Population based time trends and socioeconomic variation in use of radiotherapy and radical surgery for prostate cancer in a UK region: continuous survey
BMJ 2010; 340 doi: https://doi.org/10.1136/bmj.c1928 (Published 22 April 2010) Cite this as: BMJ 2010;340:c1928
- Georgios Lyratzopoulos, senior clinical research associate 1,
- Josephine M Barbiere, research associate1,
- David C Greenberg, senior analyst2,
- Karen A Wright, quality assurance/analyst2,
- David E Neal, professor of surgical oncology and honorary consultant urological surgeon3
- 1Department of Public Health and Primary Care, University of Cambridge School of Clinical Medicine, Institute of Public Health, Cambridge CB2 0SR
- 2Eastern Cancer Registration and Information Centre, Cambridge CB22 3AD
- 3University Department of Oncology, Addenbrooke’s Hospital, Cambridge CB2 OQQ
- Correspondence to: G Lyratzopoulos gl290{at}medschl.cam.ac.uk
- Accepted 25 February 2010
Abstract
Objective To examine variation in the management of prostate cancer in patients with different socioeconomic status.
Design Survey using UK regional cancer registry data.
Setting Regional population based cancer registry.
Participants 35 171 patients aged ≥51 with a diagnosis of prostate cancer, 1995-2006.
Main outcome measures Use of radiotherapy and radical surgery. Socioeconomic status according to fifths of small area deprivation index.
Results Over the nine years of the study, information on stage at diagnosis was available for 15 916 of 27 970 patients (57%). During the study period, the proportion of patients treated with radiotherapy remained at about 25%, while use of radical surgery increased significantly (from 2.9% (212/7201) during 1995-7 to 8.4% (854/10 211) during 2004-6, P<0.001). Both treatments were more commonly used in least deprived compared with most deprived patients (28.5% v 21.0% for radiotherapy and 8.4% v 4.0% for surgery). In multivariable analysis, increasing deprivation remained strongly associated with lower odds of radiotherapy or surgery (odds ratio 0.92 (95% confidence interval 0.90 to 0.94), P<0.001, and 0.91 (0.87 to 0.94), P<0.001, respectively, per incremental deprivation group). There were consistently concordant findings with multilevel models for clustering of observations by hospital of diagnosis, with restriction of the analysis to patients with information on stage, and with sequential restriction of the analysis to different age, stage, diagnosis period, and morphology groups.
Conclusions After a diagnosis of prostate cancer, men from lower socioeconomic groups were substantially less likely to be treated with radical surgery or radiotherapy. The causes and impact on survival of such differences remain uncertain.
Introduction
In the United Kingdom, prostate cancer is currently the most common malignancy in men. Its incidence has been increasing, particularly since the late 1980s and early 1990s,1 and is socioeconomically patterned. In the late 1990s and earlier in the present decade the incidence was about 20-40% greater in least deprived individuals.2 3 Five year relative survival has improved substantially over the past 20 years and was about 80% early in the 2000s.4 Like incidence, survival from prostate cancer is also socioeconomically patterned, with an absolute gap as high as 7% in five year relative survival between the least and most deprived individuals.5 Socioeconomic inequalities in survival from prostate cancer have also been described in New Zealand6 and Denmark.7
Socioeconomic differences in use of testing for prostate specific antigen are thought to be partly responsible for both higher incidence and increased survival in less deprived individuals.8 According to this hypothesis, higher uptake of screening for prostate specific antigen in more affluent men leads to diagnosis of a relatively higher proportion of earlier stage (and better prognosis) prostate cancer, which in turn contributes to greater survival of more affluent patients. Although there is some evidence in support of this hypothesis,9 10 because prostate specific antigen testing can take place in both hospital and primary care settings, as well as in the public and the private healthcare sector, directly examining the degree of differential test uptake between men of different socioeconomic status is fraught with practical difficulties. Even if there are differences in the proportion of (early stage) prostate cancer detected by screening in men from different socioeconomic groups, it is also possible that some of the observed inequalities in survival reflect socioeconomic variation in management.8
Optimal treatment for early stage prostate cancer is currently uncertain. The main management options comprise radical surgery, external beam radiotherapy, or active monitoring with biochemical follow-up.11 Which of these strategies is most effective is not known currently, and a major randomised controlled trial comparing active monitoring with radiotherapy and with radical surgery is not expected to report its findings before 2012.12 In addition, a range of other interventional procedures, including cryotherapy, high intensity focused ultrasound (HIFU), and brachytherapy (a form of radiotherapy with radioactive implants) have also been proposed.11 Evidential uncertainty about optimal management could make socioeconomic variation in management more likely.13
We examined whether socioeconomic variation in management exists and quantified the potential size of any such healthcare differences.
Methods
Data
We obtained anonymised information on patients from the Eastern Cancer Registration and Information Centre (ECRIC), one of the eight English population based cancer registries, covering a population of 5.5 million. Incident cases of prostate cancer were defined as those with ICD-10 (international classification of diseases, 10th revision) site codes C61. Using relevant ICD-O morphology codes, we defined two groups: adenocarcinoma (M8140-3) and “unspecified” prostate cancer, comprising “carcinoma” (8010-3) and “neoplasm malignant” (8000-3). Patients with other (rare) histological types were excluded from further analysis. Information relates to residents of the East of England Government Office region aged >50 with a diagnosis in 1995-2006 (this age restriction excluded 246 patients aged ≤50). The latter study year (2006) was the most recent study year for which data were available at the time of the analysis. We chose 1995 as the earliest study year to provide a long enough period that would also encompass recent healthcare policy initiatives, such as the NHS Cancer Plan (published 2002) and the publication of Improving Outcomes Guidance in Urological Cancers (published 2002).
When available, information on stage at diagnosis related to the fifth edition of the tumour, node, metastases (TNM) classification (stages I to IV).14 Based on registration information, Clement Brown (medical director and consultant clinical oncologist, Eastern Cancer Registration and Information Centre) derived information on staging for each case.
Socioeconomic status was assigned with the deprivation score of postcode of residence (index of multiple deprivation 2004 lower super output area score).15 The index is a UK census based (2001) small area statistic measuring different domains of deprivation. A lower super output area typically comprises five coterminous (having a common boundary) and sociodemographically similar output areas (the lowest small area with aggregated census information) and has about 1500 residents. This “homogenous” and low level of aggregation minimises the potential for misattributing individual socioeconomic status by using the “average” socioeconomic profile of a greater sample of individuals.16 We used fifths of the English distribution of lower super output area deprivation scores in our analyses (group 1 (least deprived) to 5 (most deprived)).
Registry staff collect and code information on treatment over at least a six month period from diagnosis. This includes surgical treatments, classified by the Office for Population Censuses and Surveys (fourth revision, OPCS 4) system,17 and radiotherapy. Concordant with previous research, radical surgery (hereafter referred to as “surgery”) treatment status was defined as codes M611-9 (open excision of prostate),18 and the definition for radiotherapy treatment included external beam radiotherapy and brachytherapy.19 Of all patients, 205 (0.6%) were treated by both radiotherapy and surgery. We assumed that the initial clinical management in those patients was more likely to be surgical, and we therefore included such patients in the “surgery” group.19 No information was available about treatment intent nor about comorbidity status.
Analysis
All analyses were carried out with Stata software (StataCorp, College station, TX, USA). We used binary logistic regression models to examine whether stage ascertainment and advanced stage (defined as stages III-IV) at presentation differed by diagnosis period, age, and deprivation. We described the proportion of patients treated with radiotherapy and with surgery by diagnosis period (1995-7, 1998-2000, 2001-3, and 2004-6), age group (51-60, 61-70, 71-80, >80), and deprivation group (1-5). We also examined bivariate associations between deprivation and all of age group, diagnosis period, morphology, and stage.
The effect of each variable category on the probability of radiotherapy or surgery was initially examined by multivariable logistic regression models, adjusted for age, deprivation, diagnosis period, and morphology. We derived odds ratios denoting the probability of treatment for each deprivation group using the least deprived group as reference and, subsequently, entering deprivation group (1-5) as a continuous variable in the same model. The odds ratios obtained from the latter models denote the change in odds ratio by moving from one deprivation group to the one immediately more deprived.
Subsequently, to take into account possible clustering (of patients from different deprivation groups and with different treatment patterns within different hospitals of diagnosis) we used multilevel mixed effects logistic regression models with a random effect for hospital of diagnosis. The xtmelogit command in Stata was used to fit two separate models for the binary outcome variables of surgery and radiotherapy treatment status. Adjustment was made for all other variables used in the non-hierarchical models (as above)—that is, individual level fixed effects were included in the multilevel model for age group, deprivation fifth, diagnosis period, and morphology.
After complete case analysis, in which we did not account for stage, we repeated multivariable logistic regression analyses separately for cases with stage information with adjustment for stage (both for the non-hierarchical and the multilevel models). In addition, we repeated the analysis by sequentially stratifying all models to patients aged ≤70 and those aged >70 (two age groups × two treatments × “all”/staged cases = eight models); patients with early (I-II) and advanced (III-IV) stage (two stage groups × two treatments = four models); diagnosis during an early study subperiod or during 2001-6 (two periods × two treatments × “all”/staged cases = eight models); and adenocarcinoma or “unspecified” tumour type (two tumour groups × two treatments × “all”/staged cases = eight models), producing a set of 28 additional odds ratios and corresponding significance levels for the deprivation effect of either treatment.
Results
Out of a total of 35 353 patients, 182 (0.5%) had rare types of prostate cancer, leaving 35 171 patients for further analysis, of whom 29 628 (84.2%) had adenocarcinoma and 5543 (15.7%) had tumours with unspecified morphology (fig 1)⇓. Overall, stage information was available for 16 020 (45.5%), of whom 305 (1.9%), 11 269 (70.3%), 1675 (10.5%), and 2771 (17.3%) were diagnosed at stages I, II, III, and IV, respectively. During 1995-7, information on stage was available for only 104 (1.4%) because systematic stage registration began in later years. For this reason, when we restricted the analysis to patients with information on stage, we used data only from the nine year period 1998-2006, with stage information for that period being available for 15 916 of 27 970 patients (56.9%).

Fig 1 Flow chart of study population and analysis groups
{kind=link}
Ascertainment of stage was not associated with age or deprivation (table 1)⇓, but more deprived patients were significantly more likely to have been diagnosed with advanced (that is, stage III-IV) disease.
Associations between completeness of ascertainment of stage and “advanced stage” at presentation (defined as stages III-IV) and other variables in men with prostate cancer, 1998-2006
The proportion of patients treated by surgery increased significantly over time, from 2.9% (212/7201) during 1995-7 to 8.4% (854/10 211) during 2004-6 (P<0.001, table 2)⇓. We found similar increasing trends among patients with information on stage (during 1998-2006) though not significantly (P=0.318). Use of radiotherapy remained stable at around 25% throughout the study period, and it was similarly stable over time among patients with stage information.
Proportion of patients treated by radiotherapy or radical surgery by basic characteristics for all men with prostate cancer, 1995-2006 (n=35 171), and patients with stage information, 1998-2006 (n=15 916)
There were small but significant differences between patients from different deprivation groups. On average, more deprived patients were relatively older and were more commonly diagnosed in earlier years of the study period, with unspecified morphology and at more advanced stage (table 3)⇓.
Bivariate association of deprivation (from 1 (affluent) to 5 (most deprived)) with age, diagnosis period, morphology, and stage in men with prostate cancer. Figures are numbers (percentages) unless stated otherwise
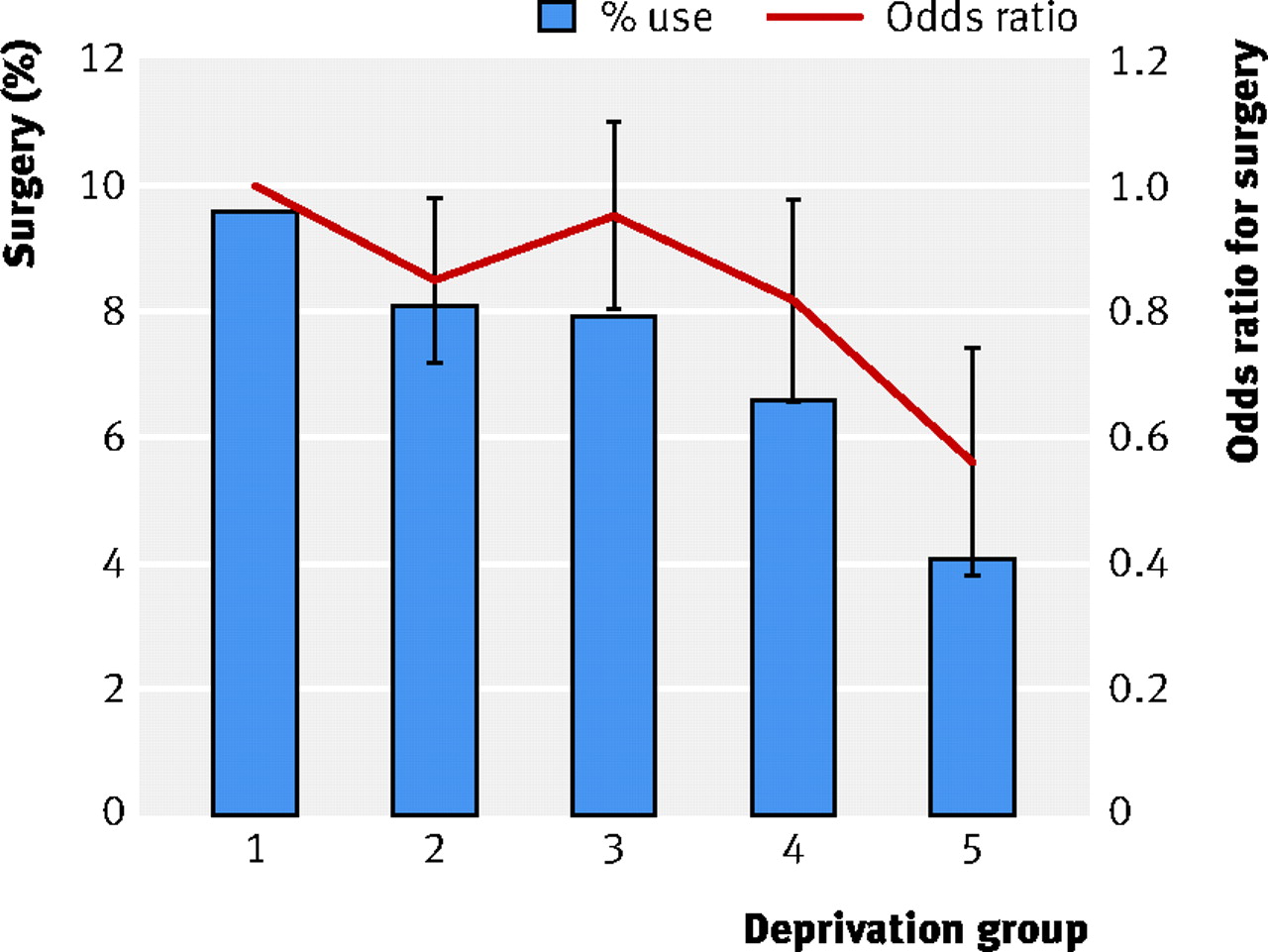
Radiotherapy and surgery were more commonly used in less deprived patients. Among patients in deprivation groups 1 to 5 the proportion treated by radiotherapy was 28.5% (2560/8977), 26.6% (2550/9597), 23.6% (2010/8510), 22.2% (1358/6119), and 21.0% (413/1968), respectively, and for surgery the figures were 8.4% (757/8977), 6.8% (650/9597), 6.5% (551/8510), 5.2% (319/6119), and 4.0% (78/1968) (table 2).⇑ Use of surgery decreased continually with increasing age, while use of radiotherapy increased with age up to age 70 and decreased thereafter. Treatment patterns for deprivation group and age were similar among patients with information on stage. Among such patients, in those treated with surgery, 1% (19/1275), 70% (891/1275), 26% (336/1275), and 2% (27/1275) had stage I, II, III, and IV disease, respectively. In patients treated with radiotherapy, the values were 1% (30/4239), 68% (2877/4239), 11% (486/4239), and 20% (846/4239).
In multivariable analysis, higher deprivation was significantly associated with lower odds of either radiotherapy (odds ratio 0.92, 95% confidence interval 0.90 to 0.94, P<0.001) or surgery use (0.91, 0.87 to 0.94, P<0.001) (table 4 and figs 2 and 4)⇓ ⇓ ⇓. Associations were similar among patients with information on stage (table 4 and figs 3 and 5)⇓ ⇓. Older age was significantly associated with lower probability of use of either treatment. Diagnosis later in the study period was significantly associated with higher probability of surgery and lower probability of radiotherapy.

Fig 2 Percentage of all patients with prostate cancer treated by radiotherapy and odds ratio of use of radiotherapy by deprivation group (odds ratios and 95% confidence intervals adjusted for age, diagnosis period, and morphology)
{kind=link}

Fig 3 Percentage of patients with prostate cancer with information on stage treated by use of radiotherapy and odds ratio of radiotherapy by deprivation group (odds ratios and 95% confidence intervals adjusted for age, diagnosis period, morphology, and stage)
{kind=link}

Fig 4 Percentage of all patients with prostate cancer treated by surgery and odds ratio of surgery by deprivation group (odds ratios and 95% confidence intervals adjusted for age, diagnosis period, and morphology)
{kind=link}

Fig 5 Percentage of patients with prostate cancer with stage information treated by surgery and odds ratio of surgery by deprivation group (odds ratios and 95% confidence intervals adjusted for age, diagnosis period, morphology, and stage)
{kind=link}
Odds ratio of radiotherapy and surgery use by basic characteristic for all cases of prostate cancer, 1995-2006 (n=35 171) and cases with information on stage, 1998-2006 (n=15 916). Logistic regression models adjusted for age group, deprivation group, diagnosis period, morphology, and, where applicable, stage
Multilevel model analysis (at the level of hospital of diagnosis) included 29 805 of 35 171 patients (84.7%) diagnosed in any of the 17 East of England NHS Hospital Trusts (range of number of patients by trust 744 to 3793). This analysis re-affirmed the significant socioeconomic treatment patterns observed in non-hierarchical modelling, both in relation to “all” and in relation to “staged” cases (table 5)⇓.
Multilevel model, with hospital of diagnosis as cluster level. Odds ratio of radiotherapy and surgery by basic characteristics for all cases of prostate cancer diagnosed in one of 17 NHS hospital trusts, 1995-2006 (n=29 805), and those patients with information on stage, 1998-2006 (n=14 830). Logistic regression models adjusted for age group, deprivation group, diagnosis period, morphology, and, where applicable, stage
Moreover, we compared the proportion of patients treated by surgery or radiotherapy in each hospital by deprivation group (that is, the least and one but least deprived groups (groups 1-2) compared with the three relatively most deprived groups (3, 4, and 5). For radiotherapy there was lower use among more deprived patients in 15 of 17 hospitals and higher use among more deprived patients in the two other hospitals (range −7.7%-0.6%, fig 6)⇓. For surgery there was lower use among more deprived patients in 15 of 17 hospitals and higher use among deprived patients in the two other hospitals (range −4.0%-1.2%, fig 7)⇓. The four (of 34) instances that socioeconomic treatment patterns favoured the more deprived all related to four different hospitals, and relative differences were small (figs 6-7). Whether the hospital of diagnosis was a district general hospital or a referral centre did not seem to influence hospital level differences (figs 6-7). The rank correlation coefficient (for deprivation differences in radiotherapy correlated on deprivation differences in surgery) was −0.10 (−0.65 to 0.45, P=0.708); this indicates that there was no correlation between a hospital ranking “high” for inequality in radiotherapy with the same hospital ranking “high” for inequality in surgery use and vice versa. The above observations strongly indicate that socioeconomic differences in treatment patterning were general among the studied hospitals and that, at least in part, the limited instances of relatively small inverse socioeconomic differences could be caused by chance.

Fig 6 Difference (in absolute percentage points) in radiotherapy use between least and most deprived patients (that is, deprivation groups 1-2 v 3-5) by hospital of diagnosis (A-Q) with 95% confidence intervals. Negative values indicate lower use in most deprived category and vice versa
{kind=link}

Fig 7 Difference (in absolute percentage points) in surgery use between least and most deprived patients (that is, deprivation groups 1-2 v 3-5) by hospital of diagnosis (A-Q) with 95% confidence intervals. Negative values indicate lower use in the most deprived category and vice versa
{kind=link}
We also observed less frequent use of either surgery or radiotherapy in more deprived patients in each one of the 28 “stratified” models (restricted for different age, stage, morphology, and diagnosis period) (table 6)⇓. The association between increasing deprivation and decreasing frequency of use of either treatment was significant in 25 of the 28 models (in 15 at P<0.001, in five at P<0.01, and in five at P<0.05). All three non-significant values related to the analysis of the subgroup of patients for whom we had information on stage, suggesting loss of power rather than difference in effect size. In other words, stage for stage and age for age, more deprived men were less likely to receive either of the two treatments, independently of diagnosis period and morphology.
Odds ratios* (change in probability of treatment use when moving from deprivation group to one immediately more deprived) of radiotherapy and surgery in men with prostate cancer, with analysis restricted (stratified) by diagnosis period, stage, age, and morphology
Discussion
Having adjusted for potential socioeconomic differences in age, diagnosis period, tumour type, and stage, we found substantial socioeconomic gradients in use of either radiotherapy or surgery for men with prostate cancer. In supplementary analyses, we further examined the robustness of the observed socioeconomic differences in treatment patterns by taking into account clustering of patients or treatment patterns in different hospitals; by restricting the analysis to patients for whom we had information on stage; and by stratifying the analysis to patients of different age, stage, diagnosis period, and tumour type. All the above analyses strongly indicated that, on average, more deprived patients were less likely to undergo surgery or receive radiotherapy in most hospitals and at any age, any stage, with any morphology, and during any study period. There was increasing use of surgery over time. This probably represents changes during the study period in availability of surgical expertise, criteria for selecting patients, or patients’ preferences for surgery.
Strengths
We used a large population based sample of observations covering a relatively long and recent time period. In addition, we had high quality information on stage for a substantial proportion of patients, and we have accounted for potential case mix or variation in clinical practice between different hospitals. Our findings indicate that stage at diagnosis does not explain the observed socioeconomic differences in management and, similarly, that variation between hospitals is also unlikely to explain such differences.
Comparisons with other studies
We are not aware of other research examining socioeconomic differences in treatment for prostate cancer that examines potential clustering at the level of hospital of diagnosis using multilevel modelling. A recent UK study also reported higher frequency of surgery and radiotherapy in least deprived patients but did not include information on stage at diagnosis.20 Studies from Australia also indicated that socioeconomically disadvantaged patients were less likely to undergo radical prostatectomy but did not encompass potential differences in use of radiotherapy (the other main treatment).21 22 As in research from the United States,19 we observed an association between lower socioeconomic status and less frequent use of surgery or radiotherapy. Just over a quarter of all patients who underwent radical prostatectomy in our study had stage III disease. This most probably reflects “upstaging” of patients with clinical stage II disease who were found to have stage III disease at histopathological examination after radical prostatectomy. Similar or slightly higher (compared with those found in our study) percentages of patients with stage III disease among hospital series of patients undergoing radical prostatectomy have been reported both in the US23 24 and the UK.25
Limitations
Although our lack of information on comorbidity is a limitation, we would have expected this to negatively influence eligibility for surgery and not radiotherapy (which presents no operative risk per se). In fact, among patients with prostate cancer managed with active treatment, greater comorbidity (which could have been expected to be associated with higher deprivation) predicts higher use of radiotherapy.26 The fact that socioeconomic differences in use of either surgery or radiotherapy are similar makes it unlikely that observed differences in use of surgery are simply a consequence of socioeconomic differences in comorbidity. In our study population radiotherapy was more common than surgery use at a ratio of between 5:1 to 3:1, earlier and later in the study, respectively (this is markedly different than in the US and most European countries).19 26 27 Therefore the observed socioeconomic treatment patterning mostly relates to differential use of radiotherapy. Nevertheless, comorbidity might influence decision making about any active management treatment option because oncologists and surgeons would normally advise radical treatments only in patients with a reasonable life expectancy, when the likely benefits of such treatments outweigh the side effects that reduce quality of life.28 More research on how comorbidity status influences decision making in the management of early stage prostate cancer would be welcome.
Potential time trends in ascertainment of treatment status could have biased the findings, but such trends are unlikely. If there were secular trends in ascertainment of treatment status they would have affected surgery and radiotherapy similarly, whereas substantial increasing trends in use were observed only for surgery. Misclassification of treatment status per se is another source of potential error. Such misclassification, however, is unlikely to have been different between deprivation groups,29 and, if present, it would have made treatment patterns between different groups more similar and would have therefore made any true differences in treatment use between different deprivation groups even smaller than those observed. A small proportion of patients treated with radiotherapy were treated with brachytherapy (<1.5% of all patients and <6% of all patients treated with radiotherapy), but this cannot explain the observed socioeconomic differences in radiotherapy, as confirmed by sensitivity analysis (data not shown). We had no data on use of high intensity focused ultrasound or cryotherapy, but the use of these procedures, even recently, seems to be rare30 and would have been even rarer during most of the study years (1995-2006).
Although we had no information on stage for a substantial subset of patients, this limitation has to be seen in the context of the study’s population based design and period. In addition, deprivation differences in surgery or radiotherapy persisted (and were nearly the same) when we restricted analysis to patients with information on stage. Given the findings, it is highly improbable that deprivation differences in the management of patients without stage information would have been any different to those observed for “all” as well as “staged” patients. The fact that deprivation status was not a predictor of stage ascertainment makes such a hypothesis even less probable.
We had no data on ethnic group, which might in principle be a confounder of socioeconomic status.19 31 High quality demographic data, however, indicate that the proportion of individuals belonging to ethnic minorities in the geographically defined population of this study was relatively small during the study period. In the 2001 census (near to the study period midpoint) only 1.7% of men aged over 65 in the East of England Government Office region belonged to a minority ethnic group,32 and of those, only 0.5% were black or black British, a population group known to have a higher than average incidence of prostate cancer.33 Therefore the observed socioeconomic differences in treatment reflect socioeconomic treatment patterning among mainly white patients.
We acknowledge that we did not have information about other dimensions of management, beyond surgery or radiotherapy per se (for example, activity volume for individual surgeons,34 radiotherapy dose and fractionation, and patients’ experience). Therefore socioeconomic differences in management might be only partially depicted.
Socioeconomic status can be measured directly by measuring a person’s income, occupation, or education or indirectly by using area based measures of the characteristics of the population of a small area.35 We used an area based measurement, in common with previous authoritative UK research.4 5 In different countries, a valid association between area based socioeconomic status and health outcomes has been established in the past two decades.36 37 Evidence suggests that both area based and individually measured socioeconomic status are independently associated with health outcomes.38 39 40 Individual measures of socioeconomic status also have limitations,41 and might be affected by lack of homogeneity within strata (such as social class or income or education bands).36 Using an area based indicator of socioeconomic status might either underestimate or overestimate socioeconomic gradients compared with individual measures, contextually, for different cancers and indicators.41 Our area based measures were small and relatively highly homogeneous (lower super output area), which substantially improves the methods.17
Research and policy implications
Whether observed differences in deprivation in use of surgery and radiotherapy confer a survival advantage to more affluent groups is debatable.8 Such an effect is possible, given some evidence that radical treatment with either surgery or radiotherapy might confer a survival advantage.42 43 It is also likely, however, that some of the observed more frequent use of radical treatment in more affluent patients might not confer any survival advantage if it relates to relatively less aggressive tumours. Furthermore, the observed socioeconomic differences in treatment might reflect true socioeconomic differences in patients’ making a positive choice for either radical or non-radical treatments or socioeconomic differences in patient-clinician interactions about management. Patients of different socioeconomic status might have different attitudes to accepting the risks associated with radical treatments.28 Decision making for treatment of prostate cancer is known to be complex44 and at least in part patterned by the patient’s lifestyle, educational, and demographic factors (such as ethnicity).45 46 47 48 Exploration of such hypotheses through qualitative research might be warranted.19 Given these uncertainties, the observed differences in treatment patterns cannot a priori be assumed to indicate differences in treatment quality.
What is already known on this topic
Optimal management of men with early prostate cancer is uncertain, and this might give rise to differential treatment patterns among different groups of patients
Socioeconomic inequalities in relative survival from prostate cancer are known to exist, but the extent to which they relate to potential differences in treatment is unknown
What this study adds
The use of either radiotherapy or surgery (prostatectomy) was lower among men with prostate cancer from lower socioeconomic groups
Socioeconomic differences in radiotherapy or surgery persisted even when factors such as hospital of diagnosis and disease stage were taken into consideration
Notes
Cite this as: BMJ 2010;340:c1928
Footnotes
We thank Clement Brown, medical director, Eastern Cancer Registration and Information Centre (ECRIC), for his work relating to staging of cases, and all ECRIC staff; Chris Palmer, Centre for Applied Medical Statistics, Department of Public Health and Primary Care, University of Cambridge, for commenting and advising on aspects of the statistical analysis; and the four peer reviewers for their constructive comments.
Contributors: GL conceived the study hypothesis and its design, with contributions from all other authors. DCG and KAW provided and quality assured data. JMB collected data. JMB and GL analysed data, with commentary and interpretation support from DEN, DCG, and KAW. Information about staging directly relates to the work of Clement Brown, medical director, Eastern Cancer Registration and Information Centre (ECRIC). All authors contributed and commented on the manuscript. GL is guarantor.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) (URL) and declare that all authors had: (1) No financial support for the submitted work from anyone other than their employer; (2) No financial relationships with commercial entities that might have an interest in the submitted work; (3) No spouses, partners, or children with relationships with commercial entities that might have an interest in the submitted work; (4) No Non-financial interests that may be relevant to the submitted work.
Ethics approval: Not required.
Data sharing: For data sharing requests please contact the corresponding author at gl290@medschl.cam.ac.uk. As was the case in this study, cancer registries in the UK have policies that permit the release of anonymised (non-identifiable and non-disclosive) data to researchers, with the aim of generating evidence that can be of use to improving patient care. More information about the regulatory environment underpinning the function of UK Cancer Registries can be found at the UK Association of Cancer Registries website http://82.110.76.19/ .
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.