Article Text

Abstract
Background: An objective definition of bronchopulmonary dysplasia (BPD) is required to interpret trial outcomes and provide a baseline for prognostic studies. Current definitions do not quantify disease severity. The cardinal measures of impaired gas exchange are a reduced ventilation:perfusion ratio (VA:Q) and increased right to left shunt. These can be determined non-invasively by plotting arterial oxygen saturation (Spo2) against inspired oxygen pressure (PIo2).
Aims: To describe the reduced VA:Q and shunt in infants with BPD and evaluate these as graded measures of pulmonary dysfunction.
Methods: 21 preterm infants with BPD were studied. PIo2 was changed stepwise to vary Spo2 between 86% and 94%. Pairs of PIo2 and Spo2 data points for each infant were plotted and analysed to derive reduced VA:Q ratio and shunt.
Results: In every infant, the Spo2 versus PIo2 curve was shifted to the right of the normal because of a reduced VA:Q. The mean (SD) shift was 16.5 (4.7) kPa (normal 6 kPa). Varying degrees of shunt were also present, but these were less important in determining Spo2 within the studied range. The degree of shift was strongly predictive of the PIo2 required to achieve any Spo2 within the range 86–94% (R2>0.9), permitting shift and VA:Q to be determined from a single pair of PIo2 and SpO2 values in this range.
Conclusions: The predominant gas exchange impairment in BPD is a reduced VA:Q, described by the right shift of the Spo2 versus PIo2 relationship. This provides a simpler method for defining BPD, which can grade disease severity.
- BPD, bronchopulmonary dysplasia
- Pco2, arterial carbon dioxide tension
- Po2, arterial oxygen tension
- PIo2, partial pressure of inspired oxygen
- Spo2, arterial oxygen saturation
- VA:Q, ventilation:perfusion ratio
Statistics from Altmetric.com
- BPD, bronchopulmonary dysplasia
- Pco2, arterial carbon dioxide tension
- Po2, arterial oxygen tension
- PIo2, partial pressure of inspired oxygen
- Spo2, arterial oxygen saturation
- VA:Q, ventilation:perfusion ratio
Despite great improvements in the survival of infants born prematurely, there continues to be a large number of infants who develop bronchopulmonary dysplasia (BPD). This causes them to remain in hospital longer, prolongs their requirement for supplemental oxygen, and is associated with long-term morbidity and an increased risk of mortality. Reducing BPD remains a major focus of clinical and research activity.
An objective definition of BPD is required to enable reliable interpretation of clinical trial outcomes and to serve as a baseline in prognostic studies. Yet, an ideal definition has been elusive. Definitions based on the infant having a requirement for supplemental oxygen at 28 days of life1 or at 36 weeks’ gestation2 have been used widely, but their usefulness is severely limited by the marked variation among clinicians in their criteria for oxygen supplementation.3 A definition based on the use of oxygen treatment alone gives wide variations in the incidence of disease, which reflect little more than clinician variation and have little relevance to the severity of any underlying pathology.4 Recently, a physiological definition has been proposed that aims to remove this bias by defining BPD as a requirement for supplemental oxygen, to maintain an oxygen saturation of 90% at 36 weeks’ gestation.4 This is undoubtedly an advance. However, healthy preterm and term infants have saturations around 97% in air,5,6 and saturations lower than this in air must reflect a degree of gas exchange impairment, even if supplemental oxygen is not always deemed necessary. Present approaches to defining BPD classify these infants as disease free.
By non-invasive measurements of PIo2 and Spo2, it is possible to quantify the severity of gas exchange impairment in a graded fashion and to partition this between the contribution made by reduced ventilation:perfusion ratio (VA:Q) and that made by right to left shunt.7,8,9,10,11 We have applied this method to analyse the gas exchange abnormalities in infants with BPD and used these observations to model an improved approach to the definition of BPD, which measures the severity of gas exchange impairment.
METHODS
Underlying physiology
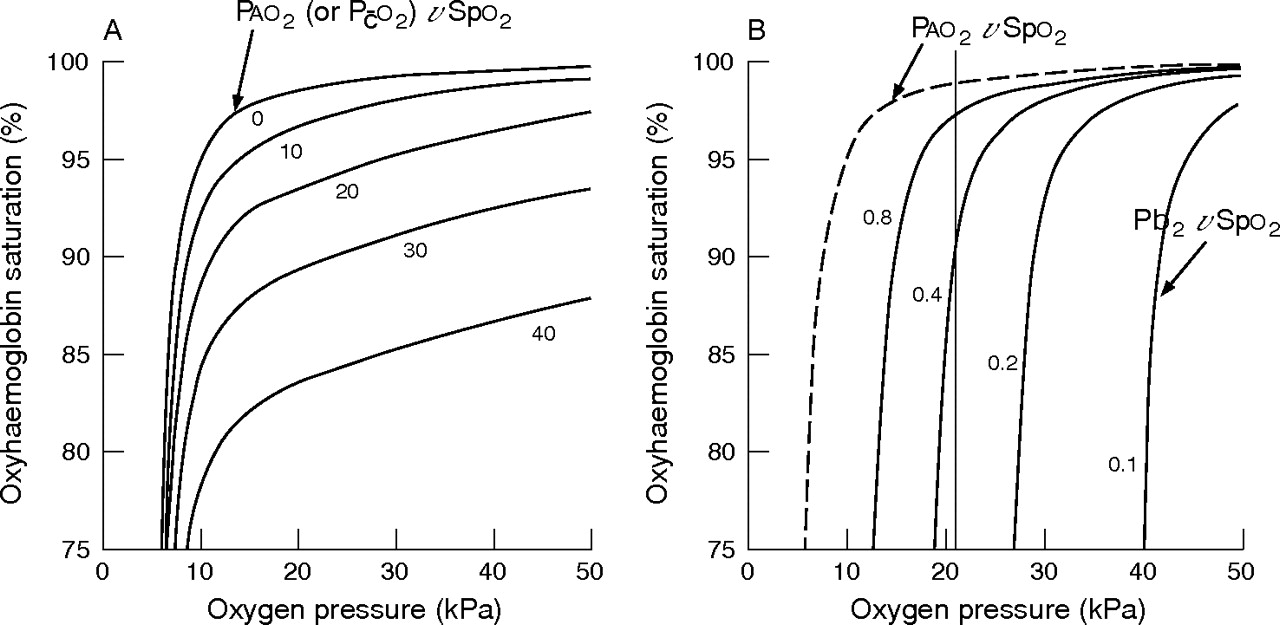
A reduced VA:Q ratio and an increased shunt have different effects on the relationship between inspired oxygen pressure (PIo2) and arterial oxygen saturation (Spo2). A reduced VA:Q ratio decreases alveolar and arterial oxygen tension (Po2) and raises alveolar and arterial carbon dioxide tension (Pco2). Increasing PIo2 restores the alveolar Po2 and Spo2 to normal, overcoming the effect of the reduced VA:Q ratio. Increased shunt does not raise Pco2 but reduces Spo2 because the shunted blood is not exposed to alveolar oxygen. Increasing PIo2 can compensate for only a small amount of shunt, because the non-shunted blood is already almost fully saturated and does not carry much more oxygen than small amounts in solution when PIo2 is increased. These independent effects on gas exchange can be represented in the form of plots of Spo2 against PIo2 (fig 1).8,9,10,11,12

Plots of oxyhaemoglobin saturation (Spo2, %) against inspired oxygen pressure (PIo2, kPa).10 (A) Increasing shunt from 0% to 40% lowers the position of the upper part of the curve. (B) Reducing ventilation:perfusion ratio (VA:Q) from 0.8 to 0.1 shifts the curve to the right. The right shift of each PIo2–Spo2 curve from the position of the dissociation curve (dashed line) is the PIo2–Pao2 difference (kPa), which includes Paco2/R. The 0.8 curve represents the normal adult curve, which intercepts a PIo2 of 21 kPa (vertical line) at 97% Spo2. R, respiratory gas exchange rate.
At sea level (1 atm), PIo2 (kPa) is the same as the inspired oxygen percentage. The curve relating alveolar (mixed capillary) Po2 to oxygen saturation in the ideal lung represents the shape of the oxyhaemoglobin dissociation curve. Increasing shunt displaces the top part of the curve downwards (fig 1A) as the maximum Spo2 obtainable falls. In contrast, reducing the VA:Q ratio shifts the whole curve to the right (fig 1B). The degree of the right shift, using the oxygen dissociation curve as the reference, is determined by the reduction in the VA:Q ratio and a rise in alveolar PCo2. The normal curve is shifted to the right of the haemoglobin–oxygen dissociation curve by 6 kPa, which is largely Pco2/R (where R is the respiratory gas exchange ratio). An additional right shift compared with the normal represents the increase in PIo2 that will be required to restore the mixed capillary Po2 to normal levels and thereby permit normal arterial saturation. If multiple pairs of PIo2 and Spo2 values are obtained from the same patient, then a single pair of shunt and shift values can be derived. This can be done graphically7–9 by moving a set of shunt curves such as those in fig 1A laterally over the plot of PIo2–Spo2 data points until one of the shunt curves superimposes the data points. The degree of shift can then be read off the axis of the graph, and the shunt can be determined by selecting the shunt curve that most closely fits the data. Alternatively, shift and shunt can be calculated using a computer algorithm that derives confidence intervals for the shunt and shift values, and coefficients of determination (R2) for the fit of the data to the shunt and shift model.8,9,10
Procedure
We studied 21 preterm infants who were considered to have BPD on the basis of a continuing requirement for supplemental oxygen at 36 weeks’ gestation. The study was approved by the institutional ethics advisory committee and written informed consent was obtained from the parents in all cases. This was a convenience sample. Infants were included if they were receiving supplemental oxygen but not other support at the time of study. According to our unit policy, oxygen was being given as required to maintain oxygen saturation in the target range 86–94%. All infants were being cared for in the neonatal unit of the Simpson Centre for Reproductive Health, Royal Infirmary of Edinburgh, Edinburgh, UK, between January 2002 and March 2005. All studies were carried out within 2 weeks of the infant reaching 36 weeks’ gestation.
At the time of study all infants were receiving oxygen via nasal cannulae. To enable measurement and control of PIo2, the infants were placed in a neonatal intensive care incubator with oxygen under servo control (Draeger 8000IC, Draeger Medical AG & Co KGaA, Lübeck, Germany). The oxygen analyser was calibrated at the start of each study. Functional Spo2 was measured using either a Siemens SC7800 (Siemens Medical Systems Inc, Danvers, MA, USA) or a Philips M3046A multiparameter patient monitor (Agilent Technologies, Boblingen, Germany), depending on which nursery the infant was being nursed in. Studies began at least 30 min after a feed and were conducted with the infant lying supine. PIo2 was reduced in increments of 1–2% (1–2 kPa) and then increased again to vary Spo2 between 94% and 86%. At each PIo2 value, the infant was allowed to stabilise for about 5 min before a pair of Spo2 and PIo2 values was recorded. Values were recorded only if there was a good pulse waveform on the oximeter and the infant was not displaying gross body movements.
Sleep state was not standardised. PIo2 was never reduced below 21 kPa, and oxygen administration to saturation >94% was minimised as per unit policy.
The pairs of PIo2 and Spo2 data points obtained from each infant were plotted and analysed using a computer algorithm that gave a curve representing a single solution for shunt and shift (the difference between PIo2 and mixed capillary Po2) for each infant’s dataset.8,9,10 If the data pairs obtained did not describe the plateau of the oxyhaemoglobin dissociation curve, the algorithm was sometimes unable to calculate the shunt and shift values. Under these circumstances the data were plotted manually, and shunt and shift were determined from the graphs directly using the method described above.
As right shift is due to the combined effects of raised Pco2 and reduced VA:Q ratio, we determined the contribution of these two variables using a mathematical model of gas exchange described by Olszowka and Wagner.12 PIo2–Spo2 curves were constructed for VA:Q values from 0.9 to 0.15, and the predicted Paco2 value was calculated from the model. From this we related the shift value in each infant to a particular VA:Q and compared the child’s most recent Pco2 measurement with the predicted Pco2.
RESULTS
Table 1 describes the clinical characteristics of the 21 infants. All infants were receiving supplemental oxygen at the time of study. There was wide variation among the infants in the length of time that each had been on a ventilator or supported with continuous positive airway pressure. Some were still cycling on and off continuous positive airway pressure.
Characteristics of the infants studied
The main finding was that in every infant the PIo2 versus Spo2 curve was shifted to the right of the oxygen dissociation curve. The mean (standard deviation (SD)) shift was 16.5 (4.7) kPa (table 2). The normal PIo2–Spo2 curve is shifted 6 kPa to the right of the dissociation curve and is identical to the VA:Q 0.8 curve shown in fig 1B. This intercepts the vertical line at 21 kPa PIo2 at an Spo2 of about 97%. Figure 2 shows the data plots of infants 2, 10, 11 and 19 in relation to the oxyhaemoglobin dissociation (ideal) curve and the normal adult PIo2 versus Spo2 curve. Table 2 shows the values for shunt and right shift for all 21 infants, with 95% confidence interval (CI) and R2. In three infants (5, 8 and 18), the range of paired values of PIo2 and Spo2 obtained did not describe enough of the plateau of their PIo2 versus Spo2 relationship to enable the algorithm to calculate the shunt and shift values. Their data points were plotted, and the shunt and shift values were determined manually from the graphs as described above; data of these infants do not therefore include CI or R2. All three infants had Spo2 ⩾90% breathing air.
Shunt and right shift of the arterial oxygen saturation versus partial pressure of inspired oxygen curve, R2, for the fit to the model and ventilation:perfusion ratio

Plots of oxyhaemoglobin (OxyHb) saturation (Spo2, %) versus inspired oxygen (PIo2, kPa) for infants 2, 10, 11 and 19. Reference grid lines are added at an Spo2 of 90% and a PIo2 of 21 kPa. The haemoglobin oxygen dissociation curve (ideal lung) is the reference point for derivation of shift. The normal Spo2–PIO2 curve is also included for comparison.
As a significant right shift of the PIo2 versus Spo2 curve occurred in every case, and was a sensitive measure of a reduced VA:Q ratio, we looked for an index of right shift that might obviate the need to produce a range of different PIo2 values in each case. In every infant, the 90% Spo2 value fell on the steep part of the dissociation curve so that the PIo2 needed to produce 90% Spo2 might be a candidate marker of right shift. Figure 3 shows plots of the degree of shunt and shift in each infant against the PIo2 required to achieve 90% Spo2. At this Spo2, the relationship between PIo2 and shift was highly siginificant and linear, whereas that between PIo2 and shunt was weak, indicating that shift was the main determinant of reduced Spo2 in these infants.

{kind=link}
{kind=link}
{kind=link}
(A) Partial pressure of inspired oxygen (PIo2) required to achieve an arterial oxygen saturation (Spo2) of 90% versus shunt. (B) PIo2 required to achieve an Spo2 of 90% versus shift.
We constructed plots of shift against the PIo2 required to achieve each saturation in the range 86–94% Spo2, and found linear relationships between shift and PIo2 at all of the Spo2 values in this range, with all values of R2>0.9. The consistency of the relationship between shift and PIo2 in this range was such that multiple data pairs in each infant were not required to derive shift. A single pair of PIo2 and Spo2 values in the Spo2 range 86–94% was sufficient to predict the shift value that would be derived from the whole data series. The mean (SD) difference between shift calculated from individual data pairs and that calculated from the entire data series for each infant was 0.24 (1.25) kPa.
To enable others to derive shift from a single pair of Spo2 and PIo2 values, shift was calculated from the results of this study for a range of PIo2 and Spo2 values that are likely to be observed in infants with BPD at 36 weeks’ gestation. Table 3 shows the results.
Right shift (kPa) of the arterial oxygen saturation (Spo2) versus partial pressure of inspired oxygen (PIo2) relationship for different pairs of PIo2 and Spo2 values
Pco2 predicted by the model of Olszowka and Wagner12 for the degree of a reduced VA:Q ratio in each infant was linearly related to measured Pco2 (y = 0.68x+3.2, R2 = 0.6). This is only a consistency check on the model, because in many cases the most recent Pco2 value available was obtained several days or more from the time of the study. When this analysis was restricted to the six infants with Pco2 values obtained within 1 day of the study, there was a close correlation (y = 0.88x+1.5, R2 = 0.99).
DISCUSSION
Series of paired values of Spo2 and PIo2 were used in preterm infants with BPD to show, non-invasively, an increase in shunt and a reduction in the VA:Q ratio. The reduced VA:Q ratio was the dominant gas exchange defect causing a major right shift of the Spo2 versus PIo2 curve in all these infants. The right shift of the curve explained the need for an increased PIo2, and there was a strong linear relationship between the degree of shift and the PIo2 required to achieve any chosen saturation in the range 86–94%. The consistency of this finding was such that a single measurement of the PIo2 required to achieve any Spo2 in the range 86–94% was sufficient to derive shift. Presently, no definition of BPD exists that provides both a robust physiological threshold for diagnosis and a continuous scale of severity that is based on the degree of gas exchange impairment. We believe that the degree of right shift of the relationship between Spo2 and PIo2 provides such a measure. This could be expressed either as the shift in kPa or as the PIo2 required to maintain a saturation of 90%. Such information has previously been derived by more invasive methods.
This non-invasive method of partitioning gas exchange impairment has been applied in sick infants,10 and in healthy and sick adults.8,9,11 The results showed a good fit between the model and the clinical data in all age groups and disease states studied. Kjaergaard et al,11 using saturation measurements non-invasively, obtained results almost identical to those obtained from simultaneous more invasive measurements. Iles and Edmunds13 showed that measures of gas exchange impairment derived from arterial blood gases sampled around term predict the prognosis of BPD, and that infants with low saturation are at higher risk of acute life-threatening events.14
The recent National Institutes of Health workshop consensus definition of BPD15 categorises infants as having no BPD, or with mild, moderate or severe BPD according to the amount of oxygen supplementation and ventilatory support required up to 36 weeks’ gestation. These categories predict later respiratory morbidity,16 but they are not physiologically based; and respiratory problems are also seen later in life in a substantial number of infants not identified to have BPD by this definition. Infants with BPD have reduced numbers of alveoli, enlarged air spaces, interstitial fibrosis and variable degrees of small airway narrowing.17 Defining the degree of physiological impairment associated with this pathology is likely to be more informative than quantifying the preceding exposure to treatment. Similar to the Walsh test,4 the National Institutes of Health network definition15 is likely to permit infants with saturations lower than those observed in healthy infants to be categorised as having no BPD. Measurement of the reduced VA:Q ratio in terms of shift enables the determination of the degree of gas exchange impairment in all infants, including those who are stable in air, and may provide a more detailed description of study outcomes and serve as a more informative baseline for studies on the prognosis of BPD.
The Walsh test4 is not really a threshold test, because many infants fail it during the 30-min observation period after having adequate saturation to begin with. In a recent study, infants with a saturation of >96% with an effective fraction of inspired oxygen <23% had a positive predictive value of 66% for passing the Walsh test.18 This reflects the fact that an oxygen saturation around 90% lies on the steep part of the dissociation curve, where reducing the PIo2 by 1% is associated with changes in saturation of ⩾2–3%, and small changes in alveolar ventilation will therefore cause considerable desaturation (fig 2). Using our method, a mean saturation value obtained at a fixed PIo2 during a brief observation period while an infant was lying supine and free from gross body movements could be used to determine whether the infant would have a saturation of 90% in air.
We have not measured the day-to-day variability of our test within patients. The accuracy of the test is dependent on the accuracy of the measurement of PIo2 and Spo2. The issue of PIo2 measurement can be eliminated if Spo2 is determined with the infant breathing air. Current Spo2 monitors are accurate to 1–3% in the range studied.19 On the steep part of the dissociation curve, changes in Spo2 of this magnitude have a small effect on shift.
What is already known on this topic
Present definitions of bronchopulmonary dysplasia have limited capacity to describe disease severity.
What this study adds
Reduced ventilation:perfusion ratio can be quantified non-invasively and may provide a simple, objective method for defining bronchopulmonary dysplasia that can grade disease severity.
The saturation values used to derive the models used in the methods described above were derived from the normal adult haemoglobin oxygen dissociation curve.20 Curves of newborn infants may differ slightly in the presence of varying amounts of fetal haemoglobin. However, by the time of our study, the infants were around 11 weeks old. Beresford et al5 showed that healthy 1-week-old and 6-month-old preterm infants have mean saturation values of around 97% in air, and Parkins et al6 showed similar values in healthy term infants at 3 months of age; so there is probably no major bias from using the normal curve in adults as a reference point for calculating shift by the time these infants reach 36 weeks’ gestation. The model assumes a fixed arteriovenous oxygen gradient of 5 ml/100 ml. Any variation in this within or between individuals affects the position of the plateau of the oxygen dissociation curve but has little effect on its shape, and should not therefore have much effect on calculations of shift.8 Similarly, estimations of shunt are more sensitive to haemoglobin level than estimations of shift.8
In conclusion, we have shown that the contribution of reduced VA:Q (shift) and shunt to impaired gas exchange can be derived easily from non-invasive measurements of Spo2 and PIo2 in infants with BPD. The degree of right shift of the Spo2 versus PIo2 curve provides a readily accessible continuous measure of the severity of gas exchange impairment due to a reduced VA:Q ratio, which is a more dominant contributor than shunt. This measure could be used to define BPD as an outcome in studies and to categorise infants in prospective studies on BPD prognosis.
REFERENCES
Footnotes
-
Published Online First 27 June 2006
-
Competing interests: None declared.
Linked Articles
- Fantoms