Article Text

Abstract
Context A significant proportion of smokers who quit do so on their own without formal help (ie, without professionally or pharmacologically mediated assistance), yet research into how smokers quit focuses primarily on assisted methods of cessation.
Objective The aim of the present work was to systematically review recent smoking cessation research in Australia, a nation advanced in tobacco control, to determine what is known about smokers who quit unassisted in order to (1) inform a research agenda to develop greater understanding of the many smokers who quit unassisted and (2) elucidate possible lessons for policy and mass communication about cessation.
Methods In January 2013, four e-databases and the grey literature were searched for articles published between 2005 and 2012 on smoking cessation in Australia. Articles focusing solely on interventions designed to stimulate cessation were excluded, as were articles focusing solely on assisted cessation, leaving articles reporting on smokers who quit unassisted. Data from articles reporting on unassisted cessation were extracted and grouped into related categories.
Results A total of 248 articles reported on smoking cessation, of which 63 focused solely on interventions designed to stimulate cessation, leaving 185 reporting on the method of cessation (‘how’ a smoker quits). Of these, 166 focused solely on assisted cessation, leaving 19 reporting, either directly or indirectly, on smokers who quit unassisted. Data from these studies indicated 54% to 69% of ex-smokers quit unassisted and 41% to 58% of current smokers had attempted to quit unassisted.
Conclusions The majority of Australian smokers quit or attempt to quit unassisted, yet little research has been dedicated to understanding this process. Almost all research that reported unassisted cessation referenced it as a comparator to the focal point of assisted cessation. Public health may benefit from insights gained from greater research into the cessation method used by most smokers. Suggestions and a rationale for such research are provided.
- Cessation
- Addiction
- Global health
Statistics from Altmetric.com
Introduction
Australia is a nation advanced in global tobacco control. Supportive government policies over several decades and a robust research track record have provided global intelligence to the wider tobacco control community about the introduction and impact of a wide range of vanguard policies and interventions.1 Adult and youth smoking prevalence figures are at record lows in Australia: in 2011–2012, the prevalence of daily smoking was 15.7% among those aged 15 years or older and 4.4% among those aged 15–17 years.2 This compares with 24.3% in 1991 for those aged 14 years or older.3
Australia is committed to reducing prevalence still further, and in 2008 set the ambitious goal of 10% prevalence of daily smoking among people aged 14 years or older by 2020.4 However, based on existing trends in uptake and cessation in Australia, Gartner and colleagues calculated that even if smoking uptake continues to decline at the current rate, prevalence will not drop to 10% until 2028. They concluded the only way to reach this goal would be to double the current cessation rate.5
Paradoxically, despite significant declines in smoking uptake and prevalence, population cessation rates have stalled in Australia3 ,5 and comparable nations.6–8 In Australia this stalling of cessation has coincided with unprecedented investment in evidence-based cessation support, including more accessible and affordable pharmacotherapy (eg, over-the-counter nicotine replacement therapy (OTC NRT) in 1997, and subsidised prescribed bupropion, varenicline and NRT in 2001, 2008 and 2011, respectively) and improved support services (extended quitline services and general practitioner (GP) involvement in supporting cessation),1 all within a tobacco-control framework committed to denormalising smoking.9
The efficacy of professionally and pharmacologically mediated cessation assistance and the ability of assistance to improve cessation rates have been extensively documented.10–12 Yet no satisfactory explanation exists for the stalled population cessation rates in the face of access to such efficacious support. The ‘hardening hypothesis’—that the group of smokers remaining as smoking prevalence declines is more addicted and less willing to quit—has not been supported in the available evidence from national datasets.13 To date discussion has centred around the efficacy versus effectiveness debate6 ,14 and the role that bias (recall, selection and Hawthorne effects) and confounding have in explaining why results obtained in randomised controlled trials may not generalise to ‘real-world’ cessation.15–17 Others emphasise it as a problem of reach or dissemination, with the solution being facilitating even greater access to assistance, or of a need to promote greater smoker knowledge about the benefits of professionally or pharmacologically mediated cessation.18 ,19 Nonetheless, smokers in Australia report high levels of awareness of quitlines and smoking cessation aids,20 and NRT, bupropion and varenicline are all subsidised by the government, casting into doubt the potential for increased promotion to increase rates of use. Further, concern has been raised by some that the widespread marketing of pharmacological cessation aids might undermine smokers’ self-efficacy7 and provide smokers with a ‘get-out-of-jail-free card’ as opposed to focusing on the need to persevere in the quit attempt.6
Increasing the rates of cessation is widely considered to be challenging and invites consideration of increased21 and more finely tuned efforts but, given the suboptimal impact of existing strategies on cessation, of also exploring hitherto under-researched possibilities.22 One of these is to better understand the motivations and cessation experiences of the many smokers who have successfully quit on their own without professionally or pharmacologically mediated assistance in anticipation of information that may be instructive to promoting increased cessation in general.
Despite the persistence of this universal phenomenon, we know little about the many who quit this way, their tobacco use histories, their previous quit attempts, why they eschewed assistance, whether their quitting motivations are any different from those using assistance, whether they have different exposure to environments conducive to cessation and relapse prevention, and whether they use any characteristic narratives or heuristics to describe or make sense of their decision to quit on their own without professionally or pharmacologically mediated assistance. Importantly, smoking cessation is frequently framed in public discourse as being very difficult, with a high probability of relapse and a process that should sensibly involve medication and professional supervision.23–27 The dominance of this discourse may contribute to expectancy or nocebo effects among smokers about the likely difficulty of quitting which may condition their experience of trying to quit. The large numbers of ex-smokers who quit on their own without professionally or pharmacologically mediated assistance provide a potentially important study population whose experiences might be instructive in changing some aspects of the ways in which public health campaigns and health professionals talk about cessation to smokers. Such information may be useful to those concerned to promote higher usage of evidence-based medications, by providing insights into barriers to use. Equally, it may provide important insights into how successful ex-smokers who quit on their own without professionally or pharmacologically mediated assistance approached their decision to quit and self-management strategies used during and after cessation.
Throughout this review, we refer to those smokers who quit on their own without professionally or pharmacologically mediated assistance as having quit ‘unassisted’. Since the early 1970s, Australia has seen high-profile tobacco control policy debates, public awareness campaigns and policy implementation across all areas of comprehensive tobacco control. All of these factors have acted synergistically to foment a social climate designed to motivate smoking cessation. These factors stimulate quit attempts21 and, in the broadest sense of the word, might be said to ‘assist’ cessation in that they provide a supportive environment. Together they are relevant to understanding why smokers quit, that is, what motivates a smoker to quit. In contrast, the focus of this current study is on the method used to quit, that is, the how of successful cessation, of what is known about Australian smokers who successfully quit unassisted, and the research gaps that may be instructive areas of inquiry to cessation in general.
Methods
Data sources and study selection
In January 2013, two review authors searched MEDLINE, PreMEDLINE and PsycINFO via OVIDSP, and CINAHL via EBSCO for articles published between January 2005 and December 2012 on smoking cessation in Australia. Data from articles published prior to 2005 were unlikely to be relevant to future campaign planning or policy decisions given the speed with which the social climate surrounding smoking has changed in Australia. The reporting of this review is in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.28
Articles were identified through use of free text and indexed terms, including ‘tobacco use cessation’, ‘smoking cessation’, ‘quit’, ‘smoking’ and ‘Australia’.29 Additional sources of smoking cessation data (from the grey research literature) were identified by searching relevant government and non-government websites including those of the Australian Bureau of Statistics, Australian Institute of Health and Welfare, Cancer Council Victoria, and Cancer Institute New South Wales (NSW) (see online supplementary file 1). If required, contact was made with authors of the original studies to acquire additional information relating to the study methods and/or results.
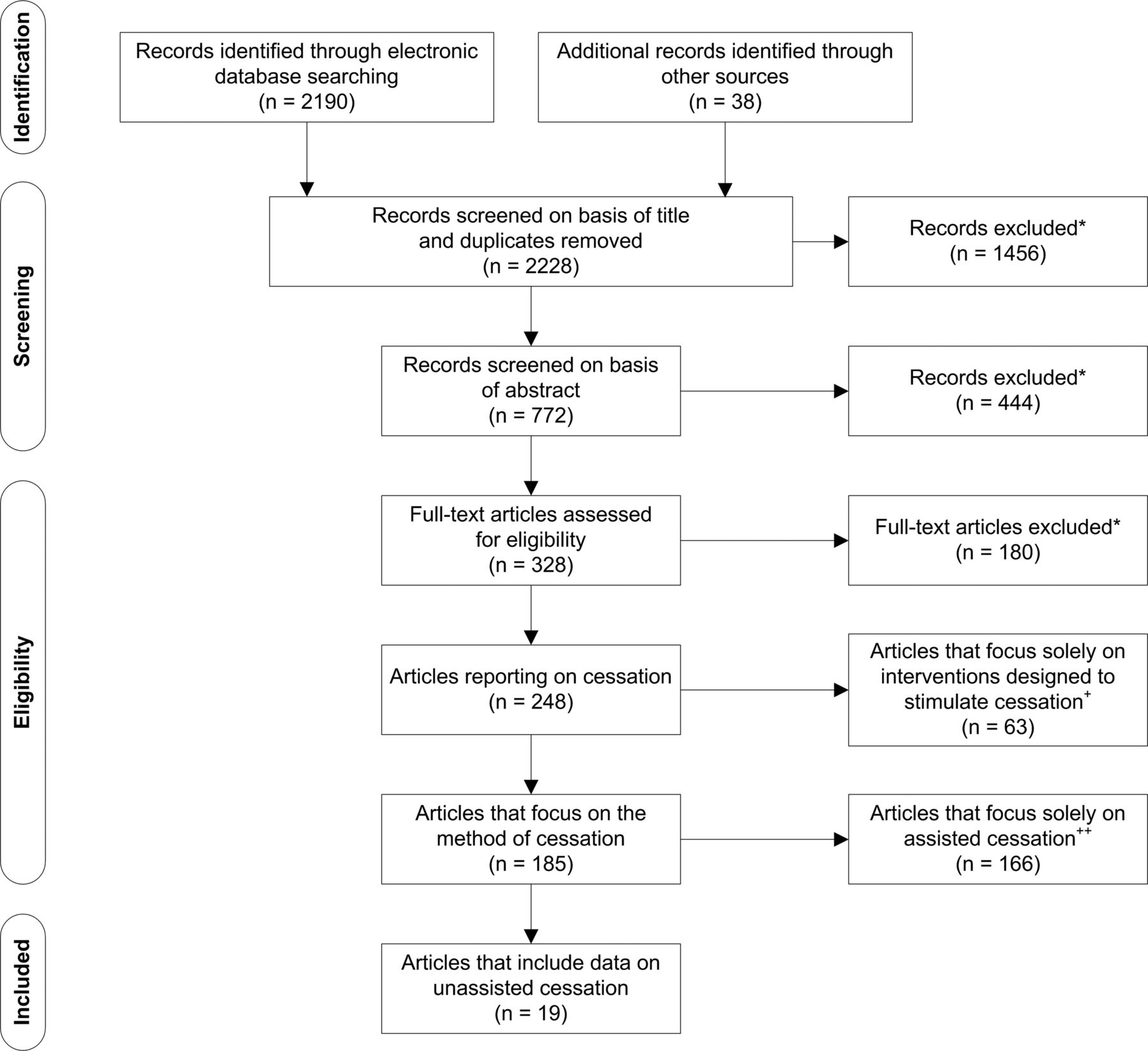
One author identified, selected and assessed the studies for eligibility, and a second author independently checked a subsample. To be included, studies had to contain original quantitative or qualitative research data on smoking cessation within the Australian population (and/or relevant subpopulations).29 Once identified, articles were screened for data on unassisted cessation. Articles were eliminated if they focused solely on interventions designed to stimulate cessation (ie, did not report on methods of quitting at all) or if they focused solely on assisted cessation (figure 1 and see online supplementary file 2, ‘Selection criteria’).
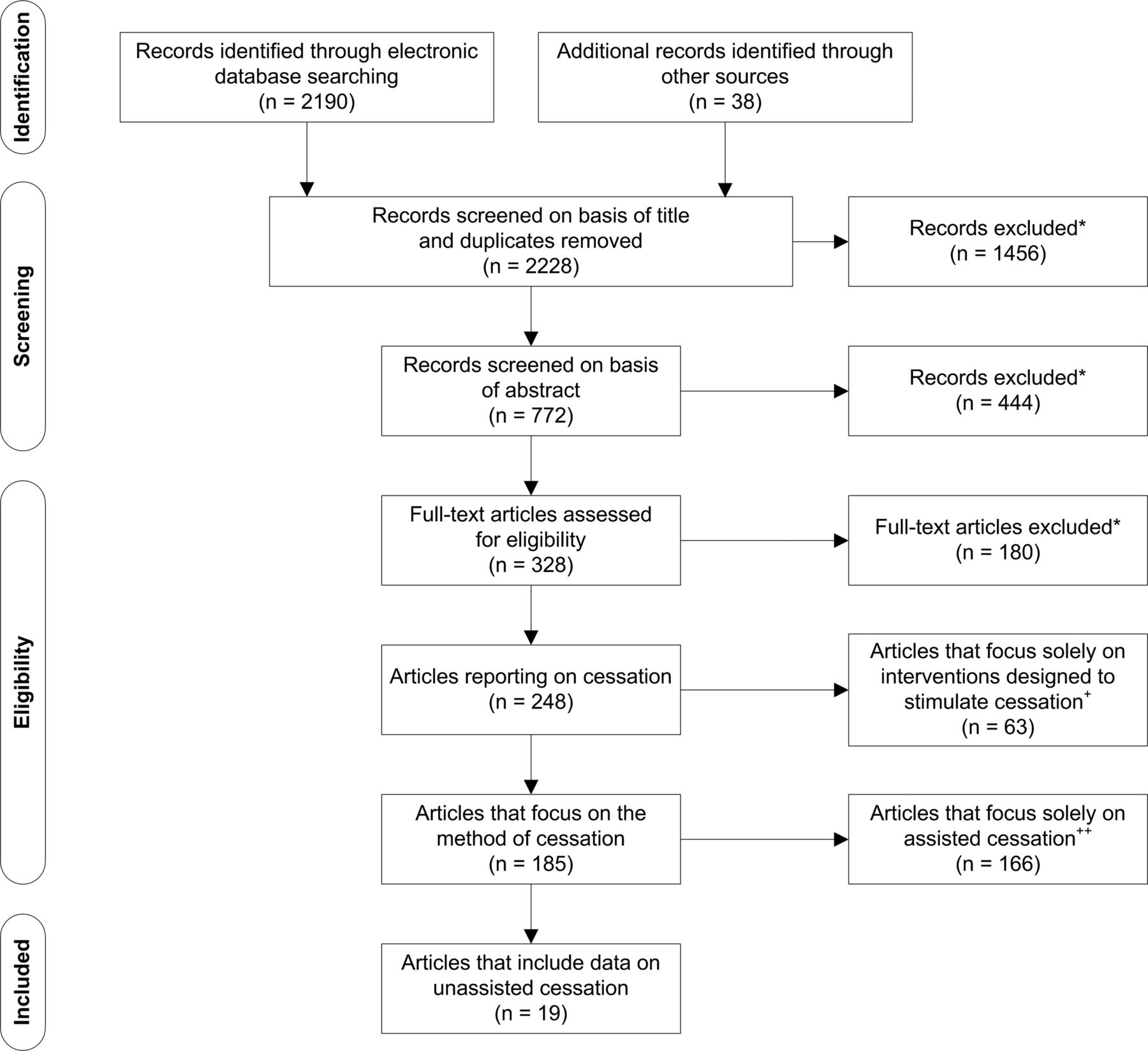
Identification, screening, eligibility and selection of articles retrieved from the literature search, January 2013. *Reasons for exclusion included reviews, study protocols, commentaries; studies of smoking status and health (eg, as a risk factor or predictor of disease); effects on behavioural or cognitive or affective variables, social disadvantage or social and economic status; methodological research; health economics or cost-effectiveness studies; interventions to prevent uptake; trends, correlates or predictors of uptake; development of clinical guidelines or adherence to guidelines; impact on environmental tobacco smoke; genetics; harm reduction; tobacco consumption trends and monitoring; bibliometrics; nicotine replacement therapy adverse effects.29 +Interventions designed to stimulate cessation included mass-media campaigns, health warnings, smokefree policies, price increases (tax) and retail regulation. ++Assisted cessation included pharmacotherapy (nicotine replacement therapy, bupropion and varenicline), behavioural counselling, and complementary and alternative therapies (eg, hypnosis and acupuncture).
Defining unassisted cessation
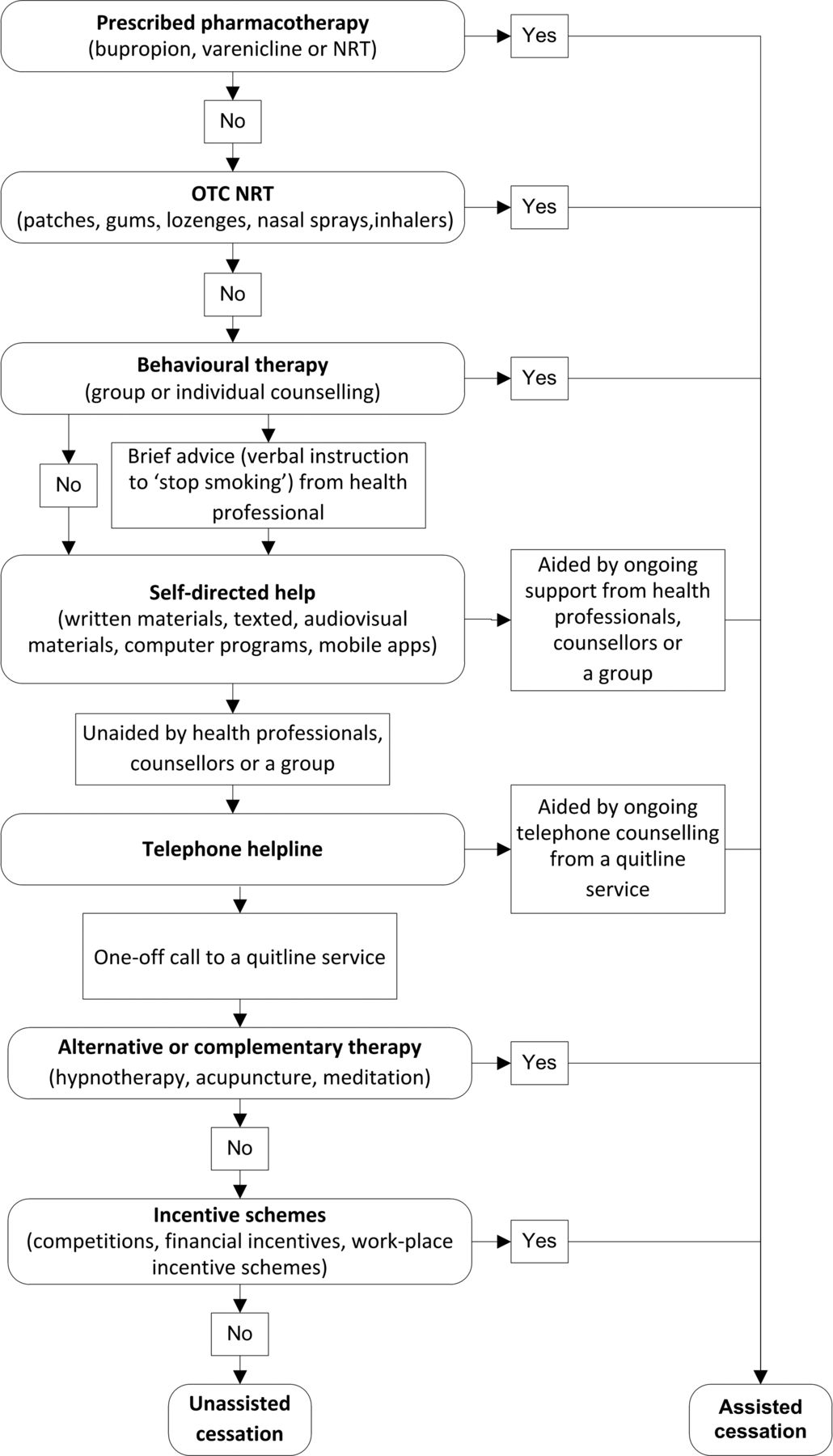
We were interested in identifying studies that reported on smokers who quit on their own without formal assistance, be it professionally or pharmacologically mediated assistance. By formal assistance, we are referring to quitting methods that have been ‘opted in’ by the smoker and that provide assistance on more than a one-off basis. All of the included studies agreed that use of NRT or stop-smoking medications constituted assistance; however, studies differed in whether or not they classified brief advice from a health professional, use of self-help materials, ever calling the a quitline service, or seeking information on the internet as assistance.30–32 In addition, several studies used ‘cold turkey’ to refer to quitting abruptly without professionally or pharmacologically mediated assistance33–36 but the term was also used to refer to quitting abruptly with professionally or pharmacologically mediated assistance.36 A standard definition of unassisted cessation was required with which we could assess every study for eligibility (figure 2). The rationale for the definitions adopted for assisted and unassisted cessation was that it reflected the stance taken by the Cochrane Collaboration, whose reviews of smoking cessation interventions differentiate between quit attempts that are formally supported by the ongoing help of a health professional or counsellor and those that are not.11 ,12 ,37–42 Our definition of ‘unassisted’ cessation therefore included, for example, smokers who received brief advice or who called a quitline but who did not receive ongoing support from a GP or counsellor.
{kind=link}
{kind=link}
Data extraction and synthesis
After screening for eligibility, data on unassisted cessation were extracted using a template pilot tested on a sample of 60 studies drawn from a literature search run during the scoping stages of the systematic review process. Data were extracted by one author and independently checked by the other two authors. Any disagreement relating to data extraction was resolved through discussion among all three review authors. If agreement could not be reached, or if further information was required, the authors of the original study were contacted for clarification. Seven authors were contacted for further information or for data clarification. Five responded: two provided clarification of the study period,43 ,44 one provided clarification of the location of the study,35 one provided clarification of data reported in a figure30 and one provided additional data not reported in the original reports.20 ,45 Data extraction was followed by collation and sorting by theme. In addition, funding source was noted.
Results
Cessation research in Australia
In total, 2228 studies were identified: 2190 from the electronic databases and 38 from the grey literature, of which 248 met the inclusion criteria. Of the 248 articles reporting on cessation, 63 focused solely on interventions designed to stimulate cessation; this left 185 articles that focused on the method used to quit. Of these, 166 focused solely on assisted cessation, leaving 19 articles that reported data, either directly or indirectly, on unassisted cessation (figure 1). The data on unassisted cessation fell into three categories: the proportion of smokers who quit unassisted; characteristics of smokers who quit unassisted; and beliefs and attitudes about quitting unassisted (table 1).
Summary of the 19 studies reporting data on unassisted cessation
Funding
Of the 248 articles reporting on cessation, 189 were funded by government or not-for-profit organisations, 4 by pharmaceutical companies, 4 by both a government or not-for-profit organisation and a commercial organisation (3 received free or subsidised NRT from a pharmaceutical company), and 55 did not specify funding source. Of the 19 reporting on unassisted cessation, 17 were funded by government or not-for-profit organisations; 2 did not specify funding source.
Proportion of smokers and ex-smokers who quit unassisted
In all, 14 studies (11 quantitative and 3 qualitative) reported on the number or proportion of smokers who quit unassisted. The 11 quantitative studies reported that between 54% and 78% of ex-smokers quit unassisted, and between 41% and 82% of current smokers had attempted to quit unassisted (table 2).17 ,30–32 ,34 ,43–48 Of the studies with representative rather than convenience samples, between 54% and 69% of ex-smokers quit unassisted and between 41% and 58% of current smokers had attempted to quit unassisted.
Proportion of smokers and ex-smokers who quit or attempted to quit unassisted, as reported in Australian studies published January 2005 to December 2012
The three qualitative studies reported data from focus groups or in-depth interviews. A series of 21 focus groups with smokers and 5 focus groups with ex-smokers across 4 states in Australia in 2010 reported ‘Most smokers who quit for any length of time did so cold turkey with only some acknowledging the use of support aids’.33 A Tasmanian study comprising in-depth interviews with ex-smokers (n=14) and current smokers (n=21) in 2006–2008 reported, ‘Many just decided to quit and did so without advice, NRT or medication’.35 Additionally, a series of in-depth interviews with Aboriginal and Torres Strait Islander ex-smokers (n=20) in Queensland reported, ‘Most participants quit smoking without using smoking cessation aids such as NRT, or varenicline, and in fact even among those who did use quit counselling services, NRT or varenicline, not one participant completed the full recommended 12-week programme’.49
Two of the quantitative studies compared rates of successful cessation for smokers who used assisted and unassisted methods of quitting.17 ,34 The Australia-wide 2003–2004 Bettering the Evaluation and Care of Health (BEACH) study of patients attending general practices reported a success rate (the number of former smokers divided by the total number attempting to quit for each cessation method) for smokers who quit cold turkey (defined as ‘immediate cessation with no method of assistance’) of 40% compared with 21% for bupropion and 20% for NRT for quit attempts since February 2001 (n=1030).34 A possible limitation of this study is that smokers using pharmacotherapy may have been more addicted than smokers who quit cold turkey.
An International Tobacco Control (ITC) 4-Country study (which included an Australian arm) compared rates of successful cessation for individuals using or not using stop-smoking medications (varenicline, bupropion, NRT gum/oral NRT, or NRT patches).17 Although the study did not differentiate between those quitting unassisted and those quitting with behavioural support, the results provide an indication of the success rate for unassisted cessation, given that the proportion of smokers who use behavioural assistance in Australia is relatively small.31 The study reported that, of those who smoked 10+ cigarettes per day and quit without medication, 21% were abstinent at 1 month and 14% at 6 months, compared with smokers who quit with medication, of whom 24% were abstinent at 1 month and 16% at 6 months (n=5157 for 1-month abstinence data and n=4792 for 6-month abstinence data). After controlling for differential recall bias, of those who quit without medication, 12% were abstinent at 1 month and 5% were abstinent at 6 months, compared with smokers who quit with medication, of whom 23% were abstinent at 1 month and 14% were abstinent at 6 months (n=511 for 1-month abstinence data and n=504 for 6-month abstinence data).
Trends in proportion of smokers and ex-smokers who quit unassisted
The Cancer Institute NSW Smoking and Health Surveys and a 2011 ITC study indicate that the proportion of smokers and ex-smokers quitting or attempting to quit unassisted is falling.20 ,31 ,45 In NSW, the proportion of smokers and ex-smokers who quit or attempted to quit cold turkey (defined as no aids, including NRT, how to quit or self-help materials, consulting a GP, advice from health professional, pharmacist or dentist, prescribed medication, using a quitline service, natural or alternative therapy, online quit smoking info, online quit smoking programme) on their most recent quit attempt fell from 68% to 55% between 2005 and 2012.20 ,45 The ITC study reported that in Australia the proportion of smokers and ex-smokers who quit or attempt to quit without ‘help’ (help being use of NRT products, varenicline or bupropion, advice or information about quitting smoking from a quitline service, the internet, or a local stop-smoking service or specialists) fell from 63% in 2002 to 2003 to 41% in 2008–2009.31
Characteristics of smokers who quit unassisted
Six studies provided data on various characteristics of those quitting without assistance.16 ,17 ,32 ,33 ,36 ,50 The Cancer Institute NSW Tobacco Tracking Surveys 2007–2009 reported that younger smokers were more likely to use unaided methods such as cold turkey, and older or less-educated smokers were more likely to use aided methods (defined as prescribed medication, NRT products, advice from health professional or quitline service, natural therapies, self-help materials).32 A 2010 qualitative study by the Department of Health and Ageing involving 26 focus groups across 4 states reported younger smokers were more likely to have only tried to quit ‘cold turkey’ (defined as ‘without use of quitting aids’).33
Two ITC studies, although not reporting specifically on unassisted cessation (unassisted cessation being the comparator group rather than the focus of the study), provided data on the profile of smokers who quit without assistance. These ITC studies reported that Australian smokers who did not use any medication (varenicline, bupropion, NRT gum, oral NRT or NRT patches) tended to be male, to be younger, to be racial/ethnic minorities, to have lower incomes, to be less heavily addicted to nicotine and to have higher self-efficacy compared with those who attempted to quit with medication, and, predictably, to disagree with the statement ‘Stop-smoking medications make it easier to quit’.16 ,17
Two further ITC studies which reported on abrupt versus gradual quitting also provided an indication as to which smokers were more likely to have quit unassisted. The first reported that smokers who did not use assistance (defined as stop-smoking medications or a quitline service) were more likely to quit abruptly than smokers who did use assistance;50 the second showed that in smokers who quit unassisted (defined as quitting without NRT products or prescribed medications), abrupt quitting lead to better outcomes in terms of quit rate and relapse prevention than gradual quitting.36
Attitudes and beliefs about quitting unassisted
Five studies reported on attitudes and beliefs about unassisted cessation.32 ,35 ,49 ,51 ,52 A study using the Cancer Institute NSW Tobacco Tracking Survey data explored the perceived effectiveness of various quitting aids (defined as prescribed medication, NRT products, advice from health professional or quitline service, natural therapies, self-help materials) from the perspective of the recent ex-smoker.32 Between 2007 and 2009, ex-smokers who had quit in the past 12 months (n=1097) were asked to rate how helpful they had found various cessation methods (used on any quit attempt, not just their last successful quit attempt). In addition to being the most widely used method of cessation (69% of recent quitters had used unassisted cessation in the previous 12 months), ‘cold turkey’ (defined as no quitting aids, including prescribed medication, NRT products, advice from health professional or quitline service, online quit info or quit programme, natural therapies, self-help materials) was perceived as being the most helpful method of cessation. As the recent quitters were able to nominate multiple methods used either at the same time or over the course of many quit attempts, the measure of perceived helpfulness allowed quitters to distinguish between methods they believed had helped them and those that had not.32
The concept of cessation aids ‘being a sign of weakness’ was mentioned by several,35 ,49 and explored extensively in the 2008 ITC study of Australian smokers and recent quitters.51 The study reported 35% of smokers and ex-smokers (ranging from 42.2% for those who were not considering quitting to 21.4% for recent quitters) believed using aids was a sign of weakness. Younger and less-well-educated smokers and ex-smokers were more likely to believe use of aids was a sign of weakness. Males and those who smoked fewer cigarettes per day were also more likely to agree that aids were a sign of weakness. Believing that use of aids was a sign of weakness was related to holding ‘sceptical’ beliefs about smoking and health risk and believing that smoking was ‘worth it’ (ie, worth the risk). Bond found that those who quit without using smoking cessation aids or support were more likely than those who used cessation aids or support to believe that use of aids was ‘evidence of lack of will power’.49 Jamrozik reported that smokers, those aged 50 years or over, those who were retired, or whose highest level of education attained was completing Year 10 (ie, leaving school aged 16) were more likely to agree with the statement ‘I couldn't quit without using a product such as patches, gum, prescription etc.’.52
Discussion
Australian cessation research has little to report about unassisted cessation. On the whole, unassisted cessation is seldom mentioned and inconsistently defined and, when it is referenced, it is usually in terms of what it is not (typically ‘non-medical’ or ‘non-pharmacotherapy’). It is considered to be the absence of an intervention rather than a phenomenon in its own right. This focus on assisted cessation aligns with the research priorities of the smoking cessation community worldwide.22
Unassisted cessation used to be more favourably viewed and more widely researched,53 ,54 but with the introduction of nicotine chewing gum in the 1980s and nicotine replacement patches in the 1990s it came under fire,55 perhaps fuelled by the growing speculation that NRT would significantly improve cessation rates.56 ,57 Yet the Australian data reported in this current review confirm that nearly 20 years after the introduction of pharmacotherapy in Australia, the majority of Australian ex-smokers (‘all’ ex-smokers as well as ‘recent’ ex-smokers) who successfully quit or current smokers who attempt to quit do so unassisted, mirroring that which has been reported in comparable countries such as the USA58–61 and, until recently, the UK.62
Although still the method used by the majority of smokers and ex-smokers, recent data indicate that the proportion who quit unassisted may be declining. This shift towards assisted cessation may be real, or may be an artefact of survey data collection and reporting. The Cancer Institute NSW Smoking and Health Surveys include consulting a GP (9% in 2005 compared with 19% in 2009) and receiving advice from other health professionals (2% in 2006 compared with 12% in 2009) as assistance,20 which many smokers would consider to be what motivated or contributed to them making a quit attempt (the ‘why’) rather than the method they used to quit (the ‘how’); similarly, Cooper's 2011 ITC study classified receiving any advice or information about quitting from a Quitline or the internet as assistance.31
The high proportion of current smokers30 ,34 ,43–48 who had used unassisted cessation when they attempted to quit could be interpreted as evidence of the failure of unassisted cessation as a method of quitting. However, the similarly high use of unassisted cessation as a method of quitting among ex-smokers17 ,32 ,34 ,43–45 counterbalances that evidence, especially as five of these six studies reported on the method used on the final, successful quit attempt,17 ,34 ,43–45 when differential recall bias has no effect.16 Controlling for recall bias appears to indicate that quit attempts with medication or NRT are more effective than quitting unassisted. In contrast, a NSW study found recent ex-smokers perceived cold turkey to be the most effective method of quitting.32 Continued population-level research into the effectiveness of assisted versus unassisted methods is required. Nonetheless, this review provides evidence that, regardless of the relative success of those who quit assisted and unassisted, there is large proportion of smokers who choose not to use formal assistance in the face of large-scale promotion and widespread availability.
Given its enduring popularity, these findings invite the question, ‘Why is there so little research into unassisted cessation?’ And why, when it is talked about is it often disparagingly,15 ,63 ,64 as illustrated in the 2012 stop-smoking campaign promoted by a number of English National Health Service Trusts entitled ‘Don't go cold turkey’,23–27 which ran in several areas alongside Pfizer's campaign bearing the same name.65 ,66
Possible explanations include the dominance of experimental evidence in evidence hierarchies,67 ,68 the power of evidence-based medicine to inform national and international policy agendas,68–70 and the increasing commodification and medicalisation of smoking cessation by the pharmaceutical industry and health professionals.71 ,72 The cessation research agenda globally and in Australia has, perhaps understandably given the long-held belief that a medical or professionally mediated solution would provide the answer to cessation, been shaped first by a desire to assess the efficacy and effectiveness of assisted cessation, and secondly by the goal of extending the reach and uptake of assisted cessation to as many smokers as possible. The failure of these efforts to generate the anticipated population effect is viewed by many as a problem that lies with the smoker's failure to use ‘evidence-based’ methods to quit43 ,73 rather than any failure or problem of enduring consumer acceptability with the methods of cessation being advocated. Despite considerable and continuing efforts invested in creating effective interventions and in encouraging the majority of smokers to use them, their impact on population cessation rates in Australia, as elsewhere, has been less than expected.3 ,6–8
Future cessation research might benefit by considering other areas of addiction research74 ,75 where quitting without formal help, or the phenomenon of natural recovery or self-change,76 ,77 is widely acknowledged and overtreatment questioned.78 There are far more ex-smokers who have quit unassisted than smokers who quit using professionally or pharmacologically mediated assistance. This enduring and large-scale phenomenon remains largely neglected and the lived cessation experiences of these large numbers of ex-smokers deserve far greater research attention than has occurred. Our review reveals many potentially instructive questions that remain largely unexamined and that might yield useful insights to the planning of future cessation policy and research (box 1). Instead of perceiving unassisted cessation only as a problem, it might be wise to embrace it as an opportunity to discover possible implications for supporting the many smokers who remain uninterested in or resistant to using assistance when they attempt to quit. It would be surprising if the experiences of millions of ex-smokers around the world who have quit unassisted had little to offer those trying to motivate and support others to quit.
Potentially instructive research questions that the Australian research does not currently answer
-
Attitudes and beliefs
-
Why do so many smokers choose not to use assistance in the face of so much persuasion to do so?
-
Why do smokers who quit on their own perceive assisted cessation to be a sign of weakness?
-
Do ex-smokers inflate their own role in their quitting and downplay the role assistance played to their success?
-
What characterises smokers who want to quit on their own: is it that they want to quit without pharmacotherapy or without any form of help at all (including help from GPs, quitline services and stop-smoking clinics)?
-
Have smokers who quit unassisted tried assistance before and realised that motivation and determination are critically important components of quitting?
-
Experiences
-
How do those who quit unassisted find the experience in terms of its degree of difficulty?
-
How does the experience of quitting unassisted compare with a smoker's expectations?
-
Does the experience of quitting unassisted differ for those who are heavily addicted compared with less addicted smokers?
-
Does the current focus on use of medications to quit mislead smokers about how hard or easy it will be to quit?
-
Does marketing for pharmaceutical aids have any impact on smokers’ self-efficacy?
-
Have smokers who successfully quit unassisted previous experience of quitting with assistance? If so, how has this informed they unassisted quit attempt?
-
Processes
-
How do those who successfully quit unassisted actually go about doing so? Is their success linked to deliberate quitting strategies or lifestyle factors (such as exercise, prayer, meditation or diet) that are not used by those who quit with assistance?
-
Do successful unassisted quitters have common ‘meta-narratives’ or heuristics that they believe assisted their determination to quit and to not relapse?
-
Are there exogenous (environmental) or endogenous (psychological) factors that many successful unassisted quitters have found useful?
-
Is to possible to identify which smokers are likely to quit unassisted, and potentially put in place a spectrum of policy interventions for different types of smokers, which can more effectively and more efficiently help them quit earlier?
Limitations
Differences in the populations under study and in definitions used in each of the studies made direct comparisons across all studies difficult. These differences included: surveying current smokers who have attempted unsuccessfully to quit versus ex-smokers who successfully quit; the quit attempt under investigation (whether the study reported on assistance used on any previous quit attempt or specifically on the last or final quit attempt); the period being reported (lifetime quit attempts vs quit attempts in the last 12 months); and differing meanings ascribed to the terms ‘cold turkey’, ‘stopping abruptly’, ‘on own’, ‘assistance’ by the study investigators (and presumably their interpretation by study participants). Limitations noted in several of the studies included recall bias (unassisted attempts tend to be forgotten more readily than assisted attempts)16 and the inability of the survey questions to adequately capture the process of smoking cessation (such as the multiple quit attempts made by many smokers and the variety of methods that may have been used on different quit attempts).
Conclusions
The lack of research interest in unassisted cessation is unfortunate. This suggests a form of unreflective research hegemony that privileges knowledge from interventionism as being more ‘real’ or important than that derived from studying the natural history of the cessation process in populations as it so often occurs entirely independently of the influence of cessation ‘treatments’. Prochaska and colleagues drew similar conclusions almost 30 years ago: ‘In spite of the overwhelming preference for and preponderant use of informal self-quitting approaches, smoking cessation research continues to focus on formalised treatments’.79
Greater study of the unassisted cessation process may reveal important individual and social factors such as life course precursors, environmental events or triggers, characteristic personal narratives and heuristics that successful unassisted quitters acknowledge as important to their success. An awareness and understanding of these factors might be useful to public health practitioners trying to motivate quit attempts and support those making them.
What this paper adds
-
Australia, with its history of vanguard tobacco control policies and fearlessness in questioning established dogmas, was thought to be the ideal place to assess what is currently known about smokers who quit on their own without formal help.
-
Apart from confirming that the majority of Australian smokers do indeed quit on their own without formal help, we found little is known about this significant population and this potentially significant phenomenon.
-
A consequence of the neglect of research into unassisted cessation is the lack of discourse in relation to the potential contribution that unassisted cessation—when promoted alongside existing policy and treatment practices—might make in reducing smoking prevalence at the population level.
-
Given the important role that cessation plays in reducing prevalence, it is essential that we gain a greater understanding about how and why smokers quit on their own without formal help. Lessons learnt from such research are highly likely to be of direct relevance to policy and practice, particularly to informing mass media campaigns that reach all smokers, including those who might prefer to quit unassisted.
Acknowledgments
Many thanks to Becky Freeman for comments on an earlier version of this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online criteria
- Data supplement 2 - Online databases
Footnotes
-
Contributors SC conceived the idea for the review. ALS and SC planned the review. ALS and SC conducted the literature searches and identified studies to include in the review. ALS categorised the studies and extracted the data. SC and SMD checked extracted data and contributed to the interpretation of the results. ALS wrote the first draft. SC and SMD contributed to the content and edited the drafts of the manuscript. All authors gave final approval for the version to be published.
-
Funding National Health and Medical Research Council, grant number 1024459.
-
Competing interests ICMJE criteria for authorship read and met: ALS, SC and SMD.
-
Provenance and peer review Not commissioned; externally peer reviewed.