Angiotensin receptor blockers and risk of myocardial infarction: meta-analyses and trial sequential analyses of 147 020 patients from randomised trials
BMJ 2011; 342 doi: https://doi.org/10.1136/bmj.d2234 (Published 26 April 2011) Cite this as: BMJ 2011;342:d2234
- Sripal Bangalore, director of research1, assistant professor of medicine2,
- Sunil Kumar, fellow in cardiovascular medicine3,
- Jørn Wetterslev, chief physician4,
- Franz H Messerli, director, hypertension program; professor of clinical medicine5
- 1Cardiac Catheterization Laboratory, New York University School of Medicine, Leon H Charney Division of Cardiology, New York, NY 10016, United States
- 2New York University School of Medicine, Leon H Charney Division of Cardiology, New York
- 3University of Nebraska, Omaha, Nebraska
- 4Copenhagen Trial Unit, Center for Clinical Intervention Research, Rigshospitalet, Copenhagen University Hospital, Denmark
- 5St Luke’s Roosevelt Hospital and Columbia University, New York
- Correspondence to: S Bangalore sripalbangalore{at}gmail.com
- Accepted 1 March 2011
Abstract
Objectives To evaluate the cardiovascular outcomes and other outcomes associated with angiotensin receptor blockers.
Design Systematic review of randomised controlled trials with meta-analysis and trial sequential analysis (TSA).
Data sources and study selection Pubmed, Embase, and CENTRAL searches for randomised clinical trials, until August 2010, of angiotensin receptor blockers compared with controls (placebo/active treatment) that enrolled at least 100 participants and had a follow-up of at least one year.
Data extraction Myocardial infarction, death, cardiovascular death, angina pectoris, stroke, heart failure, and new onset diabetes.
Results 37 randomised clinical trials included 147 020 participants and had a total follow-up of 485 166 patient years. When compared with controls (placebo/active treatment), placebo, or active treatment, angiotensin receptor blockers were not associated with an increase in the risk of myocardial infarction (relative risk 0.99, 95% confidence interval 0.92 to 1.07), death, cardiovascular death, or angina pectoris. Compared with controls, angiotensin receptor blockers were associated with a reduction in the risk of stroke (0.90, 0.84 to 0.98), heart failure (0.87, 0.81 to 0.93), and new onset diabetes (0.85, 0.78 to 0.93), with similar results when compared with placebo or with active treatment. Based on trial sequential analysis, there is no evidence even for an average 5.0-7.5% (upper confidence interval 5-11%) relative increase in myocardial infarction (absolute increase of 0.3%), death, or cardiovascular death with firm evidence for relative risk reduction of stroke (at least 1%, average 10%) (compared with placebo only), heart failure (at least 5%, average 10%), and new onset diabetes (at least 4%, average 10%) with angiotensin receptor blockers compared with controls.
Conclusions This large and comprehensive analysis produced firm evidence to refute the hypothesis that angiotensin receptor blockers increase the risk of myocardial infarction (ruling out even a 0.3% absolute increase). Compared with controls, angiotensin receptor blockers reduce the risk of stroke, heart failure, and new onset diabetes.
Introduction
The provocative editorial by Verma and Strauss in the BMJ in 20041 stating that angiotensin receptor blockers “may increase myocardial infarction—and patients may need to be told” led to extensive scrutiny of outcome data with these drugs. This controversy was a direct fallout from the publication of the valsartan antihypertensive long term use evaluation (VALUE) trial,2 in which the primary hypothesis stated that “in hypertensive patients at high cardiovascular risk, for the same level of blood pressure control, valsartan will be more effective than amlodipine in reducing cardiac morbidity and mortality.” Unexpectedly, there was a significant 19% relative increase in the prespecified secondary outcome measure of myocardial infarction in the valsartan arm compared with the amlodipine arm.
In 2008 a Cochrane Collaboration review found angiotensin receptor blockers to be as effective as angiotensin converting enzyme inhibitors at reducing blood pressure, though the effect was modest.3 4 The blood pressure lowering treatment trialists’ collaboration has shown similar blood pressure dependent effects of angiotensin converting enzyme inhibitors and angiotensin receptor blockers for the risk of stroke, coronary heart disease, and heart failure.5 The authors cautioned, however, that there was evidence of a blood pressure independent effect on the risk of major coronary disease events only for angiotensin converting enzyme inhibitors, not for angiotensin receptor blockers. In addition, more recent trials like the Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET),6 a thorough, double blind prospective randomised trial, documented equal outcome efficacy of an angiotensin receptor blocker (telmisartan) and an angiotensin converting enzyme inhibitor in a high risk population, though there was a trend towards better prevention of stroke in the angiotensin receptor blocker arm and towards better prevention of coronary artery disease in the angiotensin converting enzyme inhibitor (ramipril) arm.
We evaluated the risk of cardiovascular and other outcomes with angiotensin receptor blockers in general and tested the hypothesis of increased risk of myocardial infarction with angiotensin receptor blockers found in previous studies and analyses.
Methods
Eligibility criteria
We searched Pubmed, Embase, and CENTRAL using the terms: ‘angiotensin receptor blockers’, ‘angiotensin receptor antagonists’, ‘ARBs’, and the names of individual angiotensin receptor blockers in humans until August 2010. Appendix 1 on bmj.com gives details of the search and the MeSH terminologies used. We checked the reference lists of review articles, meta-analyses, and original studies identified by the electronic searches to find other eligible trials. There was no language restriction for the search. Authors of trials were contacted when results were unclear or when relevant data were not reported. In addition, we searched Food and Drug Administration (FDA) dockets by hand searching all documents submitted for drug approval/labelling change as well as the minutes from FDA meetings available on the FDA website. There was no formal protocol for this systematic review.
To be included in this analysis, eligible trials had to fulfil the following criteria: randomised clinical trials of participants comparing angiotensin receptor blockers with controls (placebo or active treatment); follow-up of at least one year; at least 100 participants enrolled; and reporting any of myocardial infarction, death, cardiovascular death, angina pectoris, stroke, heart failure, and new onset diabetes mellitus. We excluded studies in which angiotensin receptor blockers were not first line agents or studies/treatment arms in which angiotensin receptor blockers were used in combination with an angiotensin converting enzyme inhibitor.
Selection and quality assessment
Two authors (SB and SK) independently assessed trial eligibility and risk of trial bias and extracted data (κ=0.96). Disagreements were resolved by consensus. The risk of bias was assessed by using the components recommended by the Cochrane Collaboration7: sequence generation of allocation; allocation concealment; blinding of participants, staff, and outcome assessors; incomplete outcome data; selective outcome reporting; and other sources of bias. The trials did not differ for the last three components. Trials with high or unclear risk for bias for any one of the first three components were considered as at high risk of bias. Otherwise, they were considered as low risk of bias.
Data extraction and synthesis
We evaluated myocardial infarction, death, cardiovascular death, angina pectoris, stroke, heart failure, and new onset diabetes mellitus. In all of the analyses reported, “control” refers to either placebo or active treatment comparator.
Statistical analysis
We carried out an intention to treat meta-analysis in line with recommendations from the Cochrane Collaboration and the PRISMA statement7 8 using standard software (Stata 9.0, StataCorp, TX).9 Heterogeneity was assessed with the I2 statistic.10 I2 is the proportion of total variation observed between the trials attributable to differences between trials rather than sampling error (chance) with I2 <25% considered as low and I2 >75% as high. The pooled effect for each grouping of trials was derived from the point estimate for each separate trial weighted by the inverse of the variance (1/SE²). The risk ratio was calculated with the random effects model of DerSimonian and Laird.11 Publication bias was estimated visually with funnel plots and with Begg’s test and the weighted regression test of Egger.12 Given that the results might be different based on the comparison group (placebo v active treatment), we performed the primary analyses after stratifying the studies based on the comparator (placebo v active treatment).
Subgroup analyses
We performed subgroup analyses of trials with low risk of bias compared with trials with high risk of bias and cohort enrolled (hypertension v non-hypertension) trials. We estimated the difference between the estimates of the subgroups according to tests for interaction.13 P<0.05 indicates that the effects of treatment differ between the tested subgroups.
Trial sequential analysis
In a single trial, interim analyses increase the risk of type I error. To avoid an increase of overall type I error, monitoring boundaries can be applied to decide whether a single randomised trial could be terminated early because of the P value being sufficiently small. Because no reason exists why the standards for a meta-analysis should be less rigorous than those for a single trial, analogous trial sequential monitoring boundaries can be applied to meta-analysis as trial sequential analysis.14 15 Cumulative meta-analyses of trials are at risk of producing random errors because of few data and repetitive testing of accumulating data, and the requirement for the amount of information analogous to the sample size of a single optimally powered clinical trial might not be met.14 15
The underlying assumption for trial sequential analysis is that significance testing and calculation of the confidence intervals are performed each time a new trial is published. Trial sequential analysis depends on the quantification of the required amount of information. In this context, the smaller the required amount, the more lenient the trial sequential analysis, thus the more lenient the criteria for significance.14 15 A required diversity (D2) adjusted information size was calculated, D2 being the relative variance reduction when the meta-analysis model is changed from a random effects into a fixed effect model.16 D2 is the percentage of the variability between trials and constitutes the sum of the variability between trials. It is an estimate of sampling error after consideration of the required information size. D2 is different from the intuitively obvious adjusting factor based on the common quantification of heterogeneity, the inconsistency (I2), which might underestimate the required information size.16
The trial sequential analysis was performed with a desire to maintain an overall 5% risk of type I error, being the standard in most meta-analyses and systematic reviews, and we calculated the required information size (that is, the meta-analysis information size needed to detect or reject an intervention effect of a 20% relative risk reduction for benefit but a stricter more rigorous sequential testing of a 10% and then a 2.5-7.5% relative risk increase for harms, with a risk of type II error of 10-20%, at a power of 80-90%).14 15
Results
Study selection
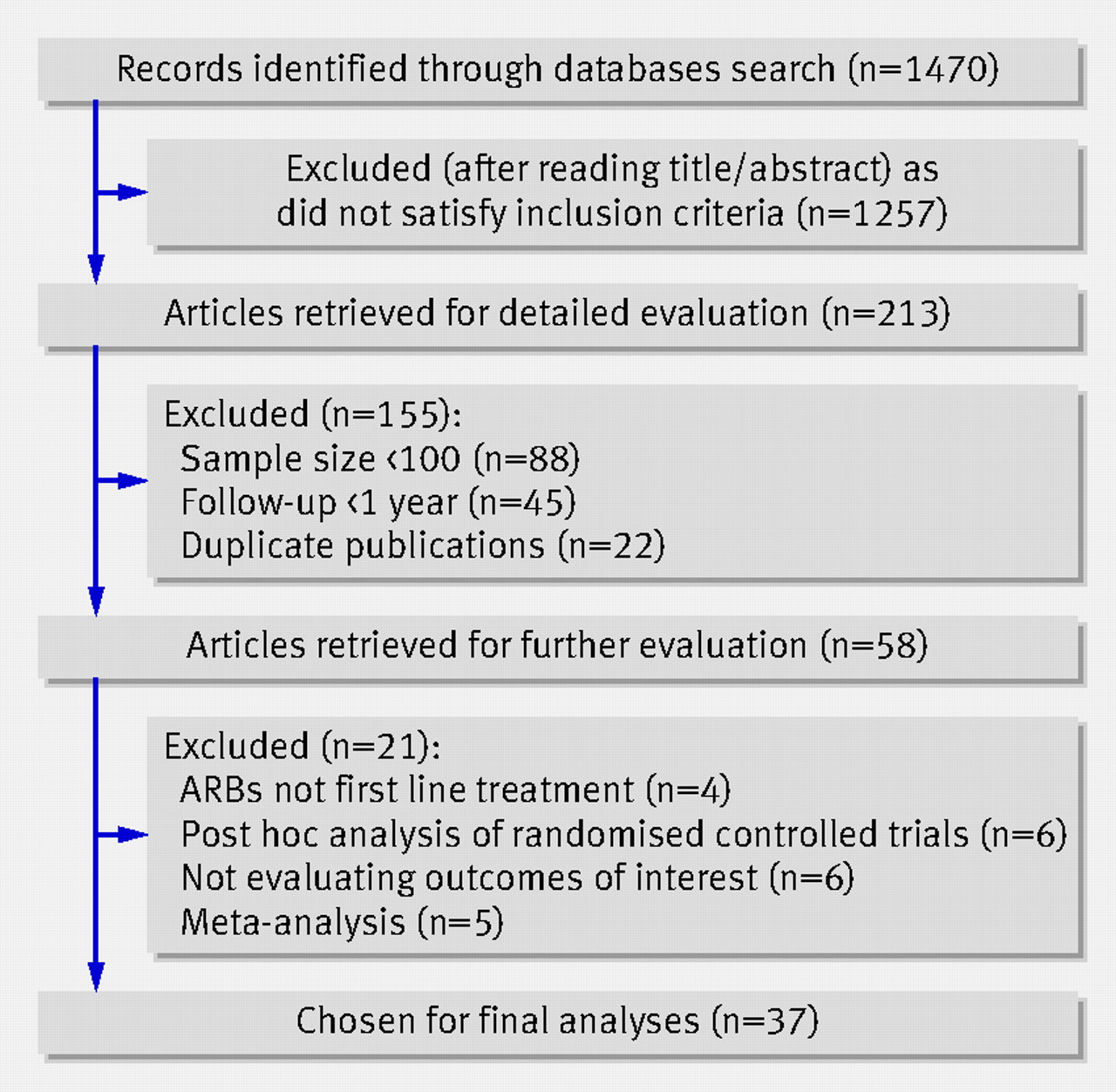
We identified 37 trials (39 comparator arms) that satisfied our inclusion criteria (fig 1⇓). The 39 comparator arms included 17 arms that compared angiotensin receptor blockers with placebo and 22 arms that compared angiotensin receptor blockers with active treatment (table 1⇓). We excluded the combination arms (angiotensin converting enzyme inhibitor plus angiotensin receptor blocker) of the ONTARGET6 and the VALIANT54 trials.

Fig 1 Study identification, selection, and exclusions
{kind=link}
Baseline characteristics of trials included in systematic review of angiotensin receptor blockers and risk of myocardial infarction
Baseline characteristics
Tables 1 and 2 summarise the baseline characteristics of the included trials⇑ ⇓. The 37 trials randomised 147 020 participants, 73 298 (49.8%) to angiotensin receptor blockers and 73 722 (50.2%) to controls. The average follow-up was 3.3 years (range 1-6.5 years), with a total follow-up across all trials of 485 166 patient years. Among the 37 randomised controlled trials, 12 were considered at high risk of bias (table 2) and the rest as low risk. Data on outcomes were abstracted both from the original publication and the Food and Drug Administration dockets (when available) (table 2)⇓.
Blood pressure, dose of drugs used, and quality of included trials in systematic review of angiotensin receptor blockers and risk of myocardial infarction
Angiotensin receptor blockers and outcomes
Angiotensin receptor blockers were not associated with any increase in the risk of myocardial infarction when compared with controls (relative risk 0.99, 95% confidence interval 0.92 to 1.07; P=0.85) (fig 2⇓). The results were similar when angiotensin receptor blockers were compared with either placebo or with active treatment (P=0.15 for interaction) (fig 2). There was low to moderate heterogeneity and no evidence for publication bias (see fig A1 in appendix 2 on bmj.com). Similarly, angiotensin receptor blockers were not associated with any increase in the risk of death (1.00, 0.97 to 1.02; P=0.75) (fig 3)⇓, cardiovascular death (0.99, 0.94 to 1.04; P=0.73) (fig 4)⇓, or angina (0.95, 0.85 to 1.06; P=0.37) (fig 5)⇓ when compared with controls. The results were similar when angiotensin receptor blockers were compared with either placebo or with active treatment for all of the above outcomes (P>0.05 for interaction for all comparisons) (figs 2-5). There was no to low heterogeneity and no evidence for publication bias for the outcomes of death and cardiovascular death (see figs A2-A3 in appendix 2 on bmj.com). For the outcome of angina, there was high heterogeneity but no evidence for publication bias (see fig A4 in appendix 2 on bmj.com).

Fig 2 Angiotensin receptor blockers (ARBs) and myocardial infarction, stratified by comparison group (placebo v active treatment)
{kind=link}

Fig 3 Angiotensin receptor blockers (ARBs) and all cause mortality, stratified by comparison group (placebo v active treatment)
{kind=link}

Fig 4 Angiotensin receptor blockers (ARBs) and cardiovascular mortality, stratified by comparison group (placebo v active treatment)
{kind=link}

Fig 5 Angiotensin receptor blockers (ARBs) and angina pectoris, stratified by comparison group (placebo v active treatment)
{kind=link}
In addition, angiotensin receptor blockers were associated with a 10% reduction in the risk of stroke (P=0.01) (fig 6⇓), a 13% reduction in the risk of heart failure (P<0.001) (fig 7)⇓, and a 15% reduction in the risk of diabetes (P<0.001) (fig 8⇓) compared with controls. The results were similar when angiotensin receptor blockers were compared with either placebo or with active treatment for all of the above outcomes (P>0.05 for interaction for all comparisons) (fig 6-8). There was no to moderate heterogeneity and no evidence for publication bias for the outcomes of stroke and heart failure (see figs A4-A5 in appendix 2 on bmj.com). For the outcome of new onset diabetes, there was moderate to high heterogeneity and no evidence for publication bias (see fig A6 in appendix 2 on bmj.com).

Fig 6 Angiotensin receptor blockers (ARBs) (ARBs) and stroke, stratified by comparison group (placebo v active treatment)
{kind=link}

Fig 7 Angiotensin receptor blockers (ARBs) and heart failure, stratified by comparison group (placebo v active treatment)
{kind=link}

Fig 8 Angiotensin receptor blockers (ARBs) and new onset diabetes mellitus, stratified by comparison group (placebo v active treatment)
{kind=link}
Trial sequential analysis
The required diversity (D2=52%) adjusted information size for the outcome of myocardial infarction was calculated based on a proportion of 4.14% events in the control group and evaluating initially for a 10% relative risk increase (absolute risk increase of 0.4% corresponding to a number needed to harm of 250) and then followed by a 7.5% relative risk increase (absolute risk increase of 0.3% corresponding to a number needed to harm of 333) with angiotensin receptor blockers, at α=5%, and β=20% (80% power) (see fig B1 in appendix 3 on bmj.com). The cumulative z curve crosses neither the traditional boundary nor the trial sequential monitoring boundary but does cross the futility boundary, suggesting firm evidence for a lack of even an average 7.5% relative risk increase (upper confidence limit 11%) of myocardial infarction with angiotensin receptor blockers (see fig B1 in appendix 3 on bmj.com). Similarly, the cumulative z curve crossed the futility boundary, suggesting firm evidence for lack of on average a 4% relative risk increase (upper confidence limit 7%) in death (see fig B2 in appendix 3 on bmj.com), a lack of on average a 5% relative risk increase (upper confidence limit 5%) in cardiovascular death (see fig B3 in appendix 3 on bmj.com), and a lack of on average a 15% relative risk increase (upper confidence limit 12%) in angina (see fig B4 in appendix 3 on bmj.com) with angiotensin receptor blockers compared with controls.
For the outcome of stroke, however, the cumulative z curve crossed the traditional boundary but not the trial sequential monitoring boundary, suggesting lack of evidence for a 7.5% relative risk reduction in stroke with angiotensin receptor blockers compared with controls (see fig B4 in appendix 3 on bmj.com). The boundary was crossed, however, for firm evidence for at least a 1% relative risk reduction (average 10%) in stroke compared with placebo. When compared with active treatment, neither the traditional boundary nor the trial sequential monitoring boundary was crossed for a 15% relative risk reduction with angiotensin receptor blockers. In addition, the futility boundary was not crossed, suggesting the need for more evidence to establish additional benefits of angiotensin receptor blockers over active treatment. Similarly, the cumulative z curve crossed the trial sequential monitoring boundary, suggesting firm evidence for at least a 5% relative risk reduction (average 10%) in heart failure with angiotensin receptor blockers (see fig B5 in appendix 32 on bmj.com) and at least a 4% relative risk reduction (average 10%) in diabetes (see fig B6 in appendix 3 on bmj.com) when compared with controls.
Sensitivity analysis
Subgroup analysis based on trial quality (low risk of bias versus high risk of bias) and cohort enrolled (hypertension versus non-hypertension trials) did not make any noticeable difference for the above analyses (table 3⇓). The risk reduction of stroke, angina, and heart failure was higher in trials at high risk of bias compared with those at low risk of bias (though directionally similar) (table 3⇓). Similarly, the risk reduction for heart failure and new onset diabetes was higher in hypertension trials compared with non-hypertension trials (though directionally similar) (table 3).⇓
Sensitivity analysis (angiotensin receptor blockers versus controls) with numbers from random effects model
Discussion
In this meta-analysis we found no evidence to support the theory that angiotensin receptor blockers increase the risk of myocardial infarction. We included 485 166 patient years of follow-up, and, with 80% power, found, on average, a lack of 7.5% relative risk increase (upper confidence limit 11%) (absolute increase of 0.3% corresponding to a number needed to harm of ≥333) of myocardial infarction with angiotensin receptor blockers compared with controls. Similar results were seen for the outcome of death, cardiovascular death, and angina. In addition, the data provide firm evidence for relative risk reduction of stroke (at least 1%, average 10%) (versus placebo only), heart failure (at least 5%, average 10%), and new onset diabetes (at least 4%, average 10%) with angiotensin receptor blockers compared with controls.
Angiotensin receptor blockers—cardioprotection v cerebroprotection
The 2004 results of the VALUE trial,2 in which the angiotensin receptor blocker valsartan produced a significant relative increase in myocardial infarction compared with amlodipine, has fuelled a debate on the safety of this class of drugs. In VALUE, those in the amlodipine arm had a modest but significantly lower blood pressure than those in the angiotensin receptor blockers arm (1.8 mm Hg systolic and 1.5 mm Hg diastolic) and a significantly lower blood pressure in the first three months, but whether this difference can explain the results has been contested.1
Angiotensin II exerts most of its deleterious effects (vasoconstriction, increased cardiac contractility, renal tubular sodium reabsorption, cell proliferation, vascular and cardiac hypertrophy, inflammatory responses, and oxidative stress) via angiotensin I receptors, while the angiotensin II receptors counterbalance some of these effects. Angiotensin receptor blockers exert their action on angiotensin I receptors, which not only block the deleterious effect of angiotensin II but also results in overstimulation of angiotensin II receptors, probably resulting in antihypertrophic and antifibrotic effects. The angiotensin receptor blockers were thus thought to not only provide blockade of the renin-angiotensin system but also to allow for favourable stimulation of angiotensin II receptors. More recent studies, however, seem to suggest that chronic overstimulation of angiotensin II receptors might also exert a hypertrophic and antiangiogenic influence on cardiovascular tissues and that therefore the “long term consequences of ARB therapy might be less beneficial and could even be harmful in some circumstances.”17 In addition, the pluripotential effects of angiotensin converting enzyme inhibitors have been attributed to upstream blockade of the renin-angiotensin axis, which also inhibits the degradation of kinins to inactive metabolites resulting in raised concentration of bioactive kinins such as bradykinin, which has been found to have several possible benefits such as anti-arrhythmic effects and reducing infarct size (mediated through ischaemic preconditioning and nitric oxide/prostacyclin related vascular protection).18 These pathophysiological mechanisms provide some mechanistic insight into the alleged inferiority of angiotensin receptor blockers compared with angiotensin converting enzyme inhibitors and potentially explain the adverse outcomes.2
Since the publication of the VALUE trial, several large randomised trials (ONTARGET, TRANSCEND) have been published that showed no increase in adverse outcomes with angiotensin receptor blockers. None of these trials by themselves had adequate power for the individual outcomes. Our meta-analysis showed firm evidence of a lack of significant effect of angiotensin receptor blockers on myocardial infarction, ruling out even a 0.3% (number need to harm ≥333) absolute increase in the risk of myocardial infarction with angiotensin receptor blockers. The analyses, however, do not rule out a <0.3% absolute increase of myocardial infarction with angiotensin receptor blockers, though this is likely to be clinically less important. The results were similar, with the cumulative z curve crossing the futility boundary for the outcomes of death, cardiovascular death, and angina. In addition, there was a significant benefit for the outcomes of stroke, heart failure, and new onset diabetes mellitus. Whether this is due to angiotensin II receptor stimulation (for example, in the brain) or to better tolerability (and hence a better effect on blood pressure and compliance) of this class of drugs is not known.
Of note, although there was no harm with treatment with angiotensin receptor blockers, despite lower blood pressure compared with placebo, there was no detectable beneficial effect for the outcome of myocardial infarction or cardiovascular mortality. Angiotensin receptor blockers, however, were as effective as the active treatment group for these outcomes. Thus angiotensin receptor blockers, unlike angiotensin converting enzyme inhibitors seem not to have any special “cardioprotective” effects, even when compared with placebo. In contrast, for the outcome of stroke, angiotensin receptor blockers were effective at reducing the risk compared with placebo. When compared with active treatment, there was benefit only in the fixed effects model but not in the random effects model, but the point estimate favoured angiotensin receptor blockers. Trial sequential analysis, however, suggests that we need more data before we can make robust decisions on this outcome.
While the results from our sensitivity analysis were largely similar, the risk reduction in trials at low risk of bias was smaller in magnitude, although significant. Thus the risk reduction for the outcomes of stroke, heart failure, and new onset diabetes with angiotensin receptor blockers is modest.
Trial sequential analysis
Conventional meta-analysis does not take into consideration the information size, the number of accrued events, and the effect size and the inference depends on the test for significance and the confidence interval, which can often be spuriously narrow. Not infrequently, non-significant results are simply inferred as “more evidence is needed.” Trial sequential analysis incorporates both the information size and the effect size and is therefore helpful in making more robust inferences. In the setting of a non-significant result, trial sequential analysis helps decide whether “more evidence is needed” (when the futility boundary is not crossed) or rule out a given effect size (if the futility boundary is crossed), thus reducing this uncertainty. As can been seen in all of the analyses, while conventional meta-analysis promises a greater effect size (for significant results) or lack of small effect size (for non-significant results), the trial sequential analysis, taking into consideration the effect size and information size, is more conservative and probably more accurate. The relative risk and 95% confidence interval for stroke, heart failure, and new onset diabetes from traditional analyses were 0.90 (0.84 to 0.98), 0.87 (0.81 to 0.93), and 0.85 (0.78 to 0.93). For stroke there was a lack of firm evidence (based on trial sequential analysis) for an average of 7.5% relative risk reduction with angiotensin receptor blockers compared with the apparent 10% relative risk reduction suggested in the traditional meta-analysis, the trial sequential analysis adjusted confidence interval being 0.80 to 1.02. We therefore need more data to test for a 7.5% relative risk reduction of stroke with angiotensin receptor blockers. For the outcome of heart failure and diabetes, the cumulative z curve crossed the trial sequential monitoring boundary, suggesting firm evidence for a 10% relative risk reduction in heart failure and diabetes with angiotensin receptor blockers compared with controls instead of the 13% relative risk reduction for heart failure and 15% relative risk reduction for diabetes suggested by the traditional meta-analysis. As trial sequential analysis relies on the accumulated number of events, the effect size, and the information size, the estimate is more conservative and the adjusted confidence interval wider but more reliable as it allows for multiple testing on accumulating data.
Study limitations
As in other meta-analyses, given the lack of data in each trial, we did not adjust our analyses for dose of drugs used or compliance with assigned treatment. Though detailed sensitivity analyses were undertaken, given heterogeneity in the study protocols, clinically relevant differences could have been missed and might be better assessed in a meta-analysis of individual patient data. In addition, there could be additional confounders not accounted for in the analysis. Also, not all of the trials reported each of the outcomes analysed. The subgroup analyses might suffer from multiple testing. The results of the sensitivity analyses are best described as secondary and hypothesis generating only.
What is already known on this topic
Angiotensin receptor blockers are important in the treatment of cardiovascular conditions
Previous studies have shown an increased risk of myocardial infarction with these drugs and have raised concern among physicians and patients
What this study adds
There is firm evidence to refute the hypothesis of angiotensin receptor blockers increasing the risk of myocardial infarction (ruling out even a 0.3% absolute increase)
Compared with controls (active treatment or placebo), angiotensin receptor blockers reduce the risk of stroke, heart failure, and new onset diabetes.
Despite lower blood pressure with angiotensin receptor blockers when compared with placebo, there also was no detectable beneficial effect for the outcome of myocardial infarction or cardiovascular mortality
Notes
Cite this as: BMJ 2011;342:d2234
Footnotes
Contributors: SB is guarantor. SB and FHM were responsible for study concept and design and supervised the study. SB and SK acquired the data, which was analysed and interpreted by SB, JW, and FHM. SB drafted the manuscript, which was critically revised for important intellectual content by SB, SK, JW, and FHM. SB and JW did the statistical analysis.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available available on request from the corresponding author) and declare: no support from any organisation for the submitted work; FHM has been an occasional consultant/speaker for Novartis, Daiichi Sankyo, Sanofi, and Savient Pharmaceuticals and has received grants from Novartis, Forest, and Boehringer Ingelheim; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: Not required.
Data sharing: No additional data available.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.