Article Text

Abstract
Objective Culture of percutaneous central venous line (PCVL) segments may assist the diagnosis of line colonisation and catheter-related sepsis (CRS). The authors aimed to determine if the diagnosis of CRS and colonisation of PCVLs in neonates is improved by the culture of the proximal and middle segments of the line in addition to the tip.
Patients and methods In a prospective study, proximal, middle and tip segments of PCVLs indwelling for more than 24 h in term and preterm infants were sent for culture at line removal. Definite CRS was considered as a positive peripheral blood culture plus any line segment growing the same organism in an infant with clinical signs of sepsis.
Results 189 lines were removed from 143 neonates: 142 (75%) were from well infants and 47 (25%) were from neonates with suspected clinical sepsis. The overall CRS rate was 7.9% (15 of 189 line episodes). In well infants, bacterial colonisation rates were significantly higher for proximal segments than for tips (p=0.004). Comparative rates of segmental culture positivity and their positive predictive values for definite CRS were similar for all segments. The diagnosis of CRS was not improved beyond a sole line tip culture by additional middle or proximal segmental cultures or by combinations of the three segments.
Conclusion In well infants, the proximal segments of PCVLs were more often colonised than line tips, but in clinically septic infants preferential culture of proximal or middle segments or combinations of the three segments did not permit better prediction of definite CRS than the culture of the line tip alone. Further studies prior to antibiotic therapy are indicated in babies with suspected CRS.
Statistics from Altmetric.com
Introduction
Percutaneous central venous lines (PCVLs) are independently responsible for most nosocomial bloodstream infections in the neonatal nursery.1 ,2 Bacteraemic infants experience fewer infection-related complications with prompt PCVL removal.3 Many centres routinely send PCVL tips for culture, either for all lines removed or only when catheter-related sepsis (CRS) is suspected. CRS is often diagnosed when a positive catheter tip culture yields the same organism as the peripheral blood culture (BC) in a baby with clinical signs of infection.4 However, culture of the PCVL tip in suspected CRS does not always return a positive bacterial growth to corroborate the diagnosis of CRS, and supportive evidence for the sensitivity of PCVL tip cultures in the diagnosis of CRS is lacking.
What is already known on this topic
▶ Indwelling central venous lines are a risk factor for nosocomial infection in neonates.
▶ Colonisation and infection of the central venous line happens primarily via the extra-luminal mode of the spread of organisms from the skin at the entry site of the central venous line.
What this study adds
▶ The proximal subcutaneous segment of the central venous line is more often colonised than the line tip or the mid-segment in well babies.
▶ Central venous line tip cultures may usefully inform the clinical management of septic babies, particularly in those with negative blood cultures due to prior antibiotic treatment.
▶ In babies with suspected sepsis, the culture of additional segments other than the line tip did not improve the diagnosis of catheter-related sepsis.
The density of skin flora at the insertion site is a major risk factor for CRS.5 Extraluminally acquired colonisation from cutaneous organisms is the commonest cause of infection in short-term, non-cuffed, non-tunnelled PCVLs.2 ,6 ,7 Logically therefore, proximal line segmental colonisation may precede that of the tip. A study in adults showed that proximal segments are colonised earlier and at a higher rate than line tips.8 Comparable studies are lacking in neonates. Our hypothesis was that the proximal and middle subcutaneous segments of indwelling PCVLs are colonised more frequently than tips and that the preferential culture of these segments will therefore more sensitively assist the diagnosis of CRS and colonisation than the sole culture of a line tip.
Methods
Study design
This was a prospective observational study in two tertiary-level neonatal intensive care units between February 2009 and April 2010. Our Local Research Ethics Committee deemed our study a service evaluation and waived the need for a formal review.
Percutaneous central venous lines
All PCVLs inserted in term and preterm infants in our centres were eligible. Lines were excluded if removed within <24 h in situ, if inserted at other units, or if still in situ in babies transferred elsewhere. PCVLs were inserted using aseptic technique by doctors or advanced neonatal nurse practitioners (ANNPs), and were removed by doctors, ANNPs or neonatal nurses according to the protocol. Two types of PCVL were used: Premicath 1Fr/28G (Vygon UK Ltd, Cirencester, Gloucestershire, UK) and Epicutaneo-Cava catheter 2Fr/24G (Vygon UK Ltd). These were non-tunnelled, single-lumen, non-antibiotic-impregnated catheters intended for short-to-medium-term use. The attending neonatologist was responsible for decisions regarding the timing of line insertion and removal. The type of PCVL and the site of insertion were chosen by the operator inserting the line.
Protocol for line removal and study samples
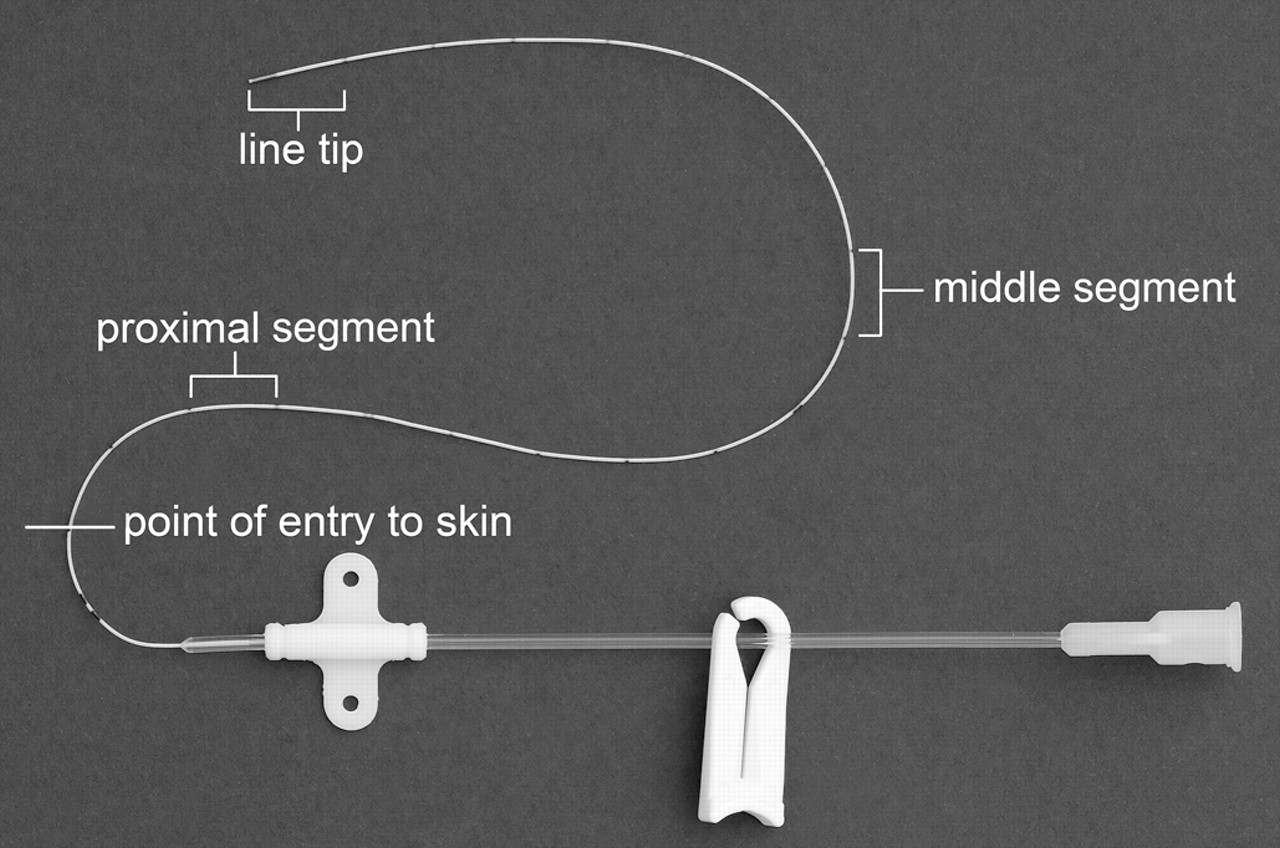
Line removal required two persons and preprepared, dedicated study packs to avoid cross-contamination between segments while cutting the line. Packs contained three sets each of sterile forceps, scissors and prelabelled containers. After removing external dressings, the skin around the entry site was disinfected with aqueous chlorhexidine and allowed to dry for 30 s before PCVL removal onto a sterile field. The PCVL was cut in the following order to obtain three approximately 1-cm-long formerly subcutaneous segments: (1) tip; (2) proximal, taken 1–2 cm from the point of skin entry; (3) middle (figure 1). Three segments were collected for all lines removed. For infants with suspected sepsis at line removal, a single peripheral BC was also concurrently obtained and sent for culture and sensitivity. Line segments were cultured by the Maki roll technique9 and a growth of >15 colony forming units was considered positive.

Segments of percutaneous central venous line taken for study.
Data collection
At line insertion, we recorded the date, infant's age, catheter type, anatomical site selected and subcutaneous line length. At removal, we recorded the date, mode of line use, reason for removal, whether CRS was suspected and the details of antibiotics if being given. Where CRS was suspected, supplementary data were collected for the period 1 day before to 3 days after line removal: specific clinical features of sepsis,1 white cell count (WCC), neutrophil count, platelet count and C reactive protein (CRP). Total WCC was considered abnormal if <5 or >20×109/l, the neutrophil count if <1.5 or >6×109/l and the platelet count if <150×109/l; CRP was considered raised if >10 mg/l.
Definition of CRS
The ‘suspected sepsis’ group was subdivided into four subgroups for analysis (figure 2). Subgroup 1: definite CRS – BC and any line segment were culture-positive with the same organism on the bacterial culture and sensitivity from a neonate with an indwelling PCVL and clinical signs of sepsis but no other focus for infection. Subgroup 2: probable CRS or indeterminate – at least one line segment had a positive growth in a clinically unwell baby, but BC was negative. Subgroup 3: definite sepsis, but likely non-CRS – BC was positive in a clinically unwell baby, but all line segments were culture-negative. Subgroup 4: clinical sepsis with negative bacteriology – CRS had been considered possible at line removal due to clinical signs of sepsis, but BC and all line segments were sterile on culture.

{kind=link}
{kind=link}
Flow chart of the study lines and their subgroups.
The ‘no sepsis’ group included the lines removed from well babies for all reasons other than suspected sepsis. These were further categorised according to bacteriology results: subgroup 5: colonised – at least one segment had a positive growth in a clinically well baby; subgroup 6: sterile – all three segments were culture-negative in a clinically well baby.
Sample size and statistical analysis
The primary outcome of interest was individual numbers of culture-positive proximal, middle and tip PCVL segments, for the overall study group and for babies with suspected CRS. Secondary analyses assessed the sensitivity of combinations of segments in the diagnosis of colonisation and definite CRS.
The sample size of 185 lines was calculated using a 7% expected CRS rate based on a previous study,10 aiming to detect a minimum proportional difference of 10% between the numbers of positive cultures in the proximal compared with tip segments with 80% power and 5% two-sided significance. Non-parametric tests (Mann–Whitney U and Kruskal–Wallis) were used. Proportions were assessed using χ2 or Fisher exact tests as appropriate. A p value of <0.05 was considered statistically significant.
Results
One hundred and eighty-nine PCVLs removed from 143 individual babies yielded 567 line segments. Figure 2 shows lines and their subgroups according to culture results. The number of lines inserted per baby ranged from one to four. No infant had multiple PCVLs concurrently in situ. The 189 lines were in situ for a total of 2190 days. Thirty-one lines (16.4%) remained in situ for >3 weeks. Table 1 shows the baseline characteristics of babies and lines overall, and for the two main subgroups of ‘suspected sepsis’ (n=47) and ‘no sepsis’ (n=142).
Baseline characteristics of the 189 percutaneous central venous lines and the babies
‘Suspected sepsis’ group
Forty-seven of 189 (25%) lines were removed because sepsis was suspected. Clinical signs were supported by either elevated or low white cell and neutrophil counts in 47% (22 of 47) and 26% (12 of 47), respectively, low platelet counts in 55% (26 of 47) and raised CRP in 80% (38 of 47). BC was positive in 23 of 47 (49%) babies with suspected sepsis at line removal, and of these 15 had at least one associated culture-positive line segment. The definite CRS rate overall was therefore 7.9% (15 of 189). Considering the utility of individual segments alone for diagnosing definite CRS, the tip would have yielded a rate of 6.8% (13 of 189), the middle a rate of 4.7% (9 of 189) and the proximal a rate of 4.2% (8 of 189). In terms of catheter days, the definite CRS rate was 15 of 2190 (6.8 infections per 1000 catheter days). In subgroup 2 (‘probable’ CRS) (figure 2), there were nine culture-positive lines in unwell babies with negative BCs, giving a composite ‘proven or probable’ CRS rate of 12.6% (24 of 189). Of the seven septicaemic infants (n=8 line removals) in subgroup 3 (definite sepsis, but likely non-CRS), one infant (n=2 line removals) had a separate septic focus (empyema and postlaparotomy wound infection), three had no other septic focus identified despite complete infection screens (negative cerebrospinal fluid (CSF) examination, urine culture and chest x-ray), and three did not have concomitant CSF and urine sent.
‘No sepsis’ group
One hundred and forty-two of 189 (75%) lines were removed for reasons other than suspected sepsis (figure 2). Thirty-seven of 142 (26%) showed colonisation (subgroup 5), with at least one culture-positive segment, and the remaining 105 of 142 (74%) were sterile (subgroup 6).
Culture-positive rates of the three line segments and their positive and negative predictive values
Table 2 shows the numbers of culture-positive segments overall (n=189 lines), from well neonates with ≥1 colonised segment (subgroup 5, n=37 lines), and from clinically septic neonates (subgroups 1–4, n=47 lines). Overall, the tip had a higher positive predictive value (PPV) than the proximal for the composite of colonisation and CRS (p=0.04), but there was no significant difference in PPV between the proximal and middle segments (p=0.49) or between the middle and the tip (p=0.13). In well babies, colonisation rates were higher for the proximal segments compared with the tips (p=0.004). For the 47 clinically septic neonates, the comparative rates of culture positivity did not differ between segments overall (p=0.14) or for the 15 infants with definite CRS (p=0.14), and their PPVs for definite CRS were similar.
Numbers of culture-positive line segments and their positive and negative predictive values for the various groups
Analysing tips alone, 20 of 47 (43%) were culture-positive from clinically septic babies compared with 16 of 142 (11%) from well babies (p<0.0001).
BC results and concurrent antibiotic treatment
BCs were positive in 23 of 47 (49%) infants with clinical sepsis at line removal. However, in 39 of 47 (83%) episodes, antibiotic treatment was already underway before PCVL removal: Prior antibiotics were received by 19 of 23 (83%) clinically-septic infants with positive BCs and 20 of 24 (83%) clinically-septic infants with negative BCs. Nine of 24 (38%) BC-negative babies had a positive growth in at least one segment: 7 of 9 tip; 5 of 9 middle; 3 of 9 proximal (tip vs proximal, p<0.0001). The tips were therefore culture-positive in 29% (7 of 24) BC-negative babies. Only 8 of 47 infants with clinical sepsis had not received antibiotics before line removal: 4 of these had a positive culture of ≥1 segment. Limiting analysis to these eight infants showed no differences between segments for assisting diagnosis of definite CRS (p=1.0).
Combinations of segments
Table 3 shows culture-positivity rates of various combinations of the segments, where at least one segment of each combination was culture-positive, and the predictive values for colonisation and/or definite CRS. In suspected sepsis, the rates of culture positivity of segmental combinations and PPVs for CRS were not significantly higher than for the tip alone, although the negative predictive value for CRS was higher for any combination of segments involving the tip compared with the tip alone (p=0.007).
Culture-positive rates for the combinations of the line segments and their positive and negative predictive values for catheter-related sepsis and colonisation
Microbiology of blood and line segment cultures
Table 4 presents the bacteriology of culture-positive blood and line segments. Coagulase-negative staphylococcus was isolated in 78% (18 of 23) culture-positive BCs and 92% (101 of 110) culture-positive line segments.
Bacteriology of blood culture and positive percutaneous central venous line segments
Discussion
To our knowledge, this is the first prospective study of PCVLs in neonates which analyses the value of the routine cultures of line segments in addition to the tip, and their diagnostic value for PCVL colonisation and CRS. Previous studies have focused on other factors relating to CRS, including the routes of infection, the types of catheters and the role of antibiotics to minimise infection.4 ,5 ,10,–,12
In respect of lines removed from well infants, our findings are consistent with a study in adults8 showing that the formerly subcutaneous proximal segments of PCVLs were more frequently colonised than the line tips (p=0.004), and suggesting that colonisation starts proximally at the insertion site. However, in the setting of clinically suspected sepsis with a high concomitant rate of antibiotic treatment, we found that neither proximal nor mid-segments had higher rates of culture positivity or better PPV for CRS compared with the tips alone. Rates of segmental culture positivity were similar, and multiple segmental combinations did not improve CRS diagnosis rates. Prior antibiotic treatment may have rendered line segments sterile on culture, negating any diagnostic advantage of proximal segments for CRS. Our findings imply that when a PCVL is removed from a septic baby, there is no diagnostic advantage from sending other line segments for culture instead of the tip.
The common route of bacterial CRS or colonisation in short-term PCVLs is via extra-luminal spread along the outer surface of the line rather than via intra-luminal spread from an infected hub.4 ,9 ,13 ,14 Our study used the Maki roll technique9 for the culture of line segments, which detects mainly the extra-luminal spread of infection. Other methods, such as endoluminal brush,14 sonication or flushing methods,8 may increase the sensitivity of the detection of colonisation due to additional diagnosis of intraluminal colonisation.8 A limitation of our study is that we did not employ such techniques.
It has been proposed that the longer a PCVL remains in situ, the higher the chances of CRs or colonisation.1 We found no significant differences in durations in situ between catheters removed from well babies and those with suspected sepsis.
We found that in the suspected sepsis group, more PCVLs had been inserted via a lower limb than via an upper limb route (p=0.0003), and furthermore that the frequency of the lower limb PCVL insertion was higher for the lines removed from clinically septic babies than from well babies (p=0.04). To our knowledge, such associations have not been reported previously. Lower limb PCVLs invariably have a longer physical length in vivo than do upper limb PCVLs. We speculate that a greater physical length of ‘foreign body’ present in vivo correlates directly with the risk of colonisation and therefore infection.
Some authorities recommend that paired BCs are drawn, from intravenous catheter and a peripheral site, to assist CRS diagnosis.15 Our study did not demand an additional BC through the PCVL because this is not usual practice in UK neonatal units.
Our study hypothesis was confounded by high rates of concurrent antibiotic use. Further prospective study is indicated to re-examine our hypothesis in a large series of lines removed before antibiotic therapy in babies with suspected CRS. The practical potential for such a study may be limited given that clinically septic babies are often treated pragmatically with antibiotics before line removal.
Conclusions
In infants with suspected sepsis, the culture of PCVL proximal and middle subcutaneous segments did not improve the diagnosis rate for definite CRS. Routine PCVL tip cultures provide a higher yield in babies with suspected sepsis than in well babies. Prior antibiotic treatment may significantly decrease the culture positivity of line segments; yet a significant minority of BC-negative babies nevertheless had a positive PCVL tip culture. PCVL tip cultures may usefully inform the clinical management of septic babies.
Acknowledgments
The authors sincerely thank all their colleagues, the doctors, ANNPs and nurses in both the neonatal units for so diligently helping with this study. The authors also thank the staff of both the microbiology departments for their support, and in particular Claire Stuart for help with microbiological data collection.
References
Footnotes
-
Competing interests None.
-
Ethics approval Norfolk Research Ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.