Article Text

Abstract
Objective: To determine the accuracy of predischarge visual assessment of jaundice for estimating bilirubin concentration and predicting risk of significant neonatal hyperbilirubinaemia.
Design: Prospective cohort study.
Setting: Well Baby Nursery at the Hospital of the University of Pennsylvania.
Patients: 522 term and late preterm newborns.
Interventions: Nurses used a 5-point scale to grade the maximum cephalocaudal extent of jaundice prior to discharge.
Main outcome measures: (1) Correlation between jaundice grade and bilirubin concentration. (2) Predictive accuracy of jaundice grade for identifying infants who developed significant hyperbilirubinaemia, defined as a bilirubin level that at any time after birth exceeded or was within 1 mg/dl (17 μmol/l) of the American Academy of Pediatrics-recommended hour-specific phototherapy treatment threshold.
Results: Nurses’ assessment of jaundice extent was only moderately correlated with bilirubin concentration and was similar in black and non-black infants (Spearman’s rho = 0.45 and 0.55, respectively (p = 0.13)). The correlation was particularly weak among infants <38 weeks’ gestational age (rho = 0.29) compared with infants ⩾38 weeks’ gestation (rho = 0.53, p = 0.05). Jaundice extent had poor overall accuracy for predicting risk of significant hyperbilirubinaemia (c-statistic = 0.65) but complete absence of jaundice had high sensitivity (95%) and excellent negative predictive value (99%) for ruling out the development of significant hyperbilirubinaemia.
Conclusions: Clinicians should not use extent of cephalocaudal jaundice progression to estimate bilirubin levels during the birth hospitalisation, especially in late preterm infants. However, the complete absence of jaundice can be used to predict with very high accuracy which infants will not develop significant hyperbilirubinaemia.
Statistics from Altmetric.com
For centuries clinicians have known that neonatal jaundice progresses in a cephalocaudal direction with progressive hyperbilirubinaemia. Its first comprehensive description appears in an 1847 thesis by Hervieux1 but it was not until 1969 that Kramer systematically correlated advancing dermal zones of jaundice with actual serum bilirubin levels.2 Despite its long history of use, few studies have evaluated the accuracy and reliability of visual assessment for estimating severity of hyperbilirubinaemia, and experts have debated its value. Some studies have demonstrated that experienced neonatologists are capable of using the cephalocaudal progression of jaundice to accurately estimate bilirubin levels3 and identify infants with significant hyperbilirubinaemia,4 while others have found that visual assessment is neither reliable nor accurate for predicting bilirubin levels.5
What this study adds
The extent of cephalocaudal progression of jaundice is not strongly correlated with measured bilirubin values during the birth hospitalisation.
However, infants with absolutely no jaundice have a very low risk of developing significant hyperbilirubinaemia.
With greater recent emphasis on predischarge screening for risk of significant hyperbilirubinaemia,6 the value of visual assessment of jaundice in predischarge risk assessment has come into question.7 Does jaundice extent correlate strongly enough with bilirubin level prior to discharge such that it can be used to determine which infants need predischarge bilirubin measurements? And does the extent of jaundice prior to discharge predict which infants will develop significant neonatal hyperbilirubinaemia? We sought to answer these questions in a large multiracial population of term and late preterm newborns.
Methods
Design, setting, and subjects
This analysis was performed as part of a larger prospective cohort study designed to compare alternative risk assessment strategies for predicting and preventing severe neonatal hyperbilirubinaemia. Details of the recruitment and follow-up procedures for that study have been published previously.8 The study was conducted in the Well Baby Nursery of the Hospital of the University of Pennsylvania (HUP), an urban tertiary care hospital. Infants were eligible for enrolment if they were managed exclusively in the Well Baby Nursery and if they were ⩾36 weeks’ gestational age (GA) and weighed ⩾2000 g, or if they were ⩾35 weeks’ GA and weighed ⩾2500 g. Infants who were transferred to the intensive care nursery for any reason and those who received more than 48 h of intravenous antibiotics for concern for sepsis were excluded from the study.
Study protocol
Visual assessment of jaundice
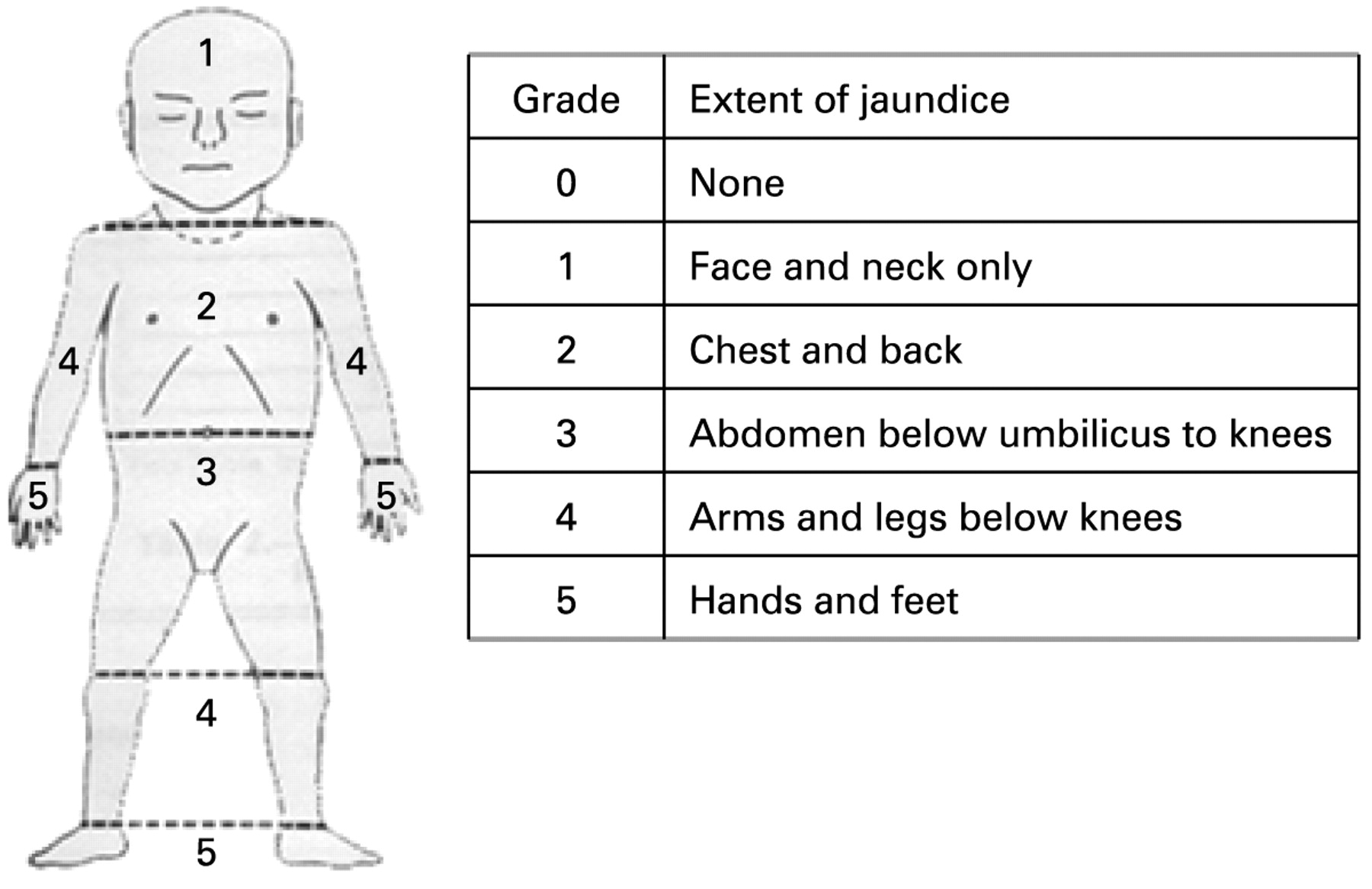
Nurses used the homunculus from the Kramer study2 (fig 1) to assess the maximum extent of infant jaundice on a 5-point scale. Jaundice assessments were performed on the day following the second night of hospitalisation (or the day of discharge if the infant was discharged earlier) to simulate the timing of predischarge decision-making during a typical vaginal birth hospitalisation stay. Jaundice assessments were performed by Well Baby Nursery nurses with ⩾2 years of nursery experience, who were not caring for the infant being evaluated and were blinded to the infant’s bilirubin values.

Schema for grading extent of jaundice.2 Nurses blinded to bilirubin values were instructed to grade the extent of jaundice by assigning a number corresponding to the maximum extent of jaundice progression. For example, an infant found to have jaundice extending to the upper arms (grade 4) and upper legs (grade 3) was categorised as grade 4 jaundice.
Bilirubin measurements
Each infant had a transcutaneous bilirubin (TcB) measurement obtained at least once a day until discharge. TcBs were measured using BiliCheck (Respironics, Murrysville, Pennsylvania, USA), a Food and Drug Administration-approved non-invasive bilirubinometer. Conforming with the standard of care in the nursery, infants whose TcB measurement exceeded the 75th percentile on an hour-specific bilirubin nomogram9 had a total serum bilirubin (TSB) measurement obtained. Because the BiliCheck is less accurate at TcB levels above 13 mg/dl (222 μmol/l),10 11 our protocol also dictated that all TcB values ⩾12 mg/dl be confirmed with a TSB.
Bilirubin measurements generally peak at age 3–5 days, and so we attempted to obtain bilirubin measurements on all study infants in this timeframe. If an infant’s birth hospitalisation was longer than 72 h, we obtained at least one TcB measurement prior to discharge between 72 and 120 h of life. For infants who were discharged from the hospital before 72 h of life, a study nurse equipped with a BiliCheck device attempted to perform a home visit to obtain a TcB between 72 and 120 h of life (as well as a heel stick TSB if the TcB was ⩾12 mg/dl (205 μmol/l)).
If a high TcB triggered the performance of a TSB (either because the TcB exceeded the 75th percentile before discharge, or was ⩾12 mg/dl at any time), we used the TSB instead of the TcB for analyses. To evaluate the correlation between the visual assessment of extent of jaundice and the bilirubin value, we paired each jaundice assessment value with a bilirubin (TcB or TSB) value obtained within 8 h of the jaundice assessment.
Significant hyperbilirubinaemia
Significant hyperbilirubinaemia was defined as a bilirubin level (TcB or TSB) that at any time after birth exceeded or was within 1 mg/dl (17 μmol/l) of the hour-specific phototherapy treatment threshold recommended in the American Academy of Pediatrics (AAP)’s Clinical Practice Guideline on management of neonatal hyperbilirubinaemia.6 Infants who received phototherapy prior to developing significant hyperbilirubinaemia as defined above were classified as not developing the outcome. We followed the AAP guideline in using specific risk factors (GA and Coombs positivity) for bilirubin neurotoxicity to select the appropriate phototherapy treatment threshold curve for each infant. Coombs status was available for 146 (28%) of all studied infants and 72 (32%) of the infants born to mothers with blood type “O”.
Covariates
Information on maternal, infant and delivery characteristics was abstracted from chart review by two research assistants. Maternal race, intended method of feeding after discharge (breast, bottle, both), and history of previous infant with jaundice or requiring phototherapy was reported by the mother during structured interviews prior to discharge. GA was abstracted from the obstetric record and was generally estimated from fetal ultrasound or last menstrual period. For the purposes of analysis we rounded GA to the nearest whole week (eg, 37 and 4/7 weeks = 38 weeks) and dichotomised the variable at 38 weeks (<38 weeks, ⩾38 weeks). All covariate data were collected during the birth hospitalisation.
Analysis
Correlation of extent of jaundice with bilirubin level
For each infant we paired the jaundice assessment with the closest bilirubin measurement obtained within 8 h of the jaundice assessment. We then plotted the jaundice grade against the paired bilirubin value and measured their correlation using the Spearman correlation coefficient. Previous studies have suggested that visual assessment of jaundice extent is less accurate in darker pigmented12 and premature13 14 newborns. Thus, we performed subgroup analyses to evaluate the correlation of extent of jaundice with bilirubin value by race (black vs non-black) and GA (<38 weeks or ⩾38 weeks). To compare Spearman rho correlation coefficients, we first performed a Fisher’s z transformation of the rhos (z = 0.5×ln((1+rho)/(1−rho))) and then computed a two-sample z test using the following formula:
λ = (z1−z2)/((1/(n1−3))+(1/(n2−3)))
where z1 and z2 are the z transformation values for rho1 and rho2, and n1 and n2 are the sample sizes for the two groups from which rho1 and rho2 were calculated.15
Negative predictive value of complete absence of jaundice
To determine whether complete absence of jaundice can be used to identify newborns who do not need a predischarge bilirubin measurement for risk assessment purposes, we evaluated the negative predictive value of a jaundice grade of “0” for ruling out a bilirubin value >40th percentile on the hour-specific bilirubin nomogram. This cut-off was chosen because numerous studies have demonstrated that infants with predischarge bilirubin <40th percentile on the hour-specific bilirubin nomogram have a near 0% risk of developing significant neonatal hyperbilirubinaemia.8 9 16 17
Predictive value of jaundice assessment for identifying infants who develop significant hyperbilirubinaemia
We also determined whether the jaundice grade was predictive of whether an infant developed significant hyperbilirubinaemia. Overall predictive accuracy was measured using the c-statistic,18 which is mathematically equivalent to the area under the receiver operating characteristics curve19 for the risk assessment strategy. We also calculated the negative predictive value of a jaundice grade of “0” for ruling out the development of significant hyperbilirubinaemia.
All data were collected by research assistants and entered directly into a Microsoft Access (Redmond, Washington, USA) database. Analyses were performed using SAS V.9.1 (Cary, North Carolina, USA) and Stata V.8 (College Station, Texas, USA). Informed consent was obtained from mothers of all infants in the study. The institutional review boards from the University of Pennsylvania School of Medicine and the Children’s Hospital of Philadelphia approved the study protocol.
Results
Subject characteristics
Between September 2004 and October 2005, 1749 infants were born on days when recruitment occurred. A total of 1079 (62%) families were approached for enrolment in the study and of those, a total of 823 (76%) consented to participate. Eleven patients were excluded from the study after they developed exclusion criteria (seven transferred to Intensive Care Nursery and four received antibiotics for more than 48 h), leaving a total of 812 infants. We were able to ascertain the development of significant hyperbilirubinaemia in 751 (92%) infants: 47 (6%) who received phototherapy during the birth hospitalisation and 704 (87%) who did not but had a bilirubin value obtained between 72 and 192 h (mean age = 97 h; interquartile range (IQR) = 82–120 h). Sixty-one infants (8%) were lost to follow-up and did not have birth hospitalisation phototherapy or a bilirubin value obtained after 72 h. Of the 751 infants for whom the outcome (significant hyperbilirubinaemia) could be ascertained, 685 (91%) had a jaundice assessment performed. We were able to pair the jaundice assessment with a bilirubin value obtained within 8 h of the assessment for 522 (70%) of these infants, who formed the sample for this analysis (fig 2). Table 1 lists their baseline characteristics.

Enrolment and follow-up of study subjects.
Subject characteristics (n = 522)
Correlation of jaundice grade with bilirubin level
The nurses’ assessment of jaundice extent (graded from 0 to 5) was moderately correlated with the bilirubin value measured within 8 h of the assessment (Spearman’s rho = 0.51; p<0.001). The correlation was similar among black infants (Spearman’s rho = 0.45; p<0.001) and non-black infants (Spearman’s rho = 0.55; p<0.001) (p value for difference = 0.13), but was particularly weak among infants <38 weeks’ GA (rho = 0.29; p<0.04) compared with infants ⩾38 weeks’ gestation (rho = 0.53; p<0.001) (p value for difference = 0.05).
Dot plots of the bilirubin value versus jaundice grade for black and non-black infants (fig 3) demonstrate that, despite this correlation, there is significant overlap of bilirubin values across jaundice grades. Greater differences in jaundice grade (eg, grade 3 vs grade 0 compared with grade 1 vs grade 0) produce better separation of bilirubin values, especially with non-black infants, but significant overlaps in bilirubin values persist even across large differences in jaundice grade.
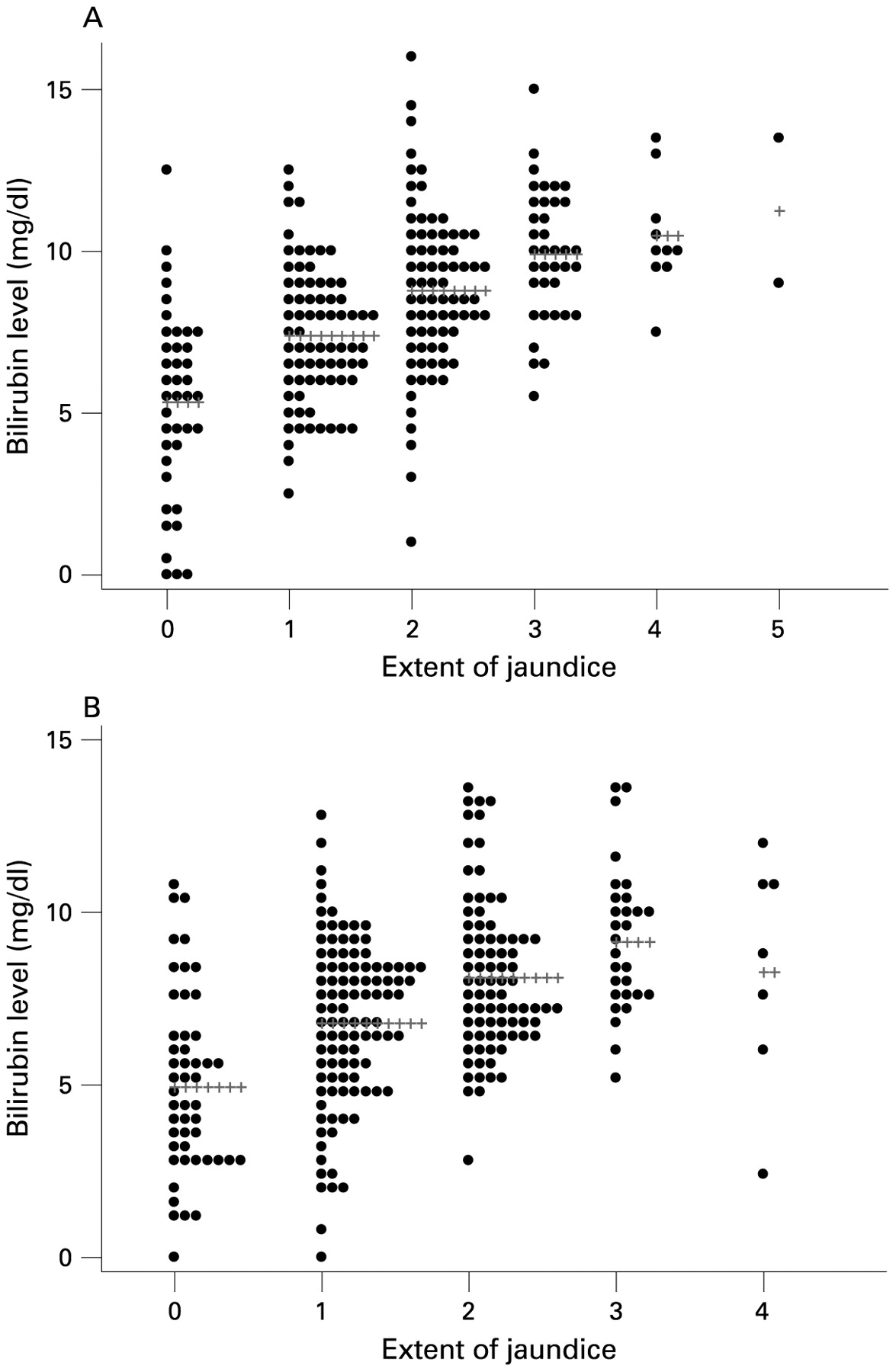
A. Non-black infants. B. Black infants. Mean bilirubin value for each grade of jaundice indicated by ++++++++.
Negative predictive value of complete absence of jaundice
Nurses assigned 91 (17%) infants a jaundice grade of “0”, indicating a complete absence of jaundice. The bilirubin values for these infants ranged from 0 to 12.5 mg/dl (mean = 5; IQR (2.9–7.2)). The wide range of bilirubin values for infants thought to have no jaundice was observed in both black (range 0–10.7 mg/dl) and non-black (range 0–12.5 mg/dl) infants. Among infants who had no jaundice observed, 76 (84%) had a concurrent bilirubin value in the low-risk zone of the hour-specific bilirubin nomogram, which is associated with a very low risk of developing severe hyperbilirubinaemia. However, complete absence of jaundice was not perfectly accurate for ruling out a concurrent predischarge hour-specific bilirubin above the low-risk zone. Ten (11%) had bilirubin values in the low–intermediate risk zone, 4 (4%) had bilirubin values in the high–intermediate risk zone, and 1 (1%) had a bilirubin value in the high-risk zone. The negative predictive value of complete absence of jaundice for identifying infants with bilirubin value in the low-risk zone was imperfect in both black (84%) and non-black (83%) infants (table 2).
Relationship between absence of jaundice and hour-specific bilirubin risk zone*
Predictive value of jaundice assessment for identifying infants who develop significant hyperbilirubinaemia
Twenty (4%) infants developed significant hyperbilirubinaemia (ie, had bilirubin levels exceeding or within 1 mg/dl of the phototherapy treatment threshold). The odds of developing significant neonatal hyperbilirubinaemia increased about 60% with each incremental increase in jaundice grade (OR = 1.6; 95% CI (1.1 to 2.4)) (fig 4), but as a continuous predictor of significant neonatal hyperbilirubinaemia, jaundice grade had poor overall discriminatory power (c-statistic = 0.65; 95% CI (0.50 to 0.80)). However, the complete absence of jaundice (grade “0”) had high sensitivity (95%; 95% CI (75 to 100%)) and a very high negative predictive value for ruling out the development of significant hyperbilirubinaemia (99%; 95% CI (94 to 100%)). The one infant (of 91) with no observed jaundice (at 54 h of age) who developed significant hyperbilirubinaemia was a South-Asian breast fed boy (GA 37 and 2/7 weeks, birth weight 3540 g, blood type B negative, Coombs negative) delivered by caesarean who developed a bilirubin value of 14.2 mg/dl at 63 h of life and had phototherapy started in hospital prior to discharge.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Extent of jaundice and development of significant hyperbilirubinaemia.
Discussion
Our results illustrate the utility and limitations of using the visual assessment of cephalocaudal extent of jaundice for management decisions in term and late preterm newborns. The extent of jaundice, as determined by the Kramer scale, was only moderately correlated with bilirubin level and could not be used to accurately predict the infant’s absolute bilirubin level or risk of developing significant hyperbilirubinaemia. Despite the widely accepted premise that darkly pigmented infants are more difficult to assess clinically for jaundice, we found no statistically significant difference in correlation with bilirubin values. The one group for whom assessment of jaundice extent was particularly poorly correlated with bilirubin level was the late preterm infants (35–38 weeks’ GA). Although extent of jaundice did not strongly correlate with bilirubin level, the complete absence of jaundice (Kramer grade “0”) was clinically informative. The predischarge bilirubin value of infants with no jaundice was almost always in the low-risk zone on the hour-specific bilirubin nomogram, and their actual risk of developing significant hyperbilirubinaemia was exceedingly low (≈1%), regardless of their race or GA.
Our study has several limitations worth noting. Ideally the bilirubin measurements and jaundice assessments would have been performed at the exact same time, but the correlation between extent of jaundice and bilirubin value was not the primary aim of the main study from which these data were obtained, and financial and logistical obstacles prevented us from coordinating these measurements. However, the hour-specific bilirubin percentiles published by Maisels20 show that the most rapid average bilirubin increase occurs in the first 36 h of life and does not exceed 1.5 mg/dl over an 8 h period, and is generally less than 1 mg/dl/8 h period throughout the other percentile tracks. The mean difference in time between the bilirubin measurement and jaundice assessment in our study was 4.2 h (bilirubin measurement preceding the jaundice assessment) with an IQR of 2.5–6.25 h. Our study is also limited by the sampling frame of the jaundice assessments, which occurred solely during the first 3 days of life (mean 47 h, IQR 40–53 h) when bilirubin levels averaged 7.6 mg/dl (IQR 5.9–9.4 mg/dl) as we were primarily interested in the value of jaundice assessment for predischarge prediction and prevention of severe hyperbilirubinaemia. It is possible that the correlation between Kramer jaundice grade and bilirubin level may be different after 3 days when bilirubin levels are often significantly higher. We did not train the nurses in jaundice assessment, evaluate inter-rater reliability, or evaluate the relationship between years of nursing experience and accuracy of jaundice assessment as we were interested in the real world effectiveness of jaundice assessment. Formal training and efforts to improve inter- and intra-rater reliability might have improved the accuracy and predictive value of jaundice assessments. Finally, our selection of phototherapy threshold curves for defining significant hyperbilirubinaemia was based largely on GA, and did not incorporate Coombs status for the majority of infants who did not have it measured, or G6PD deficiency as it was not assessed quantitatively in these infants. Knowledge of these risk factors might have changed the phototherapy threshold curve used for some infants in our analyses.
Compared with previous work carried out in this area, our study has many strengths. The sample assembled to evaluate the correlation between extent of jaundice and bilirubin level is the largest one reported to date. It includes large numbers of both black and non-black infants, which allowed us to evaluate indirectly the effect (or lack thereof) of skin tone on jaundice assessment. We also avoided some of the methodological flaws of previous studies, such as including multiple observations per infant (which introduces statistical problems of non-independence of observations) and omission of correlation coefficients. Our study concurs with previous reports that also found absence or paucity of jaundice to be useful for ruling out higher bilirubin levels,5 12 however, ours is the first to determine the value of jaundice assessment for predicting an infant’s risk of developing significant hyperbilirubinaemia.
Conclusions
The extent of cephalocaudal progression of jaundice graded by the Kramer scale correlates poorly with measured bilirubin values and therefore clinicians should not use it to estimate bilirubin levels during the birth hospitalisation. Its utility is particularly limited for late preterm infants, a group that is at greatest risk of developing significant hyperbilirubinaemia. Although the extent of jaundice does not accurately predict which infants have a bilirubin level above the 40th percentile on the hour-specific bilirubin nomogram or which infants will develop significant hyperbilirubinaemia, the complete absence of jaundice is associated with an exceedingly low risk of developing significant hyperbilirubinaemia. Thus, in experienced hands the complete absence of jaundice can be used to select infants, both black and non-black, for whom predischarge bilirubin screening may be deferred. However, these results need to be validated in other patient populations, and the benefits of this selective screening strategy (less testing, lower costs) must be weighed against the risk of inaccurate jaundice assessments in inexperienced observers and the loss of reliable and objective risk assessment that is afforded through universal bilirubin screening. The negative predictive value of complete absence of jaundice prior to discharge for ruling out the development of significant hyperbilirubinaemia is determined in part by the prevalence of this outcome in the population being screened. And so although the sensitivity of complete absence of jaundice in our study was high (95%), in populations with a higher prevalence of significant hyperbilirubinaemia the negative predictive value may be less than observed in our study. It is also important to note that the majority of our jaundice assessments were performed between 40 and 53 h of age, and none were performed in the first 26 h. Thus, absence of jaundice in an infant discharged before 24 h of age does not rule out the development of significant hyperbilirubinaemia, and predischarge bilirubin screening is especially useful in that setting. Finally, lack of visible jaundice prior to discharge does not obviate the need for the recommended early post-discharge follow-up by primary care paediatricians.6
Acknowledgments
We would like to thank research assistants Sasha Waring and Patrick Maloney, study nurse Tajuanna Harris, Dr Susan Friedman, and all the nurses and nurse practitioners in the HUP Well Baby Nursery for making this study possible.
REFERENCES
Footnotes
Funding RK was supported by grant number K23 HD043179 from the National Institute of Child Health and Human Development, Bethesda, Maryland, USA. This study was also supported by Respironics (Murrysville, Pennsylvania, USA), which loaned us a BiliCheck device for bilirubin measurements during home visits and donated a limited supply of BiliCheck disposable tips.
Competing interests None.
Ethics approval The institutional review boards from the University of Pennsylvania School of Medicine and the Children’s Hospital of Philadelphia approved the study protocol.
Patient consent Parental consent obtained.
Linked Articles
- Fantoms
- Perspective