benefit has been seen in recent clinical trials of anti-tumour necrosis factor therapy, anti-leukotriene therapy, intensive chest physiotherapy, or early inpatient pulmonary rehabilitation for treatment of exacerbations. By contrast, clinical trials of prevention rather than acute treatment have shown promising results. Long acting β agonist (LABA) or long acting anti-muscarinic (LAMA) bronchodilators and inhaled corticosteroid-LABA combinations prevent exacerbations in patients at risk, with relative risk reductions averaging 14-27% for each of these drugs relative to placebo. Triple therapy with inhaled corticosteroid-LABA plus LAMA may provide additional benefit, although study results to date are heterogeneous and more studies are needed. Pneumonia is an important complication of treatment with inhaled corticosteroid-LABA products, and the risk of pneumonia seems to be doubled in patients with COPD who use fluticasone. The addition of azithromycin to usual COPD therapy prevents exacerbations, although it may prolong the Q-T interval and increase the risk of death from cardiovascular disease in patients prone to arrhythmia. New potential drugs—including mitogen activated protein kinase inhibitors, phosphodiesterase 3 inhibitors, and monoclonal antibodies to the interleukin 1 receptor—offer additional hope for treatments that may prevent exacerbations in the future.
Introduction
Acute exacerbations of chronic obstructive pulmonary disease (COPD) are characterized clinically by worsening dyspnea, cough, sputum production, and airflow obstruction.1 Such exacerbations are associated with short term and long term reductions in quality of life and lung function, as well as increased risk of death.2 3 Owing to the considerable impact of these exacerbations on patients’ health status, their frequency is now recognized as a key component of the characterization of patients with COPD, and the prevention and treatment of exacerbations has become a primary goal of treatment.4
This article aims to review recent evidence, mostly from randomized controlled trials (RCTs), on new drug and non-drug based therapies for the prevention and treatment of COPD exacerbations. Research in this area—both industry driven and academic—has increased greatly over the past decade, and new studies and drugs are rapidly emerging. Results of recent clinical trials suggest that substantial gains have been made in developing new strategies to prevent such exacerbations. However, studies evaluating new therapies for the acute treatment of COPD exacerbations have not been so successful.
Sources and selection criteria
We searched the Cochrane Airways Group register of clinical trials and Medline from 1990 to October 2013 and November 2013, respectively. Search terms included: chronic obstructive pulmonary disease (COPD), or chronic bronchitis, or emphysema, or exacerbations of COPD, and therapy or prevention. Controlled clinical trials and systematic reviews with meta-analyses of interventions or drugs to prevent or treat acute exacerbations of chronic obstructive pulmonary disease were selected for potential inclusion in this article. We excluded observational studies and non-randomized trials.
Definition of an exacerbation of COPD
Exacerbations of COPD are characterized by a sustained worsening of respiratory symptoms from the usual stable state beyond normal day to day variations.5 Typical symptoms associated with exacerbations include worsening of dyspnea and cough, as well as increased sputum volume and sputum purulence.1 Exacerbations range in severity from transient reductions in functional status to fatal events.
Definitions of exacerbations vary between clinical studies. Studies that use home based symptom diaries or other symptom monitoring tools—such as the COPD assessment test or the exacerbations of chronic pulmonary disease tool scales—may use symptom based definitions that rely on a sustained worsening of respiratory symptoms for two consecutive days.6 7 Studies in COPD cohorts suggest that many of these symptom based events may go unreported and untreated.8 9 Most clinical trials that evaluate drugs to prevent exacerbations use event based definitions of exacerbation, which require an increase in both symptoms and the use of healthcare resources.10 11 12 Recent pivotal clinical trials define moderate exacerbations as those that require treatment with systemic glucocorticoids or antibiotics (or both) and severe exacerbations as those that require hospital admission.13 14 15
To investigate whether the use of different definitions of COPD exacerbations affected the results of clinical trials, the INSPIRE study compared the incidence of exacerbations using both symptom based definitions and treatment based ones.16 In this long term study, three COPD exacerbations were detected per patient year when a symptom based definition was used compared with about 1.5 exacerbations per patient year when a treatment based definition was used. Thus about 50% of symptom defined COPD exacerbations are not treated by physicians, and these exacerbations are unlikely to be counted as exacerbation events in most clinical trials.
Causes of COPD exacerbations
COPD exacerbations are caused by complex interactions between the host, respiratory viruses, and airway bacteria, which lead to an increase in the inflammatory burden within the airway.17 Studies suggest that airway neutrophils, as well as systemic and local mediators of inflammation, such as interleukin 8 and tumor necrosis factor α (TNF-α) increase during COPD exacerbations compared with the stable state.18 Migration and activation of neutrophils within the airway leads to the release of proteases and reactive oxygen species; this further damages the airway epithelium and leads to worsening of airway inflammation and airflow limitation (fig 1⇓). A minority of exacerbations are associated with airway and sputum eosinophilia.19

Fig 1 Mechanism for acute exacerbations in chronic obstructive pulmonary disease (COPD). Triggers of COPD exacerbations include infectious agents such as bacteria and viruses and non-infectious agents such as air pollution. These stimuli activate airway epithelial cells and macrophages to release inflammatory cytokines including tumor necrosis factor α (TNF-α), interleukin 6 (IL-6), and IL-8. These cytokines lead to neutrophil recruitment and the release of reactive oxidant species and proteases from activated neutrophils, which magnify the inflammatory process20
{kind=link}
COPD exacerbations are accompanied by changes in airway physiology that induce dyspnea.21 A clinical study suggested that patients experience acute worsening of airflow obstruction accompanied by acute lung hyperinflation at the time of a moderate exacerbations.22 At recovery, 60 days after the onset of the exacerbation, inspiratory capacity and forced expiratory volume in one second (FEV1) increased by 18% compared with values during the exacerbation, and air trapping (residual volume) decreased by 11%. Improvements in dyspnea after acute exacerbations significantly correlated with a reduction in lung hyperinflation and consequent increase in expiratory flow rates. This suggests that dyspnea during an acute exacerbation is probably partially mediated by the dynamic hyperinflation that occurs in response to the airflow limitation associated with these events (fig 2⇓).22
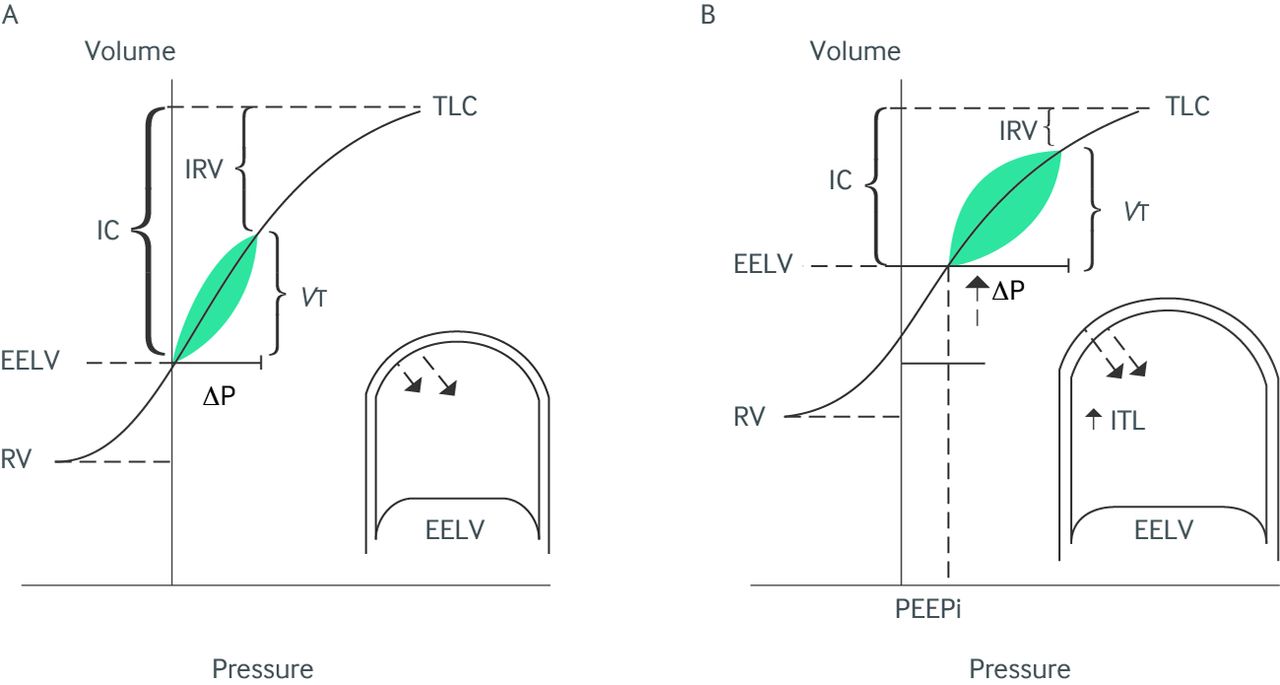
Fig 2 Schematic diagram of the pathophysiologic effects of an exacerbation of chronic obstructive pulmonary disease (COPD). Pressure-volume plots are shown during (A) stable COPD and (B) an exacerbation. During exacerbation, worsening airflow obstruction leads to dynamic hyperinflation, with increased end expiratory lung volume (EELV) and air trapping manifested as an increased residual volume (RV). Corresponding reductions occur in inspiratory capacity (IC) and inspiratory reserve volume (IRV). As a result, tidal breathing is shifted to the right on the pressure-volume curve, closer to total lung capacity (TLC), resulting in unfavorable overall compliance of the respiratory system. Increased mechanical pressures must be generated by the respiratory muscles to maintain tidal volume (VT). At EELV during an exacerbation, intrapulmonary pressures do not return to zero, as a result of the development of intrinsic positive end expiratory pressure (PEEPi), which imposes further increased inspiratory threshold loading (ITL) on the inspiratory muscles (inset). ΔP=change in pleural pressure. Reproduced, with permission, from Bafadhel and colleagues19
{kind=link}
In general, viral and bacterial infections are the most important triggers of exacerbation.23 24 25 Studies suggest that exacerbations are often associated with the isolation of new strains of airway bacteria, with an accompanying host inflammatory response to these new strains.23 26 Respiratory bacteria and viruses often act in combination.27 Recent studies of experimentally induced rhinovirus infection in patients with COPD suggest that bacterial infection of the airways often follows acute rhinovirus infection, and that infection with both viruses and bacteria can exert a synergistic inflammatory effect.28
Coinfection with viruses and bacteria has been detected in 25% of exacerbations and is associated with more severe functional impairment and longer hospital stays.29 Molecular techniques, including multiplex polymerase chain reaction, provide greater sensitivity to detect acute viral respiratory tract infections that cause exacerbations. However, a specific infectious or environmental cause cannot be identified in about a third of severe exacerbations.30
Recent investigations using cluster analysis suggest that exacerbations can be grouped into four categories: bacterial, viral, predominantly eosinophilic, and a “pauci-inflammatory” category associated with limited changes in the inflammatory profile.19 Each of these clusters is associated with a biomarker, suggesting that biomarkers may become useful for categorizing the cause of an exacerbation.
Natural course of exacerbations: onset and recovery
A recent prospective cohort of 212 patients with COPD was monitored using daily symptom diaries for a median of 2.8 years to characterize the time course of the onset of COPD exacerbations.31 Patients recorded 4439 episodes of worsening respiratory symptoms from baseline; 55% of these events resolved spontaneously and 45% resulted in an exacerbation. In 56% of COPD exacerbations the onset was sudden and the exacerbation threshold was crossed on the same day that respiratory symptoms began. By contrast, in 44% of exacerbations the onset of symptoms was gradual (median duration from symptom onset to exacerbation: four days; fig 3⇓). Patients with sudden onset exacerbations had more intense symptoms but a shorter median recovery time back to baseline health status (11 v 13 days; P<0.001). The study concluded that COPD exacerbations exhibit two distinct patterns—sudden and gradual onset—and that sudden exacerbations are associated with increased peak respiratory symptoms but shorter exacerbation recovery times.31

Fig 3 Time course and calculation of the onset and duration of exacerbation intervals: a sudden onset exacerbation is shown on the left, a gradual onset exacerbation on the right. The opening event (O) was defined as the first day of worsening of respiratory symptoms above usual baseline values. An exacerbation (E) was defined as the first of two or more consecutive days during which the patient recorded two or more new or worsening symptoms, at least one of which was a major symptom (a daily symptom score of ≥6 points for two consecutive days (indicated by the dotted line)). A closing (C) was defined as the first of five consecutive days during which symptoms had returned to their usual baseline levels. For sudden onset exacerbations the OE interval is 0 days, indicating that the exacerbation occurs on the first day of worsening of respiratory symptoms. About 55% of exacerbations are sudden onset. The EC represents the duration of the exacerbation—the time from the onset of the exacerbation to recovery back to baseline. Reproduced, with permission, from Papi and colleagues29
{kind=link}
Previous data have suggested that the median duration of recovery time after an acute exacerbation is 7-10 days for lung function as measured by peak expiratory flow, although there is wide variation, and a minority (<10%) of patients never recover to their pre-exacerbation lung function.32 Symptoms may take longer to recover than peak expiratory flow, and the median duration of symptom recovery back to previous baseline is 11-13 days.31 33
About a quarter of inpatients treated for an acute COPD exacerbation do not respond to initial treatment and experience an adverse outcome, defined as either death, intubation, or need for readmission or intensification of drug therapy. Similarly, studies suggest that a quarter of outpatients treated for an acute exacerbation either relapse (defined as an unscheduled visit to a physician or the emergency department because of worsening dyspnea) or have a second exacerbation within 30 days of the initial presentation.33 Many of these patients require readmission to hospital.33
In 2010 in the United States, there were 606 000 hospital admissions for COPD and 126 000 patients (21%) required readmission within 30 days.33 Clinical trials indicate that about 27% of outpatients treated with combined antibiotic and corticosteroid therapy relapse within 30 days.34 Treatment failure rates in inpatients with an exacerbation average 24% at 30 days and rise to 36-37% by 90 days.35 36 A recent systematic review found that there was not enough evidence to recommend specific interventions to reduce the risk of readmission in patients who have been treated in hospital for an acute exacerbation.37
COPD exacerbations and mortality
A prospective five year cohort study of 304 Spanish men with COPD found that the frequency of exacerbations is independently associated with mortality.38 When a service based definition of COPD exacerbation (need for emergency department treatment) was used, patients with three or more exacerbations had a survival rate of 30% at five years, whereas those without an exacerbation had a survival rate of 80% (hazard ratio 4.13, 95% confidence interval 1.80 to 9.41). Survival was also influenced by the severity of the exacerbation—exacerbations that necessitated hospital admission or readmission were associated with the poorest survival.38
Patients who are admitted for an exacerbation have an in-hospital mortality of about 10%. Patients with an exacerbation and hypercapnic respiratory failure have a two year mortality rate of about 50%.39 A recent study of 1824 European patients with COPD documented a 45% four year mortality rate after discharge from hospital in those admitted with an exacerbation.40
Incidence of COPD exacerbations across GOLD categories of severity
The severity of airflow limitation is traditionally classified using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) spirometric grading system, which uses specific spirometric cut-off points for simplicity.4 Although this classification system correlates poorly with health related quality of life,41 numerous studies suggest that the risk of COPD exacerbations, hospital admission, and death from COPD increase with worsening of GOLD spirometric stage.42 43 44
A recent longitudinal cohort study enrolled 2138 patients with COPD whose post-bronchodilator FEV1 was less than 80% of predicted.42 Patients were followed prospectively for three years, and the rate of moderate exacerbations that needed treatment with systemic steroids or antibiotics (or both) and severe exacerbations that required hospital admission was recorded. The study found a mean incidence of 1.21 exacerbations per patient year among the entire cohort and that incidence was associated with GOLD stage of airflow obstruction at baseline. Patients with GOLD stage II COPD (FEV1 50-80% of predicted) had 0.85 exacerbations per patient year that needed treatment with systemic steroids or antibiotics (or both). However, this figure was 1.34 for those with GOLD stage III COPD (FEV1 30-50% of predicted) and 2.00 for those with the most severe GOLD stage IV COPD (FEV1 <30% of predicted).42
Exacerbations become more frequent and severe as the severity of COPD increases. However, a distinct group of patients seems to be susceptible to exacerbations, irrespective of disease severity, and these susceptible patients typically experience two or more moderate or severe exacerbations a year.42 This susceptibility phenotype is relatively stable over time and occurs across all severities of airflow obstruction, suggesting that these patients are prone to exacerbations, perhaps as a result of intrinsic susceptibility to particular triggers, such as respiratory infections or pollutants.45
Treatment of acute exacerbations
Corticosteroids
Standard treatment for acute COPD exacerbations includes treatment with bronchodilators, antibiotics, and corticosteroids.46 Clinical trials have shown that the addition of oral or intravenous corticosteroids to antibiotics significantly decreases treatment failure rates in inpatients with COPD exacerbations35 and prevents relapse in outpatients with an exacerbation.34 A recent RCT suggested that, in patients presenting to the emergency department with acute exacerbations of COPD (most of whom were admitted), a five day treatment course with 40 mg of prednisone daily was non-inferior to a 14 day treatment course.36 Patients treated with five days of prednisone had similar rates of re-exacerbation within six months of follow-up but had significantly reduced exposure to glucocorticoids.36
Another recent randomised controlled trial investigated whether blood eosinophilia could be used as a biomarker to predict response to oral corticosteroids in patients with a COPD exacerbation.47 Serum eosinophilia of ≥2% occurs in about 50% of patients who present with a COPD exacerbation.47 48 People in the biomarker directed arm of the study were treated with prednisone for two weeks if their serum eosinophil count was ≥2%, whereas those whose eosinophil count was <2% received placebo. Both groups received antibiotics. Patients with eosinophil counts <2% in the biomarker directed treatment arm (who were treated with placebo) had a greater improvement in quality of life than those in the other arm, who were given prednisone (mean difference in chronic respiratory questionnaire score 0.45; P=0.04). Similarly, treatment failure rates were lower in those with serum eosinophils <2% who were treated with placebo rather than prednisone (15% v 2%; P=0.04).47 These results suggest that a subgroup of patients with COPD exacerbations who have serum eosinophil counts <2% of their total leukocyte count at presentation may not respond to systemic steroids. However, further clinical trials are needed to confirm the results of this relatively small study.
Antibiotics
GOLD guidelines4 and European Respiratory Society guidelines49 advocate antibiotics for patients with acute COPD exacerbations who also have worsening dyspnoea as well as increased sputum volume and purulence, or if any two of these symptoms, particularly increased sputum purulence, worsen. These recommendations are based on older studies that demonstrated better outcomes in outpatients with COPD exacerbations treated with broad spectrum antibiotics such as trimethoprim-sulfamethoxazole, doxycycline, or amoxicillin.1 In addition, a clinical trial in patients with severe exacerbations, who needed mechanical ventilation, showed that ofloxacin significantly reduced mortality associated with severe exacerbations.50
Two recently published RCTs assessed the use of antibiotics in COPD exacerbations. The first study of 223 inpatients with COPD exacerbations compared the addition of seven days of doxycycline or placebo with treatment with systemic corticosteroids.51 It found no significant difference in the primary endpoint of clinical success (61% v 53%; P=0.32), clinical cure, or lung function at day 30.51 By contrast, the other RCT studied 310 outpatients with mild to moderate exacerbations, most of whom were not treated with concomitant oral steroids.20 Amoxicillin-clavulinic acid significantly increased clinical cure rates at the end of treatment (days 9-11) compared with placebo (74% v 60%; difference 14.2%, 3.7% to 24.3%). Treatment with amoxicillin-clavulinic acid was also associated with a prolonged time to next exacerbation compared with placebo.20
Non-invasive ventilation
Non-invasive ventilation using pressure cycled bilevel positive airway pressure has been studied in several RCTs. It decreases respiratory rate and work of breathing, improves acute respiratory acidosis, and decreases the requirement for intubation and invasive ventilation in patients with COPD exacerbations and respiratory failure.52 A decrease in the need for invasive ventilation with this treatment has also translated into lower rates of ventilator associated pneumonia, shorter hospital stays, and reduced mortality.53 GOLD guidelines recommend that patients with severe dyspnea, increased work of breathing, and respiratory acidosis (pH ≤7.35 or arterial carbon dioxide pressure ≥45 mm Hg, or both) should be considered for this treatment, provided they are conscious and able to protect their airway and deal with respiratory secretions.4
New potential treatments for COPD exacerbations
Novel anti-inflammatory drugs
Several RCTs of novel drugs for the treatment of COPD exacerbations have been published recently. A trial from Canada evaluated the TNF-α antagonist etanercept as an anti-inflammatory treatment for this condition.48 The investigators randomized 81 patients with a COPD exacerbation to treatment with prednisone (40 mg/day for 10 days) or etanercept 50 mg given subcutaneously on the day of the exacerbation and seven days later. Both groups were treated with antibiotics (levofloxacin) plus long acting bronchodilators. No significant difference was seen in lung function at 14 days or treatment failure at 90 days (32% v 40%; P=0.44). A subgroup analysis suggested that prednisone was more effective than etanercept in patients who presented with serum eosinophils greater than 2%.48
A similar study of alternative anti-inflammatory treatment randomized 119 inpatients with an exacerbation to oral treatment with the anti-leukotriene inhibitor zileuton 600 mg four times daily or placebo. Patients were treated with 14 days of oral prednisone plus an antibiotic. The study found no significant difference in duration of hospital stay and treatment failure rates.54
Novel enhanced secretion clearance techniques
A recent RCT evaluated positive expiratory pressure therapy to enhance sputum clearance in 90 inpatients with a COPD exacerbation. Patients were randomized to receive this new treatment or usual care while in hospital. The addition of positive expiratory pressure therapy did not significantly improve short term outcomes, such as respiratory symptoms at day of discharge, or disease specific quality of life at eight weeks. Similarly, rates of exacerbation and admission to hospital did not differ between the two treatment groups during the six months after discharge.55
Early inpatient respiratory rehabilitation during an exacerbation
An RCT of 389 people evaluated early inpatient pulmonary rehabilitation begun within 48 hours of admission to hospital for an acute exacerbation and continued for six weeks after discharge. It found no significant effect of early pulmonary rehabilitation on readmission rates in the year after initial admission (hazard ratio 1.1, 0.86 to 1.43; P=0.440) compared with usual care. An increase in mortality was seen in the intervention group at one year (odds ratio 1.74, 1.05 to 2.88; P=0.031), but not during the intervention period or at six months. Physical performance and health status recovered after discharge in both groups, with no significant difference between groups at one year. The authors concluded that early rehabilitation during hospital admission for an acute exacerbation did not reduce the risk of subsequent readmission or enhance recovery of physical function after the initial event.56
Summary: acute management of COPD exacerbations
Despite extensive research, the medical management of COPD exacerbations has not changed substantially over the past 25 years (box). Recent studies evaluating new anti-inflammatory drugs, intensive chest physiotherapy, and early inpatient pulmonary rehabilitation have all failed to show obvious benefits. More research is needed to improve the treatment of these exacerbations and to prevent treatment failure and relapse.
Acute management of moderate to severe exacerbations of chronic obstructive pulmonary disease
Supplemental oxygen: titrate to keep oxygen saturation 90-94%
Short acting β agonist and an anticholinergic bronchodilator
Oral prednisone 40 mg daily for five days
Add antibiotics (amoxicillin-clavulinic acid, a respiratory fluoroquinolone, or a macrolide) if the patient has at least two of the following symptoms:
Worsening dyspnea
Increased sputum volume
Increased sputum purulence (particularly if this is one of the symptoms)
Consider non-invasive ventilation for patients with increased work of breathing and respiratory acidosis (pH <7.35)
Prevention of COPD exacerbations
Given the global health, social, and economic importance of this condition, the prevention of exacerbations is now recognized as a primary goal of maintenance therapy for COPD.4 Several drug and non-drug based interventions have been studied in clinical trials, with the aim of decreasing the frequency and severity of exacerbations (table⇓).57
Pharmacologic treatments for the prevention of acute exacerbations of chronic obstructive pulmonary disease
Vaccinations
Influenza vaccine reduces the rate and severity of influenza symptoms, including respiratory ones. A meta-analysis of 11 trials, including six performed exclusively in patients with COPD, found that, in patients with COPD, influenza vaccine significantly reduced the total number of exacerbations per patient compared with those who received placebo (weighted mean difference −0.37, −0.64 to −0.11; P=0.006).58
A meta-analysis of seven trials that assessed the effects of a 23 valent pneumococcal vaccine in patients with COPD found no significant effect on morbidity or mortality.59 The reduction in likelihood of acute exacerbations of COPD from two studies of 216 people was not significant (odds ratio 0.58, 0.30 to 1.13). The pooled results from three studies of 888 people showed no significant reduction in all cause mortality up to 48 months after vaccination (0.94, 0.67 to 1.33).59
Long acting bronchodilators
Two classes of bronchodilators are in widespread use for COPD: long acting antimuscarinic agents (LAMAs) and long acting β agonists (LABAs). Bronchodilators clearly have a role in the prevention of COPD exacerbations. Studies suggest that dyspnea during an exacerbation is caused by acute increases in expiratory airflow limitation and air trapping, which increase levels of dyspnea when they exceed a threshold value.21 22 By improving expiratory airflow when patients are stable, long acting bronchodilators decrease baseline air trapping and move the patient further away from the critical threshold of air trapping that is associated with a COPD exacerbation.
LAMAs
The tiotropium dry powder inhaler is the best studied LAMA.
The most recent systematic review on chronic tiotropium therapy in COPD suggests that, compared with placebo, tiotropium reduces COPD exacerbations by 22% (odds ratio 0.78, 0.70 to 0.87).60
Two RCTs included in the review were pivotal to the result. The first examined the role of tiotropium versus placebo added to standard treatment in decreasing exacerbations in 1829 patients treated in the US.74 Tiotropium significantly decreased the proportion of patients who experienced one or more exacerbations during six months of treatment (27.9% v 32.3%; P=0.037).
The second RCT, termed the UPLIFT study, assessed the use of tiotropium in more than 5900 patients. It found a significant 14% reduction in exacerbations over four years in people treated with tiotropium compared with those who received usual care for their COPD (0.73 v 0.85 exacerbations per person year; relative risk 0.86, 0.81 to 0.91).14
Newer LAMAs are becoming available for the treatment of COPD. Tiotropium is available in an aqueous solution inhaler (tiotropium Respimat) in several countries in Europe. An RCT of more than 17 000 patients with COPD compared tiotropium dry powder inhaler with tiotropium aqueous inhaler over a mean of 2.3 years. The mortality rate was non-inferior for aqueous tiotropium compared with standard dry powder inhaler tiotropium. Time to first exacerbation and rates of exacerbation over the entire study period were also equivalent.13 These data suggest that aqueous tiotropium may have similar efficacy to dry powder tiotropium in preventing exacerbations.
Other new LAMAs include glycopyrronium bromide and aclidinium bromide. An RCT randomized 1066 patients with COPD to glycopyrronium bromide 50 µg per day or to placebo or open label tiotropium. Compared with placebo, glycopyrronium significantly reduced the risk of moderate to severe exacerbations by 34% (P=0.001). This reduction in exacerbations was comparable to that seen with open label tiotropium.75
A second RCT of glycopyrronium versus placebo had similar results. Glycopyrronium significantly reduced the time to first moderate or severe exacerbation of COPD by 31% compared with placebo (hazard ratio 0.69, 0.50 to 0.95; P=0.023).76 No studies have investigated whether aclidinium bromide reduces exacerbations relative to placebo or to its active comparators.
LABAs
Clinical studies suggest that LABAs can also prevent exacerbations, although the effect size is slightly less than for LAMAs. The TORCH study suggested that salmeterol monotherapy reduces the frequency of exacerbations compared with placebo (0.97 v 1.13 exacerbations per year; relative risk 0.85, 0.78 to 0.93; P=0.001).12 A meta-analysis found that, compared with placebo, LABAs (mainly salmeterol or formoterol) significantly reduced moderately severe COPD exacerbations that necessitated a course of antibiotics or oral steroids (odds ratio 0.73, 0.61 to 0.87) or hospital admission (0.73, 0.56 to 0.95).60
A subsequent RCT of 3444 patients with severe COPD and a history of exacerbations compared indicaterol, a new once daily LABA, to tiotropium. Tiotropium was significantly more effective at preventing exacerbations than indicaterol over one year (rate ratio 1.29 in favour of tiotropium).77
LABA-LAMA combinations
Several combination LABA-LAMA inhalers are in the final stages of development and should be available for general use within the next 12-24 months. Of the fixed dose combinations currently under investigation, tiotropium plus olodaterol, umeclidinium bromide plus vilanterol, aclidinium plus formoterol, and glycopyrronium plus indacaterol have the largest phase III clinical trial programs.
To date, only one published study has evaluated whether a LAMA-LABA product can prevent COPD exacerbations. The once daily fixed dose combination LABA-LAMA inhaler QVA149 contains both glycopyrronium (50 µg) and indicaterol (110 µg) in a single inhaler. An RCT in patients with severe to very severe COPD and a history of exacerbations showed that QVA149 significantly decreased the rate of moderate to severe exacerbations by 12% compared with glycopyrronium alone, although QVA149 did not significantly reduce exacerbation rates compared with open label tiotropium.64
Inhaled corticosteroid-LABA combinations
The largest clinical trial to date of inhaled corticosteroid-LABA combination therapy was the three year TORCH study, which randomized 6112 patients to treatment with fluticasone-salmeterol, either monocomponent, or placebo. Patients treated with fluticasone-salmeterol had an annual rate of 0.85 exacerbations per person compared with 1.13 in the placebo group (rate ratio 0.75, 0.69 to 0.81), and 0.97 in the group treated with salmeterol (0.88, 0.81 to 0.95).12
A meta-analysis confirmed that inhaled corticosteroid-LABA combination inhalers significantly reduce COPD exacerbations when compared with placebo (0.73, 0.69 to 0.78).78 A second meta-analysis confirmed that they also reduced exacerbations when compared with LABA alone (0.76, 0.68 to 0.84).62
Triple therapy (inhaled corticosteroid-LABA plus LAMA)
An RCT randomized of 449 patients to tiotropium plus placebo, tiotropium plus salmeterol, or tiotropium plus fluticasone-salmeterol for one year. The primary endpoint was the proportion of patients who experienced a moderate or severe exacerbation over one year. Although tiotropium plus fluticasone-salmeterol did not significantly decrease exacerbations compared with tiotropium plus placebo (0.85, 0.65 to 1.11), it reduced the number of severe exacerbations that necessitated hospital admission by 47% (0.53, 0.33 to 0.86).10
A similar RCT that evaluated triple therapy with tiotropium plus placebo or tiotropium plus budesonide-formoterol found a 62% reduction in exacerbations (0.38, 0.25 to 0.57) and a 65% reduction in hospital admissions or emergency department visits (0.35, 0.16 to 0.78).63 However, the study was limited by a short duration of three months, and the relatively high rate of exacerbations in the group randomized to tiotropium plus placebo may reflect the effect of inhaled steroid withdrawal.
Potential increased risk of pneumonia associated with inhaled corticosteroid containing therapies
Although inhaled corticosteroids are not indicated as monotherapy for COPD, products that contain them (corticosteroid-LABA combinations and “triple therapy” combinations) are widely used to treat chronic COPD and prevent exacerbations. Recent clinical trials, including the TORCH study, suggested that pneumonia (a listed adverse effect) was more prevalent in patients who used fluticasone or fluticasone-salmeterol combination products.12 However, because none of the clinical trials was designed to assess the risk of pneumonia, radiographic confirmation of pneumonia was not usually obtained, and the extent to which pneumonia events may have been confused with COPD exacerbations was unclear. Increased pneumonia events were not associated with increased mortality in patients treated with inhaled corticosteroids in these clinical trials.
Recent analysis of the new inhaled corticosteroid-LABA product fluticasone furoate-vilanterol suggests an increased risk of pneumonia. These clinical trials required pneumonia to be confirmed as an adverse event on chest radiography. In an integrated analysis of two replicate one year studies in patients with COPD the number of pneumonia events per 1000 patient years was 42.3 in the vilanterol-treated group and 97.9 in the fluticasone furoate-vilanterol treated group. This suggests that treatment with fluticasone furoate in patients with COPD more than doubled the relative risk of pneumonia.79 80 The exposure adjusted cases of fatal pneumonia were 0 in the patients treated with vilanterol but 8.8 per 1000 patient years in those treated with fluticasone furoate-vilanterol.
The risk of pneumonia may not be a class effect and may be higher with certain inhaled corticosteroid products than others. A recently published administrative database study of 163 000 patients with COPD from Quebec identified more than 20 000 serious pneumonia events during 5.4 years of follow-up. Use of inhaled corticosteroid was associated with a 69% increase in the rate of serious pneumonia (relative risk 1.69, 1.63 to 1.75). The increased risk declined gradually after inhaled corticosteroid was stopped and disappeared after six months (1.08, 0.99 to 1.17). The risk of pneumonia seemed to be higher with fluticasone (2.01, 1.93 to 2.10) than with budesonide (1.17, 1.09 to 1.26).81
Similarly, a meta-analysis of seven large clinical trials in which 3801 patients were on inhaled budesonide and 3241 were on control treatment found no significant difference between treatment groups in the occurrence of pneumonia as an adverse event or a serious adverse event (adjusted hazard ratio 1.05, 0.81 to 1.37).82
Risk factors for pneumonia in patients with COPD receiving fluticasone furoate-vilanterol include current smoking, a history of pneumonia, a body mass index less than 25, and FEV1 less than 50% of predicted. It therefore seems reasonable to consider using a budesonide containing inhaled corticosteroid-LABA combination in patients with risk factors that might predispose them to pneumonia. It is also advisable to keep doses of inhaled corticosteroid to the lowest effective dose in patients with COPD and to be vigilant in searching for pneumonia in these patients because symptoms of pneumonia can often overlap with those of an acute exacerbation.83
Phosphodiesterase enzyme inhibitors
Clinical trials have shown that the selective phosphodiesterase 4 inhibitor roflumilast reduces COPD exacerbations in a subpopulation of patients with symptoms of chronic bronchitis (chronic cough and sputum production) who have had at least one exacerbation within the past year. In this subgroup, two clinical trials of more than 3000 patients have shown that roflumilast reduces exacerbations by 17% compared with placebo (rate ratio 0.83, 0.75 to 0.92).65 These effects have not been studied when the drug is added to inhaled corticosteroid-LABA combination therapy or triple therapy. The drug’s gastrointestinal side effects, such as nausea, diarrhea, and weight loss, may also limit its effectiveness in some patients.
Antibiotics
Moxifloxacin is a respiratory fluoroquinolone with activity against bacteria that are associated with COPD exacerbations. One RCT randomized stable patients with COPD to oral moxifloxacin 400 mg (n=573) or placebo (n=584) once a day for five days. Treatment was repeated every eight weeks for a total of six courses. At 48 weeks, the odds ratio of having an exacerbation was not significantly lower in the moxifloxacin group in the intent to treat analysis (0.81, 0.645 to 1.008; P=0.059),65 although it was significantly lower in the per protocol analysis (0.75, 0.565 to 0.994). Guidelines do not currently recommend pulsed antibiotic therapy to prevent exacerbations.84
Macrolide antibiotics have pleiotropic immunomodulatory and anti-inflammatory properties in addition to their antibiotic effects. A one year RCT of 1142 patients randomized them to 250 mg of azithromycin once daily or placebo, in addition to their usual drugs for COPD. After one year, the rates of exacerbation were 1.48 per patient year in the azithromycin group and 1.83 per patient year in the placebo group, suggesting a 17% reduction in exacerbations with daily azithromycin (rate ratio 0.83, 0.72 to 0.95).67 Smaller studies have also shown similar reductions with azithromycin, and a recent meta-analysis of six trials found a 37% relative risk reduction (0.63, 0.45 to 0.87) in COPD exacerbations in patients taking macrolides versus placebo.68
Controversies related to azithromycin
Azithromycin is a potent inducer of antimicrobial resistance. In the above RCT, the incidence of macrolide resistance, as measured in nasopharyngeal flora, was significantly higher in those treated with azithromycin versus placebo (81% v 41%).67 The impact of the widespread use of macrolides to prevent COPD exacerbations on bacterial flora in the wider community is hard to quantify, and there is concern that widespread outpatient use of azithromycin may induce macrolide resistance in communities.68
Azithromycin has very occasionally been associated with prolongation of the Q-T interval and ventricular arrhythmias.85 A study from a Tennessee Medicaid cohort found that relative to amoxicillin, azithromycin was associated with an increased risk of death from cardiovascular disease (hazard ratio 2.49, 1.38 to 4.50; P=0.002) and death from any cause (2.02, 1.24 to 3.30; P=0.005), with an estimated 47 additional deaths from cardiovascular disease per one million courses.86 However, a study of Danish adults aged 18-64 years found no increased risk of death with azithromycin use relative to other antibiotics. Compared with penicillin V potassium, current azithromycin use was not associated with an increased risk of cardiovascular death (rate ratio 0.93, 0.56 to 1.55).87
Given the uncertainties related to antibiotic resistance and potential cardiac toxicity, the most recent 2013 GOLD guidelines do not recommend once daily azithromycin to prevent COPD exacerbations.4 Most physicians reserve azithromycin for patients with relatively severe COPD and a history of frequent exacerbations. Patients with a history of cardiac disease, specifically long Q-T syndrome or ventricular arrhythmias, should probably not receive chronic therapy with azithromycin.
Statins
A recent nested case-control study from Taiwan suggested that statin use may be associated with a reduction in COPD exacerbations.88 A multicenter RCT of simvastatin 40 mg once daily was recently completed in the US and Canada. The primary aim of this study was to investigate whether simvastatin prevented COPD exacerbations. The study recruited 885 patients and followed them for a mean of 640 days. Exacerbation rates in the simvastatin and placebo groups were similar (1.36 (standard deviation 1.61) per year v 1.39 (1.73) per year; P=0.539). Median days to first exacerbation were similar (223 v 231 days; P=0.342). These results suggest that simvastatin 40 mg daily does not affect exacerbation rates or time to first exacerbation in patients with COPD.69
Mucolytics
Data on the use of mucolytics, such as N-acetylcysteine, to prevent COPD exacerbations are contradictory. A large European clinical trial enrolled 523 patients with COPD and randomly assigned them to 600 mg daily N-acetylcysteine or placebo. Patients were followed for three years. The number of exacerbations each year did not differ between groups (1.25 (standard deviation 1.35) v 1.29 (1.46); hazard ratio 0.99, 0.89 to 1.10; P=0.85).77
After publication of this study, a smaller trial from Hong Kong randomized 120 patients with COPD to one year of treatment with N-acetylcysteine 600 mg twice daily or placebo. At one year the frequency of exacerbations was reduced in the N-acetylcysteine group versus the placebo group (0.96 v 1.71 exacerbations per year; P=0.019).71
Finally, a third larger RCT randomized 1006 Chinese patients with moderate to severe COPD to treatment with N-acetylcysteine 600 mg twice daily or placebo for one year. After one year, there were 497 acute exacerbations in 482 patients in the N-acetylcysteine group (1.16 exacerbations per patient year) and 641 acute exacerbations in 482 patients in the placebo group (1.49 exacerbations per patient year; risk ratio 0.78, 0.67 to 0.90; P=0.0011).72
The therapeutic effects of N-acetylcysteine may be dose dependent, so that although 600 mg once daily was ineffective in the European study, 1200 mg daily was effective in the two later Chinese studies. However, in the last two trials all patients were ethnic Chinese, so a population effect (linked to genetic, environmental, or dietary factors) that explains the effectiveness of N-acetylcysteine in these patients cannot be excluded.89
In addition, only 10% of the patients in these last two trials used LAMAs and a relatively high proportion (27%) used oral theophylline, which may render the results of the study less applicable to North American and European patients, in whom LAMA use is common and theophylline use is relatively rare. Finally, the larger Chinese study has been criticized because exacerbations were assessed symptomatically by diary cards and were mostly unreported and mild in severity.
Vitamin D
An RCT of 182 patients with moderate to severe COPD and a history of exacerbations explored whether high dose vitamin D, given once monthly over 12 months, could reduce the incidence of exacerbations. The median time to first exacerbation did not differ significantly between vitamin D treated and placebo groups (hazard ratio 1.1, 0.82 to 1.56; P=0.41), and neither did exacerbation rates or hospital admissions.73
Disease self management for prevention of exacerbations
Several RCTs have evaluated disease self management strategies and the effects of these strategies on rates of exacerbation, emergency department visits, hospital admissions, and death. A systematic review has shown that action plans, in the absence of disease education and self management, do not reduce the use of urgent healthcare for exacerbations.90 The provision of such action plans is therefore not recommended in the absence of a disease self management strategy.
Several large RCTs have studied the provision of education on disease self management in addition to treatment action plans. An RCT of 181 patients found that a comprehensive COPD teaching and self management program, in addition to an exacerbation action plan, decreased hospital admissions and emergency department visits for exacerbation by 40% over the one year trial period, relative to usual care.91 A second RCT randomized 741 patients with COPD to a 90 minute education session, an exacerbation action plan, and monthly phone calls or usual care. Results were similar, showing a 41% reduction (22% to 56%) in emergency visits and hospital admissions in patients randomized to the intervention arm.92
However, this subject is controversial. A recent RCT of 426 patients from COPD clinics associated with Veterans’ Affairs hospitals compared an educational program, written action plans, and access to a case manager by phone with usual care. The study was terminated early by the study Data Safety Monitoring Board because of excess mortality in the group randomized to disease self management. Patients randomized to disease self management and action plans were three times more likely to die during the one year study period than those randomized to usual care (hazard ratio 3.00, 1.46 to 6.17).93 The cause of this excess mortality is unclear. Given this result, the safety of disease self management and exacerbation action plans needs further assessment before this strategy can be recommended for all patients.
Looking ahead: new drugs under development
Treatment of exacerbations
A novel p38 mitogen activated protein kinase (MAPK) inhibitor, currently named BCT197, is being developed as an oral anti-inflammatory agent by Novartis for management of acute exacerbations. A phase II trial evaluating this agent against prednisone in patients with exacerbations has been completed, but results have not yet been released.94 Bedoradrine is a highly selective β adrenergic agent for management of exacerbations. In a phase II study in patients with an exacerbation, this agent was given by slow intravenous injection and resulted in prolonged bronchodilatation without an increase in adrenergic adverse events.95
Prevention of exacerbations
Several drug companies are developing triple combinations of an inhaled corticosteroid, LABA, and LAMA. GlaxoSmithKline is developing a fluticasone-vilaneterol-umeclidinium product that will be administered in a single inhaler, which is likely to undergo clinical trials to determine whether it is effective at preventing exacerbations of COPD.
The effect of roflumilast plus an inhaled corticosteroid-LABA fixed dose combination on exacerbations is being investigated in a one year randomized double blind placebo controlled phase III-IV study.96
Phosphodiesterase 3 is an important mediator of airway smooth muscle relaxation, as confirmed by the observation that phosphodiesterase 3 inhibitors cause bronchodilatation in people with asthma.97 Combined phosphodiesterase 3 and 4 inhibitors, such as RPL554, could therefore relax airway smooth muscle and suppress inflammation. These drugs are currently being investigated for the treatment of COPD symptoms and for the prevention of exacerbations,98 and may also be investigated as acute treatment of exacerbation.
Other compounds in early phase development include monoclonal antibodies directed at the interleukin 1 receptor. Medimmune-8986 is a human monoclonal antibody that inhibits the binding and activation of interleukin 1a and interleukin 1b. These cytokines are thought to be involved in the pathogenesis of exacerbation, and a trial of patients with moderate to severe COPD and a history of frequent exacerbations is due to begin shortly.95
MAPK inhibitors are potentially attractive agents that can inhibit inflammatory responses to cigarette smoke and respiratory viruses. Phase II studies of inhaled MAPK inhibitors, such as the Janssen product JNJ-49095397, are currently assessing short term improvements in airflow limitation and symptoms as well as longer term effects on the incidence of COPD exacerbations.99
Conclusion
Patients with COPD are prone to acute respiratory exacerbations, which can develop suddenly and explosively or subacutely over several days. Exacerbations become more frequent and severe as airflow obstruction related to COPD increases, although a distinct subgroup of patients seems to be susceptible to frequent exacerbations irrespective of disease severity. The median duration of recovery from exacerbations is seven to 10 days for peak flow and 11-13 days for other symptoms. Unfortunately, 24-27% of patients do not respond adequately to initial treatment for exacerbations. These patients experience either a relapse or a second exacerbation that requires additional urgent treatment within 30 days. Clinical trials exploring alternative anti-inflammatory treatments instead of corticosteroids, intensive chest physiotherapy, and early inpatient pulmonary rehabilitation for treatment of exacerbations have all failed to show obvious benefits. Treatment for exacerbations has not evolved over many years and still revolves around short acting bronchodilators, oxygen, corticosteroids, and antibiotics.
Considerable recent research has focused on preventing exacerbations in susceptible patients. Chronic treatments that have been shown to prevent and reduce rates of exacerbation include LABAs, LAMAs, and inhaled corticosteroid-LABA combinations. Triple therapy with a combination of these products may provide additional benefits. Roflumilast reduces exacerbations in patients with a chronic bronchitis phenotype, and azithromycin, when added to usual drugs for COPD, significantly reduces the risk of an exacerbation. Potential side effects of roflumilast and azithromycin may limit their effectiveness in the general COPD population. Many new potential bronchodilators and anti-inflammatory drugs are being studied in ongoing clinical trials to try to generate alternatives to treat and prevent exacerbations in susceptible patients.
Future research questions
Exacerbations of chronic obstructive pulmonary disease (COPD) are currently diagnosed on the basis of clinical criteria alone. Could a sensitive and specific blood or sputum derived diagnostic biomarker be developed?
Do all patients with COPD exacerbations benefit from prednisone? Can a more selective anti-inflammatory treatment be developed?
Will new anti-inflammatory drugs—such as phosphodiesterase 3 inhibitors, mitogen activated protein kinase inhibitors, statins, and triple therapy combination inhalers—be more effective than current drugs in preventing exacerbations in those at risk?
Notes
Cite this as: BMJ 2014;349:g5237
Footnotes
Contributors: SDA was the sole author and is guarantor.
Competing interests: I have read and understood BMJ policy on declaration of interests and declare the following interests: I have served on advisory boards for Boerhinger-Ingelheim, Astra-Zeneca, and Novartis and have been paid about $10 000 (£6000; €7530) for these activities in the past 24 months.
Provenance and peer review: Commissioned; externally peer reviewed.